UNICEF Uganda End-Of-Year Humanitarian Situation Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ending CHILD MARRIAGE and TEENAGE PREGNANCY in Uganda
ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA Final Report - December 2015 ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA 1 A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA Final Report - December 2015 ACKNOWLEDGEMENTS The United Nations Children Fund (UNICEF) gratefully acknowledges the valuable contribution of many individuals whose time, expertise and ideas made this research a success. Gratitude is extended to the Research Team Lead by Dr. Florence Kyoheirwe Muhanguzi with support from Prof. Grace Bantebya Kyomuhendo and all the Research Assistants for the 10 districts for their valuable support to the research process. Lastly, UNICEF would like to acknowledge the invaluable input of all the study respondents; women, men, girls and boys and the Key Informants at national and sub national level who provided insightful information without whom the study would not have been accomplished. I ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA A FORMATIVE RESEARCH TO GUIDE THE IMPLEMENTATION OF THE NATIONAL STRATEGY ON ENDING CHILD MARRIAGE AND TEENAGE PREGNANCY IN UGANDA CONTENTS ACKNOWLEDGEMENTS ..................................................................................I -
Vulnerable and Marginalized Groups Framework (Vmgf)
VULNERABLE AND MARGINALIZED GROUPS FRAMEWORK (VMGF) FOR THE UGANDA DIGITAL ACCELERATION PROGRAM [UDAP] FPIC with The Tepeth Community in Tapac FPIC with the Batwa Community in Bundibugyo MARCH 2021 Confidential VULNERABLEV ANDULNE MARGINALISEDRABLE AND MA GROUPSRGINALIZ FRAMEWORKED GROUPS (VMGF) January 2021 2 FRAMEWORK Action Parties Designation Signature Prepared Chris OPESEN & Derrick Social Scientist & Environmental KYATEREKERA Specialist Reviewed Flavia OPIO Business Analyst Approved Vivian DDAMBYA Director Technical Services DOCUMENT NUMBER: NITA-U/2021/PLN THE NATIONAL INFORMATION TECHNOLOGY AUTHORITY, UGANDA (NITA-U) Palm Courts; Plot 7A Rotary Avenue (Former Lugogo Bypass). P.O. Box 33151, Kampala- Uganda Tel: +256-417-801041/2, Fax: +256-417-801050 Email: [email protected] Web: www.nita.go.ug The Uganda Digital Acceleration Program [UDAP) Page iii Confidential VULNERABLEV ANDULNE MARGINALISEDRABLE AND MA GROUPSRGINALIZ FRAMEWORKED GROUPS (VMGF) January 2021 2 FRAMEWORK TABLE OF CONTENTS ACRONYMS........................................................................................................................................................ vii EXECUTIVE SUMMARY ................................................................................... Error! Bookmark not defined. 1. INTRODUCTION ............................................................................................................................................. 1 1.1. Background................................................................................................................................................. -

WHO UGANDA BULLETIN February 2016 Ehealth MONTHLY BULLETIN
WHO UGANDA BULLETIN February 2016 eHEALTH MONTHLY BULLETIN Welcome to this 1st issue of the eHealth Bulletin, a production 2015 of the WHO Country Office. Disease October November December This monthly bulletin is intended to bridge the gap between the Cholera existing weekly and quarterly bulletins; focus on a one or two disease/event that featured prominently in a given month; pro- Typhoid fever mote data utilization and information sharing. Malaria This issue focuses on cholera, typhoid and malaria during the Source: Health Facility Outpatient Monthly Reports, Month of December 2015. Completeness of monthly reporting DHIS2, MoH for December 2015 was above 90% across all the four regions. Typhoid fever Distribution of Typhoid Fever During the month of December 2015, typhoid cases were reported by nearly all districts. Central region reported the highest number, with Kampala, Wakiso, Mubende and Luweero contributing to the bulk of these numbers. In the north, high numbers were reported by Gulu, Arua and Koti- do. Cholera Outbreaks of cholera were also reported by several districts, across the country. 1 Visit our website www.whouganda.org and follow us on World Health Organization, Uganda @WHOUganda WHO UGANDA eHEALTH BULLETIN February 2016 Typhoid District Cholera Kisoro District 12 Fever Kitgum District 4 169 Abim District 43 Koboko District 26 Adjumani District 5 Kole District Agago District 26 85 Kotido District 347 Alebtong District 1 Kumi District 6 502 Amolatar District 58 Kween District 45 Amudat District 11 Kyankwanzi District -

Funding Going To
% Funding going to Funding Country Name KP‐led Timeline Partner Name Sub‐awardees SNU1 PSNU MER Structural Interventions Allocated Organizations HTS_TST Quarterly stigma & discrimination HTS_TST_NEG meetings; free mental services to HTS_TST_POS KP clients; access to legal services PrEP_CURR for KP PLHIV PrEP_ELIGIBLE Centro de Orientacion e PrEP_NEW Dominican Republic $ 1,000,000.00 88.4% MOSCTHA, Esperanza y Caridad, MODEMU Region 0 Distrito Nacional Investigacion Integral (COIN) PrEP_SCREEN TX_CURR TX_NEW TX_PVLS (D) TX_PVLS (N) TX_RTT Gonaives HTS_TST KP sensitization focusing on Artibonite Saint‐Marc HTS_TST_NEG stigma & discrimination, Nord Cap‐Haitien HTS_TST_POS understanding sexual orientation Croix‐des‐Bouquets KP_PREV & gender identity, and building Leogane PrEP_CURR clinical providers' competency to PrEP_CURR_VERIFY serve KP FY19Q4‐ KOURAJ, ACESH, AJCCDS, ANAPFEH, APLCH, CHAAPES, PrEP_ELIGIBLE Haiti $ 1,000,000.00 83.2% FOSREF FY21Q2 HERITAGE, ORAH, UPLCDS PrEP_NEW Ouest PrEP_NEW_VERIFY Port‐au‐Prince PrEP_SCREEN TX_CURR TX_CURR_VERIFY TX_NEW TX_NEW_VERIFY Bomu Hospital Affiliated Sites Mombasa County Mombasa County not specified HTS_TST Kitui County Kitui County HTS_TST_NEG CHS Naishi Machakos County Machakos County HTS_TST_POS Makueni County Makueni County KP_PREV CHS Tegemeza Plus Muranga County Muranga County PrEP_CURR EGPAF Timiza Homa Bay County Homa Bay County PrEP_CURR_VERIFY Embu County Embu County PrEP_ELIGIBLE Kirinyaga County Kirinyaga County HWWK Nairobi Eastern PrEP_NEW Tharaka Nithi County Tharaka Nithi County -

Highlights of the Ebola Virus Disease Preparedness in Uganda
HIGHLIGHTS OF THE EBOLA VIRUS DISEASE PREPAREDNESS IN UGANDA 8th November 2018 (12:00 HRS) – UPDATE No 50 a) SITUATION UPDATE FROM DEMOCRATIC REPUBLIC OF CONGO FOR 7thNovember 2018, WITH DATA UP TO 6th November 2018 Cumulative cases: 308 Confirmed cases : 273 Probable : 35 Total deaths : 191 Suspect Cases under investigation : 39 Areas affected : Two provinces o North Kivu - Mabalako; Butembo; Ocha; Musienene; Beni and Bingo o Ituri- Mambasa, Mandina, Tchomia Health and front line workers vaccinated Security concerns limiting contact tracing. b) EVD SITUATIONAL UPDATE IN UGANDA There is NO confirmed EVD case in Uganda. Active case search continues in all communities, health facilities and on formal and informal border crossing in all districts especially in the high risk ones. Alert cases continue to be picked, isolated, treated and blood samples picked for testing by the Uganda Virus Research Institute (UVRI). The alerts are highlighted in the specific district reports below under the Surveillance section. Vaccination of frontline health workers started on 7th November, 2018 and will cover the five high-risk districts of Bundibugyo, Kaseses, Bunyangabu, Kabarole and Ntoroko. 1 2 c) PREPAREDNESS ACTIVITIES IN THE FIELD AND NATIONAL (PROGRESS AND GAPS) VACCINATION Vaccination of frontline health workers started on 7th November 2018 in Ntoroko district without any incident. Twenty (26) targeted health care/frontline workers at Karugutu HC IV, Stella Maris Ntoro HC III and Rwebisengo HC IV were vaccinated. There is high demand for the vaccine in the district MoH and WHO are going to increase the number of vaccination teams to meet the demand. Over the weekend, 4 teams with 12 members each will be trained. -
Tooro Kingdom 2 2
ClT / CIH /ITH 111111111111111111111111111111111111111111111111111111111111 0090400007 I Le I 09 MAl 2012 NOMINATION OF EMPAAKO TRADITION FOR W~~.~.Q~~}~~~~.P?JIPNON THE LIST OF INTANGIBLE CULTURAL HERITAGE IN NEED OF URGENT SAFEGUARDING 2012 DOCUMENTS OF REQUEST FROM STAKEHOLDERS Documents Pages 1. Letter of request form Tooro Kingdom 2 2. Letter of request from Bunyoro Kitara Kingdom 3 3. Statement of request from Banyabindi Community 4 4. Statement of request from Batagwenda Community 9 5. Minute extracts /resolutions from local government councils a) Kyenjojo District counciL 18 b) Kabarole District Council 19 c) Kyegegwa District Council 20 d) Ntoroko District Council 21 e) Kamwenge District Council 22 6. Statement of request from Area Member of Ugandan Parliament 23 7. Letters of request from institutions, NOO's, Associations & Companies a) Kabarole Research & Resource Centre 24 b) Mountains of the Moon University 25 c) Human Rights & Democracy Link 28 d) Rural Association Development Network 29 e) Modrug Uganda Association Ltd 34 f) Runyoro - Rutooro Foundation 38 g) Joint Effort to Save the Environment (JESE) .40 h) Foundation for Rural Development (FORUD) .41 i) Centre of African Christian Studies (CACISA) 42 j) Voice of Tooro FM 101 43 k) Better FM 44 1) Tooro Elders Forum (Isaazi) 46 m) Kibasi Elders Association 48 n) DAJ Communication Ltd 50 0) Elder Adonia Bafaaki Apuuli (Aged 94) 51 8. Statements of Area Senior Cultural Artists a) Kiganlbo Araali 52 b) Master Kalezi Atwoki 53 9. Request Statement from Students & Youth Associations a) St. Leo's College Kyegobe Student Cultural Association 54 b) Fort Portal Institute of Commerce Student's Cultural Association 57 c) Fort Portal School of Clinical Officers Banyoro, Batooro Union 59 10. -

A Participatory Gender Analysis
·•·· ~ Save the ' ICRWINTERNATIONAL CENTER \aI Children. FOR RESEARCH ON WOMEN PASSION. PROOF. POWER. A PARTICIPATORY GENDER ANALYSIS For identifying discriminatory household and community norms and practices preventing young women from participating equally in agriculture in Kasese and Ntoroko districts of Western Uganda FINAL REPORT-FEBRUARY 2020 IDRC I CRDI I ntematfami D!!W!lopment Research Cen~re Cen~re d'e reaherclles pour le developpement fntematfona Cana d .•.a List of Acronyms and Abbreviations DCDO: District Community Development Officers CDO: Community Development Officer FGD: Focus Group Discussions GA: Gender Assessment ICF: Informed Consent Form ICRW: International Center for Research on Women IDRC: International Development Research Center IRB: Institutional Review Board KII: Key Informant Interviews LC: Local Council MUREC: Mildmay Uganda Research Ethics Committee OWC: Operation Wealth Creation SBCC: Social behavior change communication SC: Save the Children SCDO: Sub County Community Development Officers. UNCST: Uganda National Council of Science and Technology YiA: Youth in Action YiA+: Youth in Action Plus YLP: Youth Livelihoods Program Page | 1 Table of Contents List of Acronyms and Abbreviations ........................................................................................... 1 Executive summary……. ............................................................................................................ 5 Introduction…………… .......................................................................................................... -

STATUTORY INSTRUMENTS SUPPLEMENT No. 5 3Rd February
STATUTORY INSTRUMENTS SUPPLEMENT No. 5 3rd February, 2012 STATUTORY INSTRUMENTS SUPPLEMENT to The Uganda Gazette No. 7 Volume CV dated 3rd February, 2012 Printed by UPPC, Entebbe, by Order of the Government. STATUTORY INSTRUMENTS 2012 No. 5. The Local Government (Declaration of Towns) Regulations, 2012. (Under sections 7(3) and 175(1) of the Local Governments Act, Cap. 243) In exercise of the powers conferred upon the Minister responsible for local governments by sections 7(3) and 175(1) of the Local Governments Act, in consultation with the districts and with the approval of Cabinet, these Regulations are made this 14th day of July, 2011. 1. Title These Regulations may be cited as the Local Governments (Declaration of Towns) Regulations, 2012. 2. Declaration of Towns The following areas are declared to be towns— (a) Amudat - consisting of Amudat trading centre in Amudat District; (b) Buikwe - consisting of Buikwe Parish in Buikwe District; (c) Buyende - consisting of Buyende Parish in Buyende District; (d) Kyegegwa - consisting of Kyegegwa Town Board in Kyegegwa District; (e) Lamwo - consisting of Lamwo Town Board in Lamwo District; - consisting of Otuke Town Board in (f) Otuke Otuke District; (g) Zombo - consisting of Zombo Town Board in Zombo District; 259 (h) Alebtong (i) Bulambuli (j) Buvuma (k) Kanoni (l) Butemba (m) Kiryandongo (n) Agago (o) Kibuuku (p) Luuka (q) Namayingo (r) Serere (s) Maracha (t) Bukomansimbi (u) Kalungu (v) Gombe (w) Lwengo (x) Kibingo (y) Nsiika (z) Ngora consisting of Alebtong Town board in Alebtong District; -
Koica Program Baseline Survey 2015 Report
KOICA PROGRAM BASELINE SURVEY 2015 REPORT Baseline Survey for KOICA Program in Uganda 2016 THE REPUBLIC OF UGANDA UGANDA BUREAU OFSTATISTICS BASELINE SURVEY FOR KOICA PROGRAM2015 Uganda Bureau of Statistics Colville Street, Plot 9 P.O. Box 7186, Kampala Tel: 0414-320740, 0772 705127 Fax: 0414-237 553 August 2016 E-mail: [email protected] Website: www.ubos.org 1 Baseline Survey for KOICA Program in Uganda 2016 LIST OF ACRONYMS ANC Antenatal Care EA Enumeration Areas EmOC Emergency Obstetric Care HC Health Centre KOICA Korea International Cooperation Agency M&E Monitoring and Evaluation MNCH Maternal New-born and Child Health PNC Post-natal Care PPS Probability Proportional to Size UBOS Uganda Bureau of Statistics UNICEF United Nations Children’s Fund UPHC Uganda Population and Housing Census VHTs Village Health Teams 2 Baseline Survey for KOICA Program in Uganda 2016 TABLE OF CONTENTS TABLE OF CONTENTS ............................................................................................................... 3 LIST OF TABLES ......................................................................................................................... 5 EXECUTIVE SUMMARY .......................................................... ERROR! BOOKMARK NOT DEFINED. 1 CHAPTER ONE .................................................................................................................... 9 INTRODUCTION ................................................................................................................................ 9 1.1 BACKGROUND -

Maternal Health Ntoroko
MATERNAL HEALTH NTOROKO In Uganda, maternal mortality remains high at 440 maternal deaths per 100,000 live births. For every maternal death in Uganda, at least six survive with chronic and debilitating ill health. Most maternal deaths are due to causes directly related to pregnancy and childbirth unsafe abortion and obstetric complications such as severe bleeding, infection, hypertensive disorders, and obstructed labour1. According to the State of Worlds’ Children WHO, declines in maternal mortality have been registered in Uganda. a review of emergency obstetric care (EOC) facilities showed that in 54 districts out of 56 EOC’s throughout the country, over 97 % of facilities that expected to provide basic emergency services were not able to do so. Among the key impediments to service delivery were Lack of running water, electricity, and functioning operating theatres. Further reviews are urgently required to ensure that existing facilities are upgraded and new ones are established in a sustainable manner. Funding for medical supplies, including essential medicines, is a further priority. The UN inter-agency list of essential medicines for reproductive health serves as a useful guide to the minimum number of effective, cost saving drugs that should be available.2 FIGURE 1, POPULATION IN NTOROKO Ntoroko district is in the Rwenzururu (aka Rwenzori) sub-region located approximately 300 kilometres (190 mi), by road, west of Kampala and has an estimated population of 84,100 (2012). There are three subcounties – Kanara, Karugutu and Rwebisengo, which include 10 parishes and 56 villages. Cities nearby include Kijura, Ntoroko, Ndaiga, Fort Portal, Yenga, Bundibugyo, Kikorba, Bugado, and Kyenjojo. -

Oil Industry in Uganda: the Socio-Economic Effects on the People of Kabaale Village, Hoima, and Bunyoro Region in Uganda
Syracuse University SURFACE Dissertations - ALL SURFACE 8-1-2016 Oil Industry in Uganda: The Socio-economic Effects on the People of Kabaale Village, Hoima, and Bunyoro Region in Uganda MIRIAM KYOMUGASHO Syracuse University Follow this and additional works at: https://surface.syr.edu/etd Part of the Social and Behavioral Sciences Commons Recommended Citation KYOMUGASHO, MIRIAM, "Oil Industry in Uganda: The Socio-economic Effects on the People of Kabaale Village, Hoima, and Bunyoro Region in Uganda" (2016). Dissertations - ALL. 613. https://surface.syr.edu/etd/613 This Thesis is brought to you for free and open access by the SURFACE at SURFACE. It has been accepted for inclusion in Dissertations - ALL by an authorized administrator of SURFACE. For more information, please contact [email protected]. ABSTRACT This thesis examines the socio-economic effects of oil industry on the people of Kabaale Village, Hoima, and Bunyoro region in Uganda. The thesis analyses the current political economy of Uganda and how Uganda is prepared to utilize the proceeds from the oil industry for the development of the country and its people. In addition, the research examines the effects of industry on the people of Uganda by analyzing how the people of Kabaale in Bunyoro region were affected by the plans to construct oil refinery in their region. This field research was done using qualitative methods and the Historical Materialism theoretical framework guided the study. The major findings include; displacement of people from land especially women, lack of accountability from the leadership, and less citizen participation in the policy formulation and oil industry. -
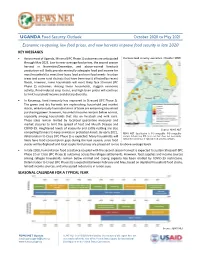
1Boctober 2020 to May 2021
UGANDA Food Security Outlook October 2020 to May 2021 Economic re-opening, low food prices, and new harvests improve food security in late 2020 KEY MESSAGES • Across most of Uganda, Minimal (IPC Phase 1) outcomes are anticipated Current food security outcomes, October 2020 through May 2021. Low to near-average food prices, the second season harvest in November/December, and above-normal livestock production will likely provide minimally adequate food and income for most household to meet their basic food and non-food needs. In urban areas and some rural districts that have been worst affected by recent floods, however, some households will most likely face Stressed (IPC Phase 2) outcomes. Among these households, sluggish economic activity, flood-induced crop losses, and high bean prices will continue to limit household income and dietary diversity. • In Karamoja, food insecurity has improved to Stressed (IPC Phase 2). The green and dry harvests are replenishing household and market stocks, while broadly favorable terms of trade are enhancing household purchasing power. However, household income remains below normal, especially among households that rely on livestock and milk sales. These sales remain limited by localized quarantine measures and market closures to limit the spread of Foot and Mouth Disease and COVID-19. Heightened levels of insecurity and cattle rustling are also Source: FEWS NET compelling farmers to keep animals in protected kraals. By early 2021, FEWS NET classification is IPC-compatible. IPC-compatible deterioration to Crisis (IPC Phase 3) is expected. Many households will analysis follows key IPC protocols but does not necessarily likely have food consumption gaps during the lean season, since food reflect the consensus of national food security partners.