MRI of the Posterolateral Corner of the Knee, Please Have a Look
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Synovial Joints Permit Movements of the Skeleton
8 Joints Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes 8.1 Contrast the major categories of joints, and explain the relationship between structure and function for each category. 8.2 Describe the basic structure of a synovial joint, and describe common accessory structures and their functions. 8.3 Describe how the anatomical and functional properties of synovial joints permit movements of the skeleton. © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes (continued) 8.4 Describe flexion/extension, abduction/ adduction, and circumduction movements of the skeleton. 8.5 Describe rotational and special movements of the skeleton. © 2018 Pearson Education, Inc. Module 8.1: Joints are classified according to structure and movement Joints, or articulations . Locations where two or more bones meet . Only points at which movements of bones can occur • Joints allow mobility while preserving bone strength • Amount of movement allowed is determined by anatomical structure . Categorized • Functionally by amount of motion allowed, or range of motion (ROM) • Structurally by anatomical organization © 2018 Pearson Education, Inc. Module 8.1: Joint classification Functional classification of joints . Synarthrosis (syn-, together + arthrosis, joint) • No movement allowed • Extremely strong . Amphiarthrosis (amphi-, on both sides) • Little movement allowed (more than synarthrosis) • Much stronger than diarthrosis • Articulating bones connected by collagen fibers or cartilage . Diarthrosis (dia-, through) • Freely movable © 2018 Pearson Education, Inc. Module 8.1: Joint classification Structural classification of joints . Fibrous • Suture (sutura, a sewing together) – Synarthrotic joint connected by dense fibrous connective tissue – Located between bones of the skull • Gomphosis (gomphos, bolt) – Synarthrotic joint binding teeth to bony sockets in maxillae and mandible © 2018 Pearson Education, Inc. -

Joints Classification of Joints
Joints Classification of Joints . Functional classification (Focuses on amount of movement) . Synarthroses (immovable joints) . Amphiarthroses (slightly movable joints) . Diarthroses (freely movable joints) . Structural classification (Based on the material binding them and presence or absence of a joint cavity) . Fibrous mostly synarthroses . Cartilagenous mostly amphiarthroses . Synovial diarthroses Table of Joint Types Functional across Synarthroses Amphiarthroses Diarthroses (immovable joints) (some movement) (freely movable) Structural down Bony Fusion Synostosis (frontal=metopic suture; epiphyseal lines) Fibrous Suture (skull only) Syndesmoses Syndesmoses -fibrous tissue is -ligaments only -ligament longer continuous with between bones; here, (example: radioulnar periosteum short so some but not interosseous a lot of movement membrane) (example: tib-fib Gomphoses (teeth) ligament) -ligament is periodontal ligament Cartilagenous Synchondroses Sympheses (bone united by -hyaline cartilage -fibrocartilage cartilage only) (examples: (examples: between manubrium-C1, discs, pubic epiphyseal plates) symphesis Synovial Are all diarthrotic Fibrous joints . Bones connected by fibrous tissue: dense regular connective tissue . No joint cavity . Slightly immovable or not at all . Types . Sutures . Syndesmoses . Gomphoses Sutures . Only between bones of skull . Fibrous tissue continuous with periosteum . Ossify and fuse in middle age: now technically called “synostoses”= bony junctions Syndesmoses . In Greek: “ligament” . Bones connected by ligaments only . Amount of movement depends on length of the fibers: longer than in sutures Gomphoses . Is a “peg-in-socket” . Only example is tooth with its socket . Ligament is a short periodontal ligament Cartilagenous joints . Articulating bones united by cartilage . Lack a joint cavity . Not highly movable . Two types . Synchondroses (singular: synchondrosis) . Sympheses (singular: symphesis) Synchondroses . Literally: “junction of cartilage” . Hyaline cartilage unites the bones . Immovable (synarthroses) . -
NOTES: Joints and Types of Movements, Continued (Ch 7, Part 4)
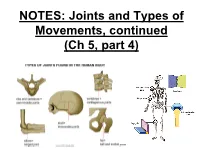
NOTES: Joints and Types of Movements, continued (Ch 5, part 4) *Joints are functional junctions between bones. TYPES OF JOINTS **Joints can be classified according to the type of tissue that binds the bones together.** FIBROUS JOINTS: • bones at fibrous joints are tightly joined by a layer of dense connective tissue. • little or no movement occurs at a fibrous joint • Example: the sutures between the flat bones of the skull CARTILAGINOUS JOINTS: • a layer of hyaline cartilage, or fibrocartilage, joins bones of cartilaginous joints • allow limited movement • Example: the joints that separate the vertebrae SYNOVIAL JOINTS: • most joints in the body are synovial joints • allow free movement • bones at synovial joints are covered with hyaline cartilage (“articular cartilage”) and held together by a fibrous JOINT CAPSULE. SYNOVIAL JOINTS: • the joint capsule consists of an outer layer of ligaments and an inner lining of synovial membrane (which secretes synovial fluid to lubricate the joint). • some synovial joints have flattened, shock- absorbing pads of fibrocartilage called MENISCI between the articulating surfaces of the bones SYNOVIAL JOINTS: • some synovial joints may also have BURSAE, which are fluid-filled sacs located between the skin and the underlying bony prominences. • Example: at the knee joint, the patella is sandwiched between 2 bursae. TYPES OF SYNOVIAL JOINTS: • Ball-and-socket - round head of one bone rests within a cup-shaped depression of another - all angular and rotational movements, including circumduction can be performed by this joint TYPES OF SYNOVIAL JOINTS: • Gliding (planar) – Have flattened or slightly curved faces – Flat articular surfaces slide across one another – Amount of movements is slightly TYPES OF SYNOVIAL JOINTS: • Condylar (ellipsoid) – Oval articular face nests within a depression in opposing surface – Angular movements occur in 2 planes: along or across length of oval TYPES OF SYNOVIAL JOINTS: • Hinge – Permits angular motion in single plane (e.g. -

1. Synarthrosis - Immovable
jAnatomy Lecture Notes Chapter 9 I. classification A. by function - 1. synarthrosis - immovable 2. amphiarthrosis - slightly movable 3. diarthrosis - freely movable B. by structure - material attaching bones together 1. fibrous -.dense c.t., no joint cavity a. suture - very thin, short fibers synostosis - ossification of fibrous c.t. in a suture joint b. syndesmosis - ligament (the longer the fibers the more movement is possible) c. gomphosis - periodontal ligament holds teeth in alveoli 2. cartilaginous - cartilage, no joint cavity a. synchondrosis - hyaline cartilage b. symphysis - fibrocartilage 3. synovial - joint capsule and ligaments II. structure of a synovial joint A. bone and articular cartilage (hyaline) • articular cartilage cushions bone ends by absorbing compression stress Strong/Fall 2008 page 1 jAnatomy Lecture Notes Chapter 9 B. articular capsule 1. fibrous capsule - dense irregular c.t.; holds bones together 2. synovial membrane - areolar c.t. with some simple squamous e.; makes synovial fluid C. joint cavity and synovial fluid 1. synovial fluid consists of: • fluid that is filtered from capillaries in the synovial membrane • glycoprotein molecules that are made by fibroblasts in the synovial membrane 2. fluid lubricates surface of bones inside joint capsule D. ligaments - made of dense fibrous c.t.; strengthen joint • capsular • extracapsular • intracapsular E. articular disc / meniscus - made of fibrocartilage; improves fit between articulating bones F. bursae - membrane sac enclosing synovial fluid found around some joints; cushion ligaments, muscles, tendons, skin, bones G. tendon sheath - elongated bursa that wraps around a tendon Strong/Fall 2008 page 2 jAnatomy Lecture Notes Chapter 9 III. movements at joints flexion extension abduction adduction circumduction rotation inversion eversion protraction retraction supination pronation elevation depression opposition dorsiflexion plantar flexion gliding Strong/Fall 2008 page 3 jAnatomy Lecture Notes Chapter 9 IV. -

Medial Meniscus Anatomy
Quantitative and Qualitative Assessment of the Posterior Medial Meniscus Anatomy Defining Meniscal Ramp Lesions Nicholas N. DePhillipo,*y MS, ATC, OTC, Gilbert Moatshe,yz§ MD, PhD, Jorge Chahla,z MD, PhD, Zach S. Aman,z BA, Hunter W. Storaci,z MSc, Elizabeth R. Morris,z BA, Colin M. Robbins,z BA, Lars Engebretsen,§ MD, PhD, and Robert F. LaPrade,*k MD, PhD Investigation performed at Steadman Philippon Research Institute, Vail, Colorado, USA Background: Meniscal ramp lesions have been defined as a tear of the peripheral attachment of the posterior horn of the medial meniscus (PHMM) at the meniscocapsular junction or an injury to the meniscotibial attachment. Precise anatomic descriptions of these structures are limited in the current literature. Purpose: To quantitatively and qualitatively describe the PHMM and posteromedial capsule anatomy pertaining to the location of a meniscal ramp lesion with reference to surgically relevant landmarks. Study Design: Descriptive laboratory study. Methods: Fourteen male nonpaired fresh-frozen cadavers were used. The locations of the posteromedial meniscocapsular and meniscotibial attachments were identified. Measurements to surgically relevant landmarks were performed with a coordinate measuring system. To further analyze the posteromedial meniscocapsular and meniscotibial attachments, hematoxylin and eosin and alcian blue staining were conducted on a separate sample of 10 nonpaired specimens. Results: The posterior meniscocapsular attachment had a mean 6 SD length of 20.2 6 6.0 mm and attached posteroinferiorly to the PHMM at a mean depth of 36.4% of the total posterior meniscal height. The posterior meniscotibial ligament attached on the PHMM 16.5 mm posterior and 7.7 mm medial to the center of the posterior medial meniscal root attachment. -

Gen Anat-Joints
JOINTS Joint is a junction between two or more bones Classification •Functional Based on the range and type of movement they permit •Structural On the basis of their anatomic structure Functional Classification • Synarthrosis No movement e.g. Fibrous joint • Amphiarthrosis Slight movement e.g. Cartilagenous joint • Diarthrosis Movement present Cavity present Also called as Synovial joint eg.shoulder joint Structural Classification Based on type of connective tissue binding the two adjacent articulating bones Presence or absence of synovial cavity in between the articulating bone • Fibrous • Cartilagenous • Synovial Fibrous Joint Bones are connected to each other by fibrous (connective ) tissue No movement No synovial cavity • Suture • Syndesmosis • Gomphosis Sutural Joints • A thin layer of dens fibrous tissue binds the adjacent bones • These appear between the bones which ossify in membrane • Present between the bones of skull e.g . coronal suture, sagittal suture • Schindylesis: – rigid bone fits in to a groove on a neighbouring bone e.g. Vomer and sphenoid Gomphosis • Peg and socket variety • Cone shaped root of tooth fits in to a socket of jaw • Immovable • Root is attached to the socket by fibrous tissue (periodontal ligament). Syndesmosis • Bony surfaces are bound together by interosseous ligament or membrane • Membrane permits slight movement • Functionally classified as amphiarthrosis e.g. inferior tibiofibular joint Cartilaginous joint • Bones are held together by cartilage • Absence of synovial cavity . Synchondrosis . Symphysis Synchondrosis • Primary cartilaginous joint • Connecting material between two bones is hyaline cartilage • Temporary joint • Immovable joint • After a certain age cartilage is replaced by bone (synostosis) • e.g. Epiphyseal plate connecting epiphysis and diphysis of a long bone, joint between basi-occiput and basi-sphenoid Symphysis • Secondary cartilaginous joint (fibrocartilaginous joint) • Permanent joint • Occur in median plane of the body • Slightly movable • e.g. -

Connections of Bones
Connections of bones Reinitz László Z. Arthrologia generales- general arthrology Classification based on the freedom of movement • Synarthrosis [Articulationes fibrosae] • limited movement, connection through connective tissue • Amphiarthrosis • limited movement • narrow articular gap • may be through cartilage or ligaments • art. carpometacarpea • Diarthrosis – [Articulationes synoviales] • unlimited movement • (Synsarcosis) • connection via muscles Synarthrosis [Articulationes fibrosae] • No joint gap • Synostosis - ossification • Ru McIII-IV. • Gomphosis – penetration • alveolus-tooth • Suturae - suture • Sutura serrata – saw suture • Ossa parietalia • Sutura foliata – leaf suture • Sutura frontonasalis • Sutura squamosa –squamosal suture • Sutura squamosofrontalis • Sutura plana – flat suture • Sutura internasalis • Syndesmosis – through connective tissue, ligament • Car: radius-ulna Amphiarthrosis [Articulationes cartilagineae] • minimal joint gap • able to move in every directions • but those are very limited • Art. carpometacarpea • Synchondrosis • hyalin cartilage • Art. sternocostalis • Symphysis • fibrous cartilage • Symphysis pelvis Diarthrosis [Articulationes synovialis] • Joint gap • Free movement • General description of joints [drawing] • [video] • Ligaments of joints • Ligg. Intracapsularia – part of the joint capsule • Ligg. Extracapsularia – outside the joint capsule • Ligg. Intercapsularia - within the joint cavity • If the surfaces do not match (incongruent surfaces) • Cartilage supplement • discus – separates the joint -

Joint Capsule Collagen in Osteoarthrosis
Ann Rheum Dis: first published as 10.1136/ard.32.6.510 on 1 November 1973. Downloaded from Ann. rheum. Dis. (1973), 32, 510 Joint capsule collagen in osteoarthrosis C. HERBERT, M. I. V. JAYSON, AND A. J. BAILEY From the Department ofMedicine, University ofBristol, the Royal National Hospitalfor Rheumatic Diseases, Bath, and the Agricultural Research Council, Meat Research Institute, Langford, Bristol It has long been recognized that although osteoarth- and stability of the capsular collagen could lead to rosis is characterized by degenerative changes in the the observed symptoms. articular cartilage and bones, changes in the capsule Recent studies have established that the stability play an important part in the symptoms. The capsule of the collagen fibre depends upon the formation of becomes thickened and lacks its normal pliability, inter-molecular cross-links between the tropocollagen thus restricting normal movement (Gade, 1947; molecules making up the fibre (Bailey, 1968; Traub Apley, 1969) and resulting in pain in the joint. and Piez, 1971). These cross-links are formed Similarly, Jayson (1969) described a series of patients extracellularly through reaction of aldehydes derived with arthralgia and increased joint capsule stiffness. from specific lysine and hydroxylysine on the collagen Incision, or partial removal of the osteoarthritic molecule (see Scheme). capsule, relieves the pain and improves the range of There is now a well-documented pattern of evolu- movement and degree of deformity (Lloyd-Roberts, tion of these inter-molecular cross-links. The links 1953; Gade, 1947). The joint cavity and articular initially formed are labile Schiff-bases and may be by copyright. -

Medial Meniscus Anatomy—From Basic Science to Treatment
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/270004929 Medial meniscus anatomy—from basic science to treatment Article in Knee Surgery Sports Traumatology Arthroscopy · December 2014 DOI: 10.1007/s00167-014-3476-5 · Source: PubMed CITATIONS READS 40 1,012 4 authors, including: Robert Smigielski Roland Becker Medical University of Warsaw Hospital Brandenburg, Teaching Hospital of the Charite University of Berlin 55 PUBLICATIONS 408 CITATIONS 206 PUBLICATIONS 2,659 CITATIONS SEE PROFILE SEE PROFILE Urszula Zdanowicz Carolina Medical Center 31 PUBLICATIONS 196 CITATIONS SEE PROFILE Some of the authors of this publication are also working on these related projects: Surgical Anatomy of the Knee Joint View project vitamys VEPE View project All content following this page was uploaded by Urszula Zdanowicz on 28 August 2016. The user has requested enhancement of the downloaded file. Medial meniscus anatomy—from basic science to treatment Robert Śmigielski, Roland Becker, Urszula Zdanowicz & Bogdan Ciszek Knee Surgery, Sports Traumatology, Arthroscopy ISSN 0942-2056 Knee Surg Sports Traumatol Arthrosc DOI 10.1007/s00167-014-3476-5 1 23 Your article is protected by copyright and all rights are held exclusively by European Society of Sports Traumatology, Knee Surgery, Arthroscopy (ESSKA). This e-offprint is for personal use only and shall not be self- archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. -

4 Anat 35 Articulations
Human Anatomy Unit 1 ARTICULATIONS In Anatomy Today Classification of Joints • Criteria – How bones are joined together – Degree of mobility • Minimum components – 2 articulating bones – Intervening tissue • Fibrous CT or cartilage • Categories – Synarthroses – no movement – Amphiarthrosis – slight movement – Diarthrosis – freely movable Synarthrosis • Immovable articulation • Types – Sutures – Schindylesis – Gomphosis – Synchondrosis Synarthrosis Sutures • Found only in skull • Immovable articulation • Flat bones joined by thin layer of fibrous CT • Types – Serrate – Squamous (lap) – Plane Synarthrosis Sutures • Serrate • Serrated edges of bone interlock • Two portions of frontal bones • Squamous (lap) • Overlapping beveled margins forms smooth line • Temporal and parietal bones • Plane • Joint formed by straight, nonoverlapping edges • Palatine process of maxillae Synarthrosis Schindylesis • Immovable articulation • Thin plate of bone into cleft or fissure in a separation of the laminae in another bone • Articulation of sphenoid bone and perpendicular plate of ethmoid bone with vomer Synarthrosis Gomphosis • Immovable articulation • Conical process into a socket • Articulation of teeth with alveoli of maxillary bone • Periodontal ligament = fibrous CT Synarthrosis Synchondrosis • Cartilagenous joints – Ribs joined to sternum by hyaline cartilage • Synostoses – When joint ossifies – Epiphyseal plate becomes epiphyseal line Amphiarthrosis • Slightly moveable articulation • Articulating bones connected in one of two ways: – By broad flattened -

Musculoskeletal System
4 Musculoskeletal System Learning Objectives Upon completion of this chapter, you will be able to • Identify and define the combining forms, prefixes, and suffixes introduced in this chapter. • Correctly spell and pronounce medical terms and major anatomical structures relating to the musculoskeletal system. • Locate and describe the major organs of the musculoskeletal system and their functions. • Correctly place bones in either the axial or the appendicular skeleton. • List and describe the components of a long bone. • Identify bony projections and depressions. • Identify the parts of a synovial joint. • Describe the characteristics of the three types of muscle tissue. • Use movement terminology correctly. • Identify and define musculoskeletal system anatomical terms. • Identify and define selected musculoskeletal system pathology terms. • Identify and define selected musculoskeletal system diagnostic procedures. • Identify and define selected musculoskeletal system therapeutic procedures. • Identify and define selected medications relating to the musculoskeletal system. • Define selected abbreviations associated with the musculoskeletal system. 83 M04_FREM0254_06_SE_C04.indd 83 18/12/14 10:12 pm Section I: Skeletal System at a Glance Function The skeletal system consists of 206 bones that make up the internal framework of the body, called the skeleton. The skeleton supports the body, protects internal organs, serves as a point of attachment for skeletal muscles for body movement, produces blood cells, and stores minerals. Organs Here -
A Proposal for a New Morphological Classification of the Popliteus
www.nature.com/scientificreports OPEN A proposal for a new morphological classifcation of the popliteus muscle tendon with potential clinical and biomechanical signifcance Łukasz Olewnik1*, Robert F. LaPrade2, Friedrich Paulsen3,4, Bartosz Gonera1, Konrad Kurtys1, Michał Podgórski5, Paloma Aragonés6, J. Ramón Sanudo7 & Michał Polguj8 The purpose of this study was to characterize the morphological variations in the proximal attachments and create an accurate classifcation of the PPM for use in planning surgical procedures in this area, for evaluating radiological imaging and rehabilitation. One hundred and thirty-four lower limbs of body donors (52 woman and 82 man) fxed in 10% formalin solution were examined. The popliteus muscle was present in all 134 limbs. Four main types were identifed with subtypes. The most common type was Type I (34.3%), characterized by a single tendon in the popliteus sulcus. Type II (30.6%) characterized by a main tendon in the popliteus sulcus and accessory bands. This type was divided into fve subtypes (A–E) based on presence of specifc accessory bands. Type III (15.3%) was characterized by two tendons in the popliteal sulcus. Type IV (19.4%) was characterized by two tendons in the popliteus sulcus and additional bands. This type was also divided into fve subtypes (A–E) based on presence of specifc accessory bands. The popliteofbular ligament was present in 90.3% of cases. A new classifcation based on a proximal attachment is proposed. The popliteus tendon is characterized by a very high morphological variability, which can afect posterolateral knee stability and the natural rotation of the tibia.