JARDIANCE (Empagliflozin)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treatment of Diabetes Mellitus
TREATMENT OF DIABETES MELLITUS DIABETES is a condition that affects how the body makes energy from food. Food is broken down into sugar (glucose) in the body and released into the blood. When the blood sugar level rises after a meal, insulin responds to let the sugar into the cells to be used as energy. In diabetes, the body either does not make enough insulin or it stops responding to insulin as well as it should. This results in sugar staying in the blood and leads to serious health problems over time. DIAGNOSIS OF DIABETES1 • A1C Test: Lab test measuring average blood sugar over past two to three months • Fasting Blood Sugar Test: Lab test measuring blood sugar after eight hours of no food or drink • Oral Glucose Tolerance Test (OGTT): Measures blood sugar before and two hours after drinking a specific sugary liquid • Random Blood Sugar Test: Measures blood sugar at a moment in time, without any kind of preparation (like fasting) FASTING BLOOD ORAL GLUCOSE TOLERANCE RANDOM BLOOD RESULT A1C TEST SUGAR TEST TEST SUGAR TEST Diabetes ≥ 6.5% ≥126 mg/dL ≥ 200 mg/dL ≥ 200 mg/dL Prediabetes 5.7 – 6.4% 100 – 125 mg/dL 140 – 199 mg/dL N/A Normal < 5.7% ≤99 mg/dL < 140 mg/dL N/A NON-DRUG TREATMENTS2 THERAPY COST WHAT TO EXPECT Diet (Mediterranean diet) and exercise (30 minutes a day, five days a week of moderate- Weight loss $-$$ intensity exercise); 7% weight loss decreases risk of diabetes3 Psychological intervention $$-$$$ Psychotherapy may reduce diabetic distress and improve glycemic control4,5 nationalcooperativerx.com PRESCRIPTION TREATMENTS -

Therapeutic Medications Against Diabetes: What We Have and What We Expect
Advanced Drug Delivery Reviews 139 (2019) 3–15 Contents lists available at ScienceDirect Advanced Drug Delivery Reviews journal homepage: www.elsevier.com/locate/addr Therapeutic medications against diabetes: What we have and what we expect Cheng Hu a,b, Weiping Jia a,⁎ a Shanghai Diabetes Institute, Shanghai Key Laboratory of Diabetes Mellitus, Shanghai Key Clinical Center for Metabolic Diseases, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, 600 Yishan Road, Shanghai 200233, People's Republic of China b Shanghai Jiao Tong University Affiliated Sixth People's Hospital South Campus, 6600 Nanfeng Road, Shanghai 200433, People's Republic of China article info abstract Article history: Diabetes has become one of the largest global health and economic burdens, with its increased prevalence and Received 28 June 2018 high complication ratio. Stable and satisfactory blood glucose control are vital to reduce diabetes-related compli- Received in revised form 1 September 2018 cations. Therefore, continuous attempts have been made in antidiabetic drugs, treatment routes, and traditional Accepted 27 November 2018 Chinese medicine to achieve better disease control. New antidiabetic drugs and appropriate combinations of Available online 5 December 2018 these drugs have increased diabetes control significantly. Besides, novel treatment routes including oral antidia- betic peptide delivery, nanocarrier delivery system, implantable drug delivery system are also pivotal for diabetes Keywords: fi Diabetes control, with its greater ef ciency, increased bioavailability, decreased toxicity and reduced dosing frequency. Treatment Among these new routes, nanotechnology, artificial pancreas and islet cell implantation have shown great poten- Drug delivery tial in diabetes therapy. Traditional Chinese medicine also offer new options for diabetes treatment. -

Step Therapy
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2020 P 3086-9 Program Step Therapy – Diabetes Medications - SGLT2 Inhibitors Medication Farxiga (dapagliflozin)*, Glyxambi (empagliflozin/linagliptan), Invokana (canagliflozin)*, Invokamet (canagliflozin/metformin)*, Invokamet XR (canaglifloxin/metformin extended-release)*, Jardiance (empagliflozin), Qtern (dapagliflozin/saxagliptin)*, Segluromet (ertugliflozin/metformin)*, Steglatro (ertugliflozin)*, Steglujan (ertugliflozin/sitagliptin)*, Xigduo XR (dapagliflozin/metformin extended-release)* P&T Approval Date 10/2016, 10/2017, 4/2018, 8/2018, 12/2018, 2/2019, 2/2020, 5/2020; 7/2020 Effective Date 10/1/2020; Oxford only: 10/1/2020 1. Background: Farxiga (dapagliflozin)*, Invokana (canagliflozin)*, Jardiance (empagliflozin) and Steglatro (ertugliflozin)* are sodium-glucose co-transporter 2 (SGLT2) inhibitors indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. Farxiga*, Invokana* and Jardiance have additional indications. Farxiga* is indicated to reduce the risk of cardiovascular death and hospitalization for heart failure in adults with heart failure (NYHA class II-IV) with reduced ejection fraction. Invokana* is indicated to reduce the risk of major adverse cardiovascular events (cardiovascular death, nonfatal myocardial infarction and nonfatal stroke) in adults with type 2 diabetes mellitus and established cardiovascular disease (CVD), and to reduce the risk of end-stage kidney disease (ESKD), doubling of -
Protocol for Non-Interventional Studies Based on Existing Data
ABCD TITLE PAGE Protocol for non-interventional studies based on existing data TITLE PAGE Note: This template complies with the European Medicines Agency requirements on format, layout and content of a Post Authorisation safety Study (PASS) protocol of 26 Sep 2012. Please do not change structure provided in this template. Document Number: <document number> BI Study Number: <Study Number> BI Investigational Empagliflozin (Jardiance®) Product(s): Empagliflozin + Linagliptin (Glyxambi®) Empagliflozin + Metformin (Synjardy®) Title: Cardiovascular outcomes and mortality in Danish patients with type 2 diabetes who initiate empagliflozin versus liraglutide as second-line therapy: A Danish nationwide comparative effectiveness study Protocol version 1.0 identifier: Date of last version of 15JUL2018 protocol: PASS: No EU PAS register If applicable: Registration number in the EU PAS register; number: indicate “Study not registered” if the study has not been registered in the EU PAS register Active substance: A10BX12 Empagliflozin A10BK03 Empagliflozin A10BD19 Empagliflozin + Linagliptin A10BD20 Empagliflozin + Metformin A10BX07 Liraglutide A10BJ02 Liraglutide A10AE56 Insulin degludec + Liraglutide Medicinal product: Jardiance Glyxambi Synjardy Victoza Xultophy Product reference: Reference number(s) of centrally authorised products and/or, if possible, of nationally authorised products subject to the study 001-MCS-90-124_RD-01 (4.0) Boehringer Ingelheim Page 2 of 55 Protocol for non-interventional studies based on existing data BI Study Number <Study Number> <document number> Proprietary confidential information © 2019 Boehringer Ingelheim International GmbH or one or more of its affiliated companies Procedure number: If applicable, Agency or national procedure number(s), e.g. EMA/X/X/XXX Joint PASS: No Research question and To compare, among patients with type 2 diabetes in Denmark, objectives: clinical outcomes among new users (initiators) of empagliflozin versus liraglutide. -

The Sodium Glucose Cotransporter Type 2 Inhibitor Empagliflozin Preserves B-Cell Mass and Restores Glucose Homeostasis in the Male Zucker Diabetic Fatty Rat
1521-0103/350/3/657–664$25.00 http://dx.doi.org/10.1124/jpet.114.213454 THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS J Pharmacol Exp Ther 350:657–664, September 2014 Copyright ª 2014 by The American Society for Pharmacology and Experimental Therapeutics The Sodium Glucose Cotransporter Type 2 Inhibitor Empagliflozin Preserves b-Cell Mass and Restores Glucose Homeostasis in the Male Zucker Diabetic Fatty Rat Henrik H. Hansen, Jacob Jelsing, Carl Frederik Hansen, Gitte Hansen, Niels Vrang, Michael Mark, Thomas Klein, and Eric Mayoux Gubra, Hørsholm, Denmark (H.H.H., J.J., C.F.H., G.H., N.V.); and Boehringer Ingelheim Pharma, Biberach, Germany (M.M., T.K., E.M.) Received January 22, 2014; accepted July 2, 2014 Downloaded from ABSTRACT Type 2 diabetes is characterized by impaired b-cell function at week 8 of treatment compared with week 4, those of empagliflozin associated with progressive reduction of insulin secretion and remained stable throughout the study period. Similarly, empagliflozin b -cell mass. Evidently, there is an unmet need for treatments improved glucose tolerance and preserved insulin secretion jpet.aspetjournals.org with greater sustainability in b-cell protection and antidiabetic after both 4 and 8 weeks of treatment. These effects were efficacy. Through an insulin and b cell–independent mechanism, reflected by less reduction in b-cell mass with empagliflozin or empagliflozin, a specific sodium glucose cotransporter type 2 liraglutide at week 4, whereas only empagliflozin showed b-cell (SGLT-2) inhibitor, may potentially provide longer efficacy. This sparing effects also at week 8. Although this study cannot be study compared the antidiabetic durability of empagliflozin treat- used to dissociate the absolute antidiabetic efficacy among ment (10 mg/kg p.o.) against glibenclamide (3 mg/kg p.o.) and the different mechanisms of drug action, the study demon- liraglutide (0.2 mg/kg s.c.) on deficient glucose homeostasis and strates that empagliflozin exerts a more sustained improve- b-cell function in Zucker diabetic fatty (ZDF) rats. -

AACE Annual Meeting 2021 Abstracts Editorial Board
June 2021 Volume 27, Number 6S AACE Annual Meeting 2021 Abstracts Editorial board Editor-in-Chief Pauline M. Camacho, MD, FACE Suleiman Mustafa-Kutana, BSC, MB, CHB, MSC Maywood, Illinois, United States Boston, Massachusetts, United States Vin Tangpricha, MD, PhD, FACE Atlanta, Georgia, United States Andrea Coviello, MD, MSE, MMCi Karel Pacak, MD, PhD, DSc Durham, North Carolina, United States Bethesda, Maryland, United States Associate Editors Natalie E. Cusano, MD, MS Amanda Powell, MD Maria Papaleontiou, MD New York, New York, United States Boston, Massachusetts, United States Ann Arbor, Michigan, United States Tobias Else, MD Gregory Randolph, MD Melissa Putman, MD Ann Arbor, Michigan, United States Boston, Massachusetts, United States Boston, Massachusetts, United States Vahab Fatourechi, MD Daniel J. Rubin, MD, MSc Harold Rosen, MD Rochester, Minnesota, United States Philadelphia, Pennsylvania, United States Boston, Massachusetts, United States Ruth Freeman, MD Joshua D. Safer, MD Nicholas Tritos, MD, DS, FACP, FACE New York, New York, United States New York, New York, United States Boston, Massachusetts, United States Rajesh K. Garg, MD Pankaj Shah, MD Boston, Massachusetts, United States Staff Rochester, Minnesota, United States Eliza B. Geer, MD Joseph L. Shaker, MD Paul A. Markowski New York, New York, United States Milwaukee, Wisconsin, United States CEO Roma Gianchandani, MD Lance Sloan, MD, MS Elizabeth Lepkowski Ann Arbor, Michigan, United States Lufkin, Texas, United States Chief Learning Officer Martin M. Grajower, MD, FACP, FACE Takara L. Stanley, MD Lori Clawges The Bronx, New York, United States Boston, Massachusetts, United States Senior Managing Editor Allen S. Ho, MD Devin Steenkamp, MD Corrie Williams Los Angeles, California, United States Boston, Massachusetts, United States Peer Review Manager Michael F. -

PRESCRIBING INFORMATION ------WARNINGS and PRECAUTIONS------These Highlights Do Not Include All the Information Needed to Use JARDIANCE Safely and Effectively
HIGHLIGHTS OF PRESCRIBING INFORMATION -----------------------WARNINGS AND PRECAUTIONS------------------------ These highlights do not include all the information needed to use JARDIANCE safely and effectively. See full prescribing information for Ketoacidosis: Assess patients who present with signs and symptoms of JARDIANCE. metabolic acidosis for ketoacidosis, regardless of blood glucose level. If suspected, discontinue JARDIANCE, evaluate and treat promptly. JARDIANCE® (empagliflozin tablets), for oral use Before initiating JARDIANCE, consider risk factors for ketoacidosis. Initial U.S. Approval: 2014 Patients on JARDIANCE may require monitoring and temporary discontinuation of therapy in clinical situations known to predispose to ---------------------------RECENT MAJOR CHANGES--------------------------- ketoacidosis. (5.1) Volume Depletion: Before initiating JARDIANCE, assess volume status Indications and Usage (1) 8/2021 and renal function in patients with impaired renal function, elderly Dosage and Administration (2.1) 6/2021 patients, or patients on loop diuretics. Monitor for signs and symptoms Dosage and Administration (2.2) 8/2021 during therapy. (5.2, 6.1) Dosage and Administration (2.3) – Removed 8/2021 Urosepsis and Pyelonephritis: Evaluate patients for signs and symptoms Contraindications (4) 6/2021 of urinary tract infections and treat promptly, if indicated (5.3) Warnings and Precautions (5.1, 5.2) 6/2021 Hypoglycemia: Consider lowering the dose of insulin secretagogue or Warnings and Precautions (5.3, 5.5) 8/2021 insulin to reduce the risk of hypoglycemia when initiating JARDIANCE Warnings and Precautions (5.9) – Removed 6/2021 (5.4) ----------------------------INDICATIONS AND USAGE--------------------------- Necrotizing Fasciitis of the Perineum (Fournier’s Gangrene): Serious, JARDIANCE is a sodium-glucose co-transporter 2 (SGLT2) inhibitor life-threatening cases have occurred in both females and males. -

Clinical Pharmacology Biopharmaceutics Review(S)
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 206111Orig1s000 CLINICAL PHARMACOLOGY AND BIOPHARMACEUTICS REVIEW(S) (b) Q=(4) % at 20 minutes for empagliflozin and metformin HCl Review: The Biopharmaceutics review is focused on the evaluation and acceptability of the bioequivalence and dissolution data to support approvability of the proposed FDC tablets. RECOMMENDATION: The bioequivalence results and dissolution method are acceptable. From the Biopharmaceutics perspective, NDA 206111 for Empagliflozin/Metformin Hydrochloride Fixed Dose Combination Tablets is recommended for approval. Signature Signature Digitally signed by Kelly M. Kitchens -S Digitally signed by Tapash K. Ghosh -S DN: c=US, o=U.S. Government, DN: c=US, o=U.S. Government, ou=HHS, Kelly M. Tapash K. ou=FDA, ou=People, ou=HHS, ou=FDA, ou=People, 0.9.2342.19200300.100.1.1=200033657 0.9.2342.19200300.100.1.1=1300148262 , cn=Tapash K. Ghosh -S 4, cn=Kelly M. Kitchens -S Date: 2015.04.15 16:19:26 -04'00' Kitchens -S Date: 2015.04.15 15:55:42 -04'00' Ghosh -S Kelly M. Kitchens, Ph.D. Tapash Ghosh, Ph.D. Acting Biopharmaceutics Lead Acting Biopharmaceutics Branch Chief Office of New Drug Products Office of New Drug Products cc. PSeo. 4 Bioequivalence Study No. 1276.6 8 9 Bioanalytical Results: Analyte Name: Empagliflozin Parameter Standard Curve Samples Concentration (nmol/mL) 1.11 2.22 111 55.4 222 665 998 1110 Inter day Precision 7.5 5.2 2.8 2.3 2.2 2.2 2.6 1.7 (%CV) Inter day Accuracy -0.8 0.6 1.0 0.3 -1.7 0.4 -0.2 0.1 (%bias) Linearity 0.994576 – 0.999437 (range -

G Protein-Coupled Receptors
S.P.H. Alexander et al. The Concise Guide to PHARMACOLOGY 2015/16: G protein-coupled receptors. British Journal of Pharmacology (2015) 172, 5744–5869 THE CONCISE GUIDE TO PHARMACOLOGY 2015/16: G protein-coupled receptors Stephen PH Alexander1, Anthony P Davenport2, Eamonn Kelly3, Neil Marrion3, John A Peters4, Helen E Benson5, Elena Faccenda5, Adam J Pawson5, Joanna L Sharman5, Christopher Southan5, Jamie A Davies5 and CGTP Collaborators 1School of Biomedical Sciences, University of Nottingham Medical School, Nottingham, NG7 2UH, UK, 2Clinical Pharmacology Unit, University of Cambridge, Cambridge, CB2 0QQ, UK, 3School of Physiology and Pharmacology, University of Bristol, Bristol, BS8 1TD, UK, 4Neuroscience Division, Medical Education Institute, Ninewells Hospital and Medical School, University of Dundee, Dundee, DD1 9SY, UK, 5Centre for Integrative Physiology, University of Edinburgh, Edinburgh, EH8 9XD, UK Abstract The Concise Guide to PHARMACOLOGY 2015/16 provides concise overviews of the key properties of over 1750 human drug targets with their pharmacology, plus links to an open access knowledgebase of drug targets and their ligands (www.guidetopharmacology.org), which provides more detailed views of target and ligand properties. The full contents can be found at http://onlinelibrary.wiley.com/doi/ 10.1111/bph.13348/full. G protein-coupled receptors are one of the eight major pharmacological targets into which the Guide is divided, with the others being: ligand-gated ion channels, voltage-gated ion channels, other ion channels, nuclear hormone receptors, catalytic receptors, enzymes and transporters. These are presented with nomenclature guidance and summary information on the best available pharmacological tools, alongside key references and suggestions for further reading. -

SGLT2) Inhibitors (Gliflozins) in Adults with Type 2 Diabetes (T2DM
Sodium-glucose cotransporter-2 (SGLT2) inhibitors (Gliflozins) in Adults with Type 2 Diabetes (T2DM) There are currently four SGLT2 inhibitors (canagliflozin, dapagliflozin, empagliflozin and ertugliflozin) licensed in the UK for the management of adults with T2DM. No head to head trials between the SGLT2 inhibitors have been conducted. As at December 2019, clinical outcome data is available for three of the four SGLT2 inhibitors around their cardiovascular effects in people with T2DM. Ertugliflozin is still to report on this data. This document summarises the key prescribing considerations. NICE Technology Appraisal Recommendation NICE makes recommendations for when SGLT2 inhibitors can be considered in adults with T2DM; Hertfordshire Medicines Management Committee Recommendations are in line with NICE guidance: Monotherapy NICE TA 390: Canagliflozin, Dapagliflozin and Empagliflozin and NICE TA 572: Ertugliflozin as monotherapies for treating T2DM Monotherapy recommended as option in adults for whom metformin is contraindicated or not tolerated and when diet & exercise alone do not provide adequate glycaemic control, only if: •a DPP‑4 inhibitor would otherwise be prescribed and •a sulfonylurea or pioglitazone is not appropriate. Dual therapy NICE TA 315: Canagliflozin, NICE TA288: Dapagliflozin, TA 336: Empagliflozin, TA 572: Ertugliflozin as combination therapies for treating T2DM In a dual therapy regimen in combination with metformin is recommended as an option, only if: •a sulfonylurea is contraindicated or not tolerated or •the person is at significant risk of hypoglycaemia or its consequences. In combination with insulin NICE TA 315: Canagliflozin, NICE TA288: Dapagliflozin, TA 336: Empagliflozin in combination with insulin with or without other antidiabetic drugs is recommended as an option. -

204629Orig1s000
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 204629Orig1s000 RISK ASSESSMENT and RISK MITIGATION REVIEW(S) Department of Health and Human Services Public Health Service Food and Drug Administration Center for Drug Evaluation and Research Office of Surveillance and Epidemiology Office of Medication Error Prevention and Risk Management Risk Evaluation and Mitigation Strategy (REMS) Review Date: July 28, 2014 Reviewer(s): Amarilys Vega, M.D., M.P.H, Medical Officer Division of Risk Management (DRISK) Team Leader: Doris Auth, Pharm.D, Team Leader DRISK Division Director Cynthia LaCivita, Pharm.D, Acting Director DRISK Subject: Evaluation of need for a REMS Drug Name(s): Empagliflozin (Jardiance®) Therapeutic Class: Sodium-dependent glucose co-transporter-2 (SGLT2) inhibitor Dosage and Route: 10 mg, 25 mg tablet once daily/oral Application Type/Number: NDA 204629 Submission Number: Resubmission, June 3, 2014 (0032) Applicant/sponsor: Boehringer Ingelheim Pharmaceuticals, Inc. OSE RCM #: 2013-619 and 2013-656 *** This document contains proprietary and confidential information *** that should not be released to the public Reference ID: 3600276 1 INTRODUCTION This review documents the Division of Risk Management’s (DRISK) evaluation of whether a Risk Evaluation and Mitigation Strategy (REMS) is necessary for empagliflozin (NDA 204629). Boehringer Ingelheim Pharmaceuticals, Inc. is seeking approval for empagliflozin as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus (T2DM). DRISK reviewed the original application for empagliflozin submitted to FDA on March 5, 2013 and determined that a REMS was not required to manage the serious risks associated to empagliflozin (e.g., hypoglycemia, volume depletion, and genital infections). -
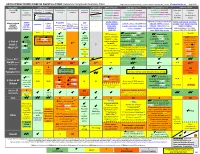
ANTI-HYPERGLYCEMIC DIABETES AGENTS in T2DM: Color Outcomes Comparison Summary Table
ANTI-HYPERGLYCEMIC DIABETES AGENTS in T2DM: Outcomes Comparison Summary Table L Regier BSP BA, M LeBras PharmD, T Trischuk PharmD, J Bareham BSP, L Lu BSP © www.RxFiles.ca Aug 2021 Drug Class Sulfonylureas TZDs Meglitinides DPP4 Inhibitors GLP1 Agonists *** SGLT2 Inhibitors *** Insulin in T2DM Generic Metformin Gliclazide Glyburide Pioglitazone Rosiglitazone Acarbose Repaglinide Saxagliptin ONGLYZA Liraglutide VICTOZA Empagliflozin JARDIANCE Intensity: Intensity: BRAND (MF) DIAMICRON DIABETA ACTOS, g AVANDIA GLUCOBAY GLUCONORM Sitagliptin JANUVIA Exenatide BYETTA, BYDUREON Canagliflozin INVOKANA Less More GLUCOPHAGE Dulaglutide TRULICITY Dapagliflozin FORXIGA, FARXIGA Alogliptin NESINA (e.g. NPH (Multiple daily GLUCOTROL D/C STEGLATRO Glipizide Nateglinide Semaglutide OZEMPIC, RYBELSUS (PO) Ertugliflozin Linagliptin TRAJENTA HS + MF) doses) STARLIX D/C SPREAD-DIMCAD] Lixisenatide ADLYXINE; ALBIGLUTIDE D/C SAVOR-TIMI 53, EMPA-REG, CANVAS, CREDENCE, T2DM: UKPDS-33,80; ADVANCE, Major trials to UKPDS- ProACTIVE ACE 33,34,80 UKPDS- Meta-analysis. TECOS, EXAMINE LEADER, EXSCEL, FREEDOM CVO, DECLARE, VERTIS-CV (2020), ACCORD, VADT, ORIGIN, DEVOTE support ADVANCE (Prevention (ADOPT; 33,80 Ferwana M. Meta- RECORD interim, PROLOGUE, REWIND, SUSTAIN-6, PIONEER-6, DAPA-HF, DAPA-CKD (2020), T1DM: DCCT/EDIC findings/ analysis 2013. trial: Stop- - some use in (ADOPT) ADOPT, DREAM CARMELINA, EMPEROR-Reduced & -Preserved (Also Boussageon et al. Meta- Outcomes* ADVANCE) SR-Liao 2017; IRIS NIDDM) ELIXA, HARMONY CAROLINA (2020), EMPA-Kidney (2022) analysis.