Integrated Nutrition and Mortality Smart Survey
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Rethinking the Somali State
Rethinking the Somali State MPP Professional Paper In Partial Fulfillment of the Master of Public Policy Degree Requirements The Hubert H. Humphrey School of Public Affairs The University of Minnesota Aman H.D. Obsiye May 2017 Signature below of Paper Supervisor certifies successful completion of oral presentation and completion of final written version: _________________________________ ____________________ ___________________ Dr. Mary Curtin, Diplomat in Residence Date, oral presentation Date, paper completion Paper Supervisor ________________________________________ ___________________ Steven Andreasen, Lecturer Date Second Committee Member Signature of Second Committee Member, certifying successful completion of professional paper Table of Contents Introduction ........................................................................................................................... 3 Methodology .......................................................................................................................... 5 The Somali Clan System .......................................................................................................... 6 The Colonial Era ..................................................................................................................... 9 British Somaliland Protectorate ................................................................................................. 9 Somalia Italiana and the United Nations Trusteeship .............................................................. 14 Colonial -

COVID-19 Update
Series: 03 MINISTRY OF PLANNING, INVESTMENT AND Somalia as of 23rd June ECONOMIC DEVELOPMENT MINISTRY OF PLANNING, INVESTMENT AND 2020 COVID-19 cases: 2835 Directorate of National Statistics ECONOMIC DEVELOPMENT Deaths: 90 Directorate of National Statistics Recoveries: 829 Recoveries: 486 Number of confirmed cases per state: Somaliland: 682 Puntland: 282 Hiirshabelle: 24 CORONOVIRUS (COVID-19) Update South West: 142 Reported period 10th June – 23rf June, 2020 Galmudug: 118 Jubaland: 176 Benadir: 1411 Key Summary Indicators There are 2835 confirmed cases in Somalia with 90 deaths and 829 recoveries 50% of the confirmed COVID 19 cases in the country are in Benadir Regional Administration 72% of the confirmed COVID 19 cases are Hotline Numbers for COVID-19 males, and 28% are females Please call if you are in: COVID-19 has claimed the lives of 3 persons for every 100 confirmed cases in Somalia Galmudug: 449 Somaliland:988 Puntland: 343 Jubaland: 466 Benadir: 449 Southwest:449 Ministry of Planning, Investment and Economic Development Directorate of National Statistics Number of confirmed cases, FIGURE 1: COVID-19 EVENTS Actives cases, Recoveries, NUMBER OF CONFIR M ED CASES , ACTIVES CASES, and Deaths in Somalia RECOVERIES, AND DEATHS IN SOM ALIA As of 23rd of June 2020, the 2835 number of confirmed cases are 2835 with 829 recoveries and 90 deaths. In addition, 1916 the active cases are 1916 as shown in Figure1 829 90 CONFIRMED ACTIVE CASES RECOVERIES DEATHS CASES Percentage Distribution of COVID 19 Figure 2: Percentage distribution of confirmed cases by State Confirmed Cases by State Hiirshabelle Galmudug Jubaland 1% Approximately 50 percent of the confirmed 4% COVID-19 cases in the country are in 6% Banaadir Region whereas the remaining (24 South West percent) are from Somaliland, Puntland (10 5% percent), Jubbaland (6 percent), South West (5 percent), Galmudug (4 percent) and Hirshabelle State (1 percent) as shown in Benadir (Figure 2). -

Punishment on Stage
Punishment on Stage -Application of Islamic Criminal Law by Harakat al-Shabaab al-Mujahideen- Michael Skjelderup Master’s Degree Thesis in History of Religion (60sp) Department of Culture Studies and Oriental Languages The Faculty of Humanities University of Oslo Autumn 2011 © Michael Skjelderup Autumn 2011 Punishment on Stage: Application of Islamic Criminal Law by Harakat al-Shabaab al- Mujahideen Michael Skjelderup http://www.duo.uio.no/ Trykk: Reprosentralen, Universitetet i Oslo II Executive summary Harakat al-Shabaab al-Mujahideen, usually referred to as al-Shabaab (“the youth”), is mostly known as a Somali terrorist group. But since the end of 2008 it has functioned as a state power in large parts of Southern and Central Somalia. In this study I sketch out the structure and function of the legal system of the group. Over the last three years they have developed an administrative structure and a legal system which is unprecedented in the Somali conflict, which has lasted for more than 20 years. In order to establish law and order in their territories al-Shabaab has applied their own version of sharī’a and issued strict religiously inspired decrees. The present study is based on information acquired through interviews with Somali refugees in Nairobi who have direct experiences with al-Shabaab’s judicial practice. It reveals that al-Shabaab’s application of criminal law follows the inherent logic of classical Islamic legal doctrines on several points. However, the al-Shabaab courts tend to overlook many of the strict requirements regarding evidence and procedure which was outlined by the medieval Muslim scholars in order to humanize Islamic law. -

Exploring the Old Stone Town of Mogadishu
Exploring the Old Stone Town of Mogadishu Exploring the Old Stone Town of Mogadishu By Nuredin Hagi Scikei Exploring the Old Stone Town of Mogadishu By Nuredin Hagi Scikei This book first published 2017 Cambridge Scholars Publishing Lady Stephenson Library, Newcastle upon Tyne, NE6 2PA, UK British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Copyright © 2017 by Nuredin Hagi Scikei All rights for this book reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the copyright owner. ISBN (10): 1-5275-0331-3 ISBN (13): 978-1-5275-0331-1 Dedicated to my father Hagi Scikei Abati, my mother Khadija Ali Omar, my sister Zuhra and my brother Sirajadin. CONTENTS Preface ........................................................................................................ xi Acknowledgements .................................................................................. xiii Chapter One ................................................................................................. 1 Introduction Who are the Banaadiri Maritime Traders and Ancient Banaadiri Settlements Religion and Learning The Growth of Foreign Trade, Urbanisation and the First Industries of Banaadir Chapter Two .............................................................................................. 11 The Campaign of Defamation against the Banaadiri -

Using Satellite Imagery to Track the Developmental Effects of Somali Piracy
Africa Programme Paper: AFP PP 2012/01 Treasure Mapped: Using Satellite Imagery to Track the Developmental Effects of Somali Piracy Dr Anja Shortland Brunel University January 2012 The views expressed in this document are the sole responsibility of the author(s) and do not necessarily reflect the view of Chatham House, its staff, associates or Council. Chatham House is independent and owes no allegiance to any government or to any political body. It does not take institutional positions on policy issues. This document is issued on the understanding that if any extract is used, the author(s)/ speaker(s) and Chatham House should be credited, preferably with the date of the publication or details of the event. Where this document refers to or reports statements made by speakers at an event every effort has been made to provide a fair representation of their views and opinions, but the ultimate responsibility for accuracy lies with this document’s author(s). The published text of speeches and presentations may differ from delivery. Programme Paper: Treasure Mapped SUMMARY POINTS There are increasing pressures to develop land-based approaches to Somali piracy. By making use of non-traditional data sources including local market data and satellite images, this paper is intended to be an objective analysis of who benefits from pirate ransoms. Significant amounts of ransom monies are spent within Somalia, but conspicuous consumption appears to be limited by social norms dictating resource-sharing. Around a third of pirate ransoms are converted into Somali shillings, benefiting casual labour and pastoralists in Puntland. Data analysis is complemented by examination of satellite imagery to establish where the beneficiaries are located. -

Facts & Figures
SOMALIA FACTS AND FIGURES FACTS FACTS & FIGURES JANUARY - JULY 2021 FACILITATING ACCESS TO HEALTH CARE • 282,550 patients benefited from the Primary Health Care program in 29 clinics. • 10,534 patients were treated within the Outpatient Therapeutic program. • 15,529 consultations took place at the four ICRC supported hospitals Emergency rooms. • 2,944 patients received care at the two stabilization centers in Baidoa and Kismayo. • 167 PHC beneficiaries were referred to hospitals for emergency or specialized care and their transportation paid. RESPONDING TO OUTBREAK OF ACUTE WATER DIARRHEA • 21,085 people attended health promotion sessions, while 883 households were visited and provided with AWD prevention information. • 471 people received treatment for AWD at SRCS clinics. PHYSICAL REHABILITATION PROGRAMME • 3,209 people received physical rehabilitation services. • 233 prostheses, 614 orthoses, 484 walking aids and crutches and 105 wheelchairs and postural devices delivered to 3 SRCS centers in Mogadishu, Galkacyo and Hargeisa. • Conducted 7,292 physiotherapy sessions. FIRST AID PROGRAMME • More than 1,240 weapon-wounded, sick and injured have been assisted. • 2,356 families have been undertaken first aid training. • 2,231 volunteer responder teams have been trained on first aid. COVID-19 RESPONSE • Covid-19 prevention messages are broadcasted daily by 12 radio stations across the country from April to June 2020.sss • 224 SRCS volunteers and 154 health staff of PHC clinics trained on Covid-19 prevention messages; 85 health staff working in Medina, Keysaney, Baidoa and Kismayo hospitals trained as well. • 14,576 health promotion sessions reached 103,756 people in Banaadir, Lower Juba, Gedo, Hiiran, Lower Shabelle, Middle Shabelle and Galgadud among other regions; 4,133 sessions held at hospital level, reaching 33,994 people. -
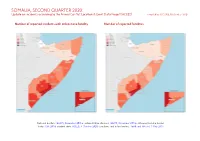
SOMALIA, SECOND QUARTER 2020: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 30 October 2020
SOMALIA, SECOND QUARTER 2020: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 30 October 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; Ethiopia/Somalia border status: CIA, 2014; incident data: ACLED, 3 October 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 SOMALIA, SECOND QUARTER 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 30 OCTOBER 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Battles 327 152 465 Conflict incidents by category 2 Violence against civilians 146 100 144 Development of conflict incidents from June 2018 to June 2020 2 Explosions / Remote 133 59 187 violence Methodology 3 Protests 28 1 1 Conflict incidents per province 4 Strategic developments 18 2 2 Riots 6 0 0 Localization of conflict incidents 4 Total 658 314 799 Disclaimer 6 This table is based on data from ACLED (datasets used: ACLED, 3 October 2020). Development of conflict incidents from June 2018 to June 2020 This graph is based on data from ACLED (datasets used: ACLED, 3 October 2020). 2 SOMALIA, SECOND QUARTER 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 30 OCTOBER 2020 Methodology on what level of detail is reported. Thus, towns may represent the wider region in which an incident occured, or the provincial capital may be used if only the province The data used in this report was collected by the Armed Conflict Location & Event is known. -

Al-Shabaab Is a Movement That Merged Four Somali Groups and Has Been Supported from Its Early Days by Foreign Islamists, Including Those Linked to Al-Qâ’Idah
THE RISE OF A JIHADI MOVEMENT IN A COUNTRY AT WAR HARAKAT AL -SHABAAB AL MUJAHEDDIN IN SOMALIA Roland Marchal Senior Research Fellow at CNRS SciencesPo Paris March 2011 This report is independent and does not represent the views of Her Majesty’s Government CONTENT Content Executive Summary Chapter I: Historical Background to the Development of al-Shabaab 1. A political history 1.1. Learning from failures? The radicalisation of the Somali Islamist movement 1.2. The experiments of the Islamic Courts 1.3. The emergence of al-Shabaab 2. Getting organized 2.1. The Supreme Council 2.2. The ministries or Maktabs 3. Conclusion Chapter II: The confrontation with other Islamic Trends 1. The Salafi divide 2. Al-I’tisaam, Muqawama and the Salafi Trend 3. The merging with Hisbul Islaam 4. The collusion with Takfiir wa Hijra 5. An apolitical Jihad? 6. Conclusion Chapter III: Citizens of Jihad. Al-Shabaab Recruitment 1. Joining al-Shabaab 1.1. Coerced recruitments 1.2. Economic incentives 1.3. Born again Jihadists 2 1.4. Recruitment of diaspora and East African radicalized Muslims 1.5. Challenging generational privileges 2. Short notes on the media policy 3. Recruitment among political “minorities” 4. Conclusion Chapter IV: Al-Shabaab Military Tactics 1. The modernisation of war and the globalisation of suicide bombers 2. Organizing the coexistence of foreign and local fighters 3. Military misadventures 4. Conclusion Chapter V: Funding an apparatus and ruling a population 1. Getting money for al-Shabaab 1.1. Collecting money outside the country 1.2. Getting funding from Somalia: maximisation of the protection economy 2. -

Iom Appeal Somalia Drought January - June 2017 Content
IOM APPEAL SOMALIA DROUGHT JANUARY - JUNE 2017 CONTENT IOM IN SOMALIA ............................................................................................ 3 DROUGHT RESPONSE OVERVIEW ................................................................... 4 SITUATION OVERVIEW ................................................................................... 6 IOM SOMALIA DROUGHT APPEAL .................................................................. 7 IOM SOMALIA PROJECT LOCATIONS ............................................................... 8 IOM SOMALIA DROUGHT RESPONSE LOCATIONS ........................................... 9 FOOD SECURITY .............................................................................................. 11 WATER, SANITATION AND HYGIENE ................................................................ 13 HEALTH ........................................................................................................... 13 SHELTER/NON FOOD ITEMS ........................................................................... 13 PROTECTION-DISPLACEMENT TRACKING MATRIX .......................................... 15 TECHNICAL SUPPORT ..................................................................................... 15 IOM PROJECTS WITHIN THE HUMANITARIAN RESPONS PLAN ......................... 17 COPYRIGHT / PICTURES: COVER: IOM/MARY-SANYU OSIRE PAGE 5: IOM/MARY-SANYU OSIRE PAGE 10: DTM (TOP) & DR. ABDIKADIR OMAR (BOTTOM) PAGE 12: IOM/DR. ABDIKADIR OMAR PAGE 14: IOM/BARRE MUHAMED PAGE 16: IOM/MARY-SANYU OSIRE -

S.No Region Districts 1 Awdal Region Baki
S.No Region Districts 1 Awdal Region Baki District 2 Awdal Region Borama District 3 Awdal Region Lughaya District 4 Awdal Region Zeila District 5 Bakool Region El Barde District 6 Bakool Region Hudur District 7 Bakool Region Rabdhure District 8 Bakool Region Tiyeglow District 9 Bakool Region Wajid District 10 Banaadir Region Abdiaziz District 11 Banaadir Region Bondhere District 12 Banaadir Region Daynile District 13 Banaadir Region Dharkenley District 14 Banaadir Region Hamar Jajab District 15 Banaadir Region Hamar Weyne District 16 Banaadir Region Hodan District 17 Banaadir Region Hawle Wadag District 18 Banaadir Region Huriwa District 19 Banaadir Region Karan District 20 Banaadir Region Shibis District 21 Banaadir Region Shangani District 22 Banaadir Region Waberi District 23 Banaadir Region Wadajir District 24 Banaadir Region Wardhigley District 25 Banaadir Region Yaqshid District 26 Bari Region Bayla District 27 Bari Region Bosaso District 28 Bari Region Alula District 29 Bari Region Iskushuban District 30 Bari Region Qandala District 31 Bari Region Ufayn District 32 Bari Region Qardho District 33 Bay Region Baidoa District 34 Bay Region Burhakaba District 35 Bay Region Dinsoor District 36 Bay Region Qasahdhere District 37 Galguduud Region Abudwaq District 38 Galguduud Region Adado District 39 Galguduud Region Dhusa Mareb District 40 Galguduud Region El Buur District 41 Galguduud Region El Dher District 42 Gedo Region Bardera District 43 Gedo Region Beled Hawo District www.downloadexcelfiles.com 44 Gedo Region El Wak District 45 Gedo -

Epidemiological Week 28 (Week Ending 15Th July, 2018)
Epidemiological Week 28 (Week ending 15th July, 2018) Highlights Cumulative figures as of week 28 • 232 health facilities across Somalia submitted weekly • 1,576,745 consultations from week 1 reports of epidemic-prone diseases in the electronic to week 28. early warning disease surveillance (EWARN) system in • 5,880 cumulative cases of week 28. • Total number of consultations increased from 51,625 AWD/Cholera and 40 deaths since in week 27 to 54,605 in week 28. December 2017. • A total of 307 alerts were received. 35 of these alerts • 8,880 Accumulative alerts were were confirmed as true alerts in week 28. received, 499 of these, were • The highest numbers of diseases reported in week 28 confirmed as true alerts from week 1 were other acute diarrhoeas (2,306 cases), influenza to week 28, 2018. like illness (1,245 cases) and severe acute respiratory illness (1,559 cases). • 6,201 cumulative cases of suspected measles cases since the beginning of • A total of 146 new cases of suspected AWD/cholera with no death were reported in week 28 compared to 2018. Of the 6,201 measles cases, 151 AWD cases with no death in week 27. 4,112 (66%) are under 5 years while • A cumulative total of 5,880 AWD/cholera cases1, 2,089 (34%) are above 5 years. including 40 deaths have been reported since • 7,624 cumulative cases of Malaria December 2017. were reported since the beginning of • The number of reported measles cases decreased 2018, 3,302(43%) are under 5 years, from 61 in week 27 to 52 cases in week 28. -

S 2019 858 E.Pdf
United Nations S/2019/858* Security Council Distr.: General 1 November 2019 Original: English Letter dated 1 November 2019 from the Chair of the Security Council Committee pursuant to resolution 751 (1992) concerning Somalia addressed to the President of the Security Council On behalf of the Security Council Committee pursuant to resolution 751 (1992) concerning Somalia, and in accordance with paragraph 54 of Security Council resolution 2444 (2018), I have the honour to transmit herewith the final report of the Panel of Experts on Somalia. In this connection, the Committee would appreciate it if the present letter and the report were brought to the attention of the members of the Security Council and issued as a document of the Council. (Signed) Marc Pecsteen de Buytswerve Chair Security Council Committee pursuant to resolution 751 (1992) concerning Somalia * Reissued for technical reasons on 14 November 2019. 19-16960* (E) 141119 *1916960* S/2019/858 Letter dated 27 September 2019 from the Panel of Experts on Somalia addressed to the Chair of the Security Council Committee pursuant to resolution 751 (1992) concerning Somalia In accordance with paragraph 54 of Security Council resolution 2444 (2018), we have the honour to transmit herewith the final report of the Panel of Experts on Somalia. (Signed) Jay Bahadur Coordinator Panel of Experts on Somalia (Signed) Mohamed Abdelsalam Babiker Humanitarian expert (Signed) Nazanine Moshiri Armed groups expert (Signed) Brian O’Sullivan Armed groups/natural resources expert (Signed) Matthew Rosbottom Finance expert (Signed) Richard Zabot Arms expert 2/161 19-16960 S/2019/858 Summary During the first reporting period of the Panel of Experts on Somalia, the use by Al-Shabaab of improvised explosive devices reached its greatest extent in Somali history, with a year-on-year increase of approximately one third.