A Proposal for a New Morphological Classification of the Popliteus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Synovial Joints Permit Movements of the Skeleton
8 Joints Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes 8.1 Contrast the major categories of joints, and explain the relationship between structure and function for each category. 8.2 Describe the basic structure of a synovial joint, and describe common accessory structures and their functions. 8.3 Describe how the anatomical and functional properties of synovial joints permit movements of the skeleton. © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes (continued) 8.4 Describe flexion/extension, abduction/ adduction, and circumduction movements of the skeleton. 8.5 Describe rotational and special movements of the skeleton. © 2018 Pearson Education, Inc. Module 8.1: Joints are classified according to structure and movement Joints, or articulations . Locations where two or more bones meet . Only points at which movements of bones can occur • Joints allow mobility while preserving bone strength • Amount of movement allowed is determined by anatomical structure . Categorized • Functionally by amount of motion allowed, or range of motion (ROM) • Structurally by anatomical organization © 2018 Pearson Education, Inc. Module 8.1: Joint classification Functional classification of joints . Synarthrosis (syn-, together + arthrosis, joint) • No movement allowed • Extremely strong . Amphiarthrosis (amphi-, on both sides) • Little movement allowed (more than synarthrosis) • Much stronger than diarthrosis • Articulating bones connected by collagen fibers or cartilage . Diarthrosis (dia-, through) • Freely movable © 2018 Pearson Education, Inc. Module 8.1: Joint classification Structural classification of joints . Fibrous • Suture (sutura, a sewing together) – Synarthrotic joint connected by dense fibrous connective tissue – Located between bones of the skull • Gomphosis (gomphos, bolt) – Synarthrotic joint binding teeth to bony sockets in maxillae and mandible © 2018 Pearson Education, Inc. -

An Evidence Based Medicine Understanding of Meniscus Injuries and How to Treat Them
An Evidence Based Medicine Understanding of Meniscus Injuries and How to Treat Them Patrick S. Buckley, MD University Orthopaedic Associates June 1, 2019 Disclosures • None www.UOANJ.com Anatomy of the Meniscus • Act as functional extensions of the tibial plateaus to increase depth of tibial articular surface • The meniscotibial attachment contributes to knee stability • Triangular in cross-section Gross Anatomy of the Meniscus • Ultrastructural Anatomy – Primarily Type I collagen (90%) – 70% water – Fiber orientation is circumferential (hoop stressing) Meniscal Vascularity • Relatively avascular • Vascular penetration – 10 - 30% medial – 10 - 25% lateral • Non-vascularized portions gain nutrients from mechanical loading and joint motion Medial Meniscus • Semilunar shape • Thin anterior horn • Broader posterior horn • More stable & less motion than the lateral = tears more often Lateral Meniscus • Almost circular in shape • Intimately associated with the ACL tibial insertion • Posterior horn attachments – Ligament of Humphrey – Ligament of Wrisberg • Lateral meniscus is a more dynamic structure with more motion Main Importance of Menisci • Load transmission • Joint stability Load Bearing / Shock Absorption • MM 50% and 70% LM of load transmitted through mensicus in extension • 85 % at 90° of flexion • Meniscectomy – 50 % decrease in contact area – 20 % less shock absorption www.UOANJ.com Meniscal effect on joint stability • Secondary restraints to anterior tibial translation in normal knees • In an ACL-deficient knee: the posterior horn of the medial meniscus is more important than the lateral meniscus Interaction of ACL and PHMM • Lack of MM in ACLD knees significantly ↑ anterior tibial translation at all knee flexion angles • Think about with high grade pivot! (Levy, JBJS,1982) (Allen, JOR,2000) C9ristiani, AJSM, 2017) Meniscus Function -Now known to be important structure for load distribution and secondary stabilizer to the knee. -

Meniscus Tear
291 North Fireweed Soldotna, AK 99669 907-262-6454 www.kenaipeninsulaortho.com ______________________________________________________________________________________ Orthopaedic Surgeon: Hand and Wrist Specialist: Henry G. Krull, M.D. Edwin D. Vyhmeister, M.D. Meniscus Tear The meniscus is the rubbery, soft cartilage cushion in the knee. There are two of the C-shaped cushions in each knee, a medial (inner) and lateral (outer) meniscus. They sit between the two bones that form the knee joint, and function to cushion and support the knee. The meniscus can tear with injury or degeneration, or a combination of both. The medial meniscus is torn about 10X more frequently than the lateral meniscus. In young people, the meniscus usually tears with an injury. In older people, the cartilage can degenerate (weaken) with age, and can tear with or without an injury; spontaneous tears can occur. Meniscal tears can occur in association with other injuries to the knee. Symptoms: Pain is the usual symptom of complaint with a meniscus tear. There is often a noticeable “pop.” Swelling and stiffness can also occur. Mechanical symptoms are common—clicking, popping, and locking. Sometimes there is just a feeling that something is wrong inside the knee. Pain can be sharp, or can be dull and aching. Meniscus tears do not heal, but sometimes the symptoms dissipate. Chronic, intermittent symptoms is very common. Meniscal tears can cause a feeling of instability, or can cause the knee to buckle or give way. Cause: Injuries, particularly with sports, are a common cause of meniscal tears in young people. As people age, the meniscus tissue weakens through the normal degenerative process, and tears can occur spontaneously, or with simple activities, such as getting up from a chair, and changing direction while walking. -

About Your Knee
OrthoInfo Basics About Your Knee What are the parts of the knee? Your knee is Your knee is made up of four main things: bones, cartilage, ligaments, the largest joint and tendons. in your body Bones. Three bones meet to form your knee joint: your thighbone and one of the (femur), shinbone (tibia), and kneecap (patella). Your patella sits in most complex. front of the joint and provides some protection. It is also vital Articular cartilage. The ends of your thighbone and shinbone are covered with articular cartilage. This slippery substance to movement. helps your knee bones glide smoothly across each other as you bend or straighten your leg. Because you use it so Two wedge-shaped pieces of meniscal cartilage act as much, it is vulnerable to Meniscus. “shock absorbers” between your thighbone and shinbone. Different injury. Because it is made from articular cartilage, the meniscus is tough and rubbery to help up of so many parts, cushion and stabilize the joint. When people talk about torn cartilage many different things in the knee, they are usually referring to torn meniscus. can go wrong. Knee pain or injury Femur is one of the most (thighbone) common reasons people Patella (kneecap) see their doctors. Most knee problems can be prevented or treated with simple measures, such as exercise or Articular cartilage training programs. Other problems require surgery Meniscus to correct. Tibia (shinbone) 1 OrthoInfo Basics — About Your Knee What are ligaments and tendons? Ligaments and tendons connect your thighbone Collateral ligaments. These are found on to the bones in your lower leg. -

Arthroscopic Partial Meniscectomy 1
Chris Lena MD, James Alvarez PAC Arthroscopic and Reconstructive Surgery of the Shoulder and Knee Sports Medicine MEA’s Karen Smith, Jackie Zuidema, Annmarie Fiore Tel: (860) 549-8249 - FAX: (860) 244-8813 www.oahct.com Arthroscopic Partial Meniscectomy 1. ACTIVITIES: No harm is done in putting full weight on your knee immediately. You are encouraged to try to walk as smoothly as possible. Do not do any strenuous activity such as running and jumping until I clear you for this. You may experience some mild discomfort as you walk. You may use crutches, but generally they are not necessary. You may start bending your knee as tolerated, the sooner the better. 2. BANDAGES: Your bandage may be removed 2 days following surgery. The knee should then be re-wrapped with only the elastic bandage for about 3-4 days or until swelling is gone. DO NOT wrap the elastic bandage too tightly, or it will act like a tourniquet and cause ankle swelling. 3. MEDICATIONS: : A prescription will be provided to help relieve pain. Please use this medication as directed. This medication is strong, and should not be taken with alcohol or other pain medications, and may cause drowsiness. Exercise good judgment in its use. You may also try over the counter pain medications such as Aleve (naprosyn) or Advil (Ibuprofen). Take as directed unless there are contraindications. Take 1 Aspirin (325 mg) daily in addition to the pain medication. 4. SHOWER: You may shower after 48 hours. Do not take a bath or submerge the knee under water for 7 days. -

Joints Classification of Joints
Joints Classification of Joints . Functional classification (Focuses on amount of movement) . Synarthroses (immovable joints) . Amphiarthroses (slightly movable joints) . Diarthroses (freely movable joints) . Structural classification (Based on the material binding them and presence or absence of a joint cavity) . Fibrous mostly synarthroses . Cartilagenous mostly amphiarthroses . Synovial diarthroses Table of Joint Types Functional across Synarthroses Amphiarthroses Diarthroses (immovable joints) (some movement) (freely movable) Structural down Bony Fusion Synostosis (frontal=metopic suture; epiphyseal lines) Fibrous Suture (skull only) Syndesmoses Syndesmoses -fibrous tissue is -ligaments only -ligament longer continuous with between bones; here, (example: radioulnar periosteum short so some but not interosseous a lot of movement membrane) (example: tib-fib Gomphoses (teeth) ligament) -ligament is periodontal ligament Cartilagenous Synchondroses Sympheses (bone united by -hyaline cartilage -fibrocartilage cartilage only) (examples: (examples: between manubrium-C1, discs, pubic epiphyseal plates) symphesis Synovial Are all diarthrotic Fibrous joints . Bones connected by fibrous tissue: dense regular connective tissue . No joint cavity . Slightly immovable or not at all . Types . Sutures . Syndesmoses . Gomphoses Sutures . Only between bones of skull . Fibrous tissue continuous with periosteum . Ossify and fuse in middle age: now technically called “synostoses”= bony junctions Syndesmoses . In Greek: “ligament” . Bones connected by ligaments only . Amount of movement depends on length of the fibers: longer than in sutures Gomphoses . Is a “peg-in-socket” . Only example is tooth with its socket . Ligament is a short periodontal ligament Cartilagenous joints . Articulating bones united by cartilage . Lack a joint cavity . Not highly movable . Two types . Synchondroses (singular: synchondrosis) . Sympheses (singular: symphesis) Synchondroses . Literally: “junction of cartilage” . Hyaline cartilage unites the bones . Immovable (synarthroses) . -

Meniscus FAQ Robert T. Bents, MD
Meniscus FAQ Robert T. Bents, MD Q. What is a “meniscus”? A. The meniscus is a “C” shaped shock absorber in your knee joint. The meniscus is made of cartilage similar to your earlobe. The meniscus has several different functions‐shock absorption, joint stabilization, and joint instability. A healthy meniscus is important to protect against arthritis. Q. What does it mean to “tear” a meniscus? A. You can tear a meniscus in many different ways. As we get older the water content of the meniscus decreases and becomes more brittle. With twisting, squatting, or sporting activities the meniscus can be pinched between the femur and tibia causing it to fray, tear, or split. The tear may occur with injury or simply fray with aging. The most severe tears involve the attachment to the bone called the root. Q. What are some of the symptoms of a torn meniscus? A. Patients may have pain associated with twisting activities. The pain is usually localized along the inside (medial) or outside (lateral) part of the knee. Swelling of the joint is another common complaint. Sometimes patients will feel like something is catching or pinching in the joint. Occasionally the knee will “lock” in a certain position. Most of these symptoms are reproducible by the doctor’s examination. Q. Will an X‐ray detect a meniscal tear? A. No. The purpose of the X‐ray is to make certain that you do not have any underlying arthritis in your knee. Also a loose bone chips or “loose body” may mimic a meniscal tear. The X‐ray gives your doctor information about the “bony” anatomy of a joint. -
NOTES: Joints and Types of Movements, Continued (Ch 7, Part 4)
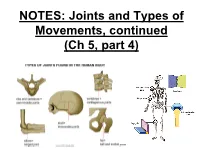
NOTES: Joints and Types of Movements, continued (Ch 5, part 4) *Joints are functional junctions between bones. TYPES OF JOINTS **Joints can be classified according to the type of tissue that binds the bones together.** FIBROUS JOINTS: • bones at fibrous joints are tightly joined by a layer of dense connective tissue. • little or no movement occurs at a fibrous joint • Example: the sutures between the flat bones of the skull CARTILAGINOUS JOINTS: • a layer of hyaline cartilage, or fibrocartilage, joins bones of cartilaginous joints • allow limited movement • Example: the joints that separate the vertebrae SYNOVIAL JOINTS: • most joints in the body are synovial joints • allow free movement • bones at synovial joints are covered with hyaline cartilage (“articular cartilage”) and held together by a fibrous JOINT CAPSULE. SYNOVIAL JOINTS: • the joint capsule consists of an outer layer of ligaments and an inner lining of synovial membrane (which secretes synovial fluid to lubricate the joint). • some synovial joints have flattened, shock- absorbing pads of fibrocartilage called MENISCI between the articulating surfaces of the bones SYNOVIAL JOINTS: • some synovial joints may also have BURSAE, which are fluid-filled sacs located between the skin and the underlying bony prominences. • Example: at the knee joint, the patella is sandwiched between 2 bursae. TYPES OF SYNOVIAL JOINTS: • Ball-and-socket - round head of one bone rests within a cup-shaped depression of another - all angular and rotational movements, including circumduction can be performed by this joint TYPES OF SYNOVIAL JOINTS: • Gliding (planar) – Have flattened or slightly curved faces – Flat articular surfaces slide across one another – Amount of movements is slightly TYPES OF SYNOVIAL JOINTS: • Condylar (ellipsoid) – Oval articular face nests within a depression in opposing surface – Angular movements occur in 2 planes: along or across length of oval TYPES OF SYNOVIAL JOINTS: • Hinge – Permits angular motion in single plane (e.g. -

Understanding the Stiff-To-Compliant Transition of the Meniscal
Research Article Cite This: ACS Appl. Mater. Interfaces 2019, 11, 26559−26570 www.acsami.org Understanding the Stiff-to-Compliant Transition of the Meniscal Attachments by Spatial Correlation of Composition, Structure, and Mechanics Alexander J. Boys,† Jennie A. M. R. Kunitake,† Corinne R. Henak,‡ Itai Cohen,§ Lara A. Estroff,†,∥ and Lawrence J. Bonassar*,‡,⊥ † ‡ § ∥ Department of Materials Science & Engineering, Meinig School of Biomedical Engineering, Department of Physics, Kavli ⊥ Institute at Cornell for Nanoscale Science, and Sibley School of Mechanical Engineering, Cornell University, Ithaca, New York 14853, United States *S Supporting Information ABSTRACT: Recently, the scientific community has shown considerable interest in engineering tissues with organized compositional and structural gradients to mimic hard-to-soft tissue interfaces. This effort is hindered by an incomplete understanding of the construction of native tissue interfaces. In this work, we combined Raman microscopy and confocal elastography to map compositional, structural, and mechanical features across the stiff-to-compliant interface of the attach- ments of the meniscus in the knee. This study provides new insight into the methods by which biology mediates multiple orders of magnitude changes in stiffness over tens of microns. We identified how the nano- to mesoscale architecture mediates complex microscale transitional regions across the interface: two regions defined by chemical composition, five distinguished by structural features, and three mechanically distinct regions. We identified three major components that lead to a robust interface between a soft tissue and bone: mobile collagen fiber units, a continuous interfacial region, and a local stiffness gradient. This tissue architecture allows for large displacements of collagen fibers in the attachments, enabling meniscal movement without localizing strains to the soft tissue-to-bone interface. -

Postoperative Instructions for Knee Arthroscopy, Torn Meniscus Dr
Postoperative Instructions For Knee Arthroscopy, Torn Meniscus Dr. Jeffrey J. Mair, DO PAIN: You will be sent home from the surgery center with prescriptions for pain medication. Take the pain medication as prescribed. After the first few days, as the pain lessens, you may decrease the frequency with which you take the medication and taper off as you feel comfortable, but keep in mind that many people have an increase in pain around day 3 or 4 after surgery. Remember, the medications are not necessarily meant to completely eliminate your pain, only to make it more bearable. It is also helpful to use ice, as well as to elevate your leg to decrease pain and swelling. Elevation should be achieved by placing pillows under the heel or calf—not under the knee—in order to keep your leg straight. If these measures are not adequately controlling your pain, please call our office. MEDICATIONS: Most pain medications need a handwritten prescription for refills and cannot be obtained after hours or on the weekends. Please plan accordingly. Narcotic pain medications can cause constipation; you may wish to use an over-the- counter stool softener to help prevent this. DRESSINGS: You will have a soft dressing applied over your incisions. It is meant to absorb any leaking blood or fluid from the joint, and to protect from infection. Leakage immediately after surgery is normal and actually helps to drain some of the fluid that accumulates in the joint during surgery. The dressings may become moist or blood-stained; this is normal and usually not a cause for alarm. -

1. Synarthrosis - Immovable
jAnatomy Lecture Notes Chapter 9 I. classification A. by function - 1. synarthrosis - immovable 2. amphiarthrosis - slightly movable 3. diarthrosis - freely movable B. by structure - material attaching bones together 1. fibrous -.dense c.t., no joint cavity a. suture - very thin, short fibers synostosis - ossification of fibrous c.t. in a suture joint b. syndesmosis - ligament (the longer the fibers the more movement is possible) c. gomphosis - periodontal ligament holds teeth in alveoli 2. cartilaginous - cartilage, no joint cavity a. synchondrosis - hyaline cartilage b. symphysis - fibrocartilage 3. synovial - joint capsule and ligaments II. structure of a synovial joint A. bone and articular cartilage (hyaline) • articular cartilage cushions bone ends by absorbing compression stress Strong/Fall 2008 page 1 jAnatomy Lecture Notes Chapter 9 B. articular capsule 1. fibrous capsule - dense irregular c.t.; holds bones together 2. synovial membrane - areolar c.t. with some simple squamous e.; makes synovial fluid C. joint cavity and synovial fluid 1. synovial fluid consists of: • fluid that is filtered from capillaries in the synovial membrane • glycoprotein molecules that are made by fibroblasts in the synovial membrane 2. fluid lubricates surface of bones inside joint capsule D. ligaments - made of dense fibrous c.t.; strengthen joint • capsular • extracapsular • intracapsular E. articular disc / meniscus - made of fibrocartilage; improves fit between articulating bones F. bursae - membrane sac enclosing synovial fluid found around some joints; cushion ligaments, muscles, tendons, skin, bones G. tendon sheath - elongated bursa that wraps around a tendon Strong/Fall 2008 page 2 jAnatomy Lecture Notes Chapter 9 III. movements at joints flexion extension abduction adduction circumduction rotation inversion eversion protraction retraction supination pronation elevation depression opposition dorsiflexion plantar flexion gliding Strong/Fall 2008 page 3 jAnatomy Lecture Notes Chapter 9 IV. -

Medial Meniscus Anatomy
Quantitative and Qualitative Assessment of the Posterior Medial Meniscus Anatomy Defining Meniscal Ramp Lesions Nicholas N. DePhillipo,*y MS, ATC, OTC, Gilbert Moatshe,yz§ MD, PhD, Jorge Chahla,z MD, PhD, Zach S. Aman,z BA, Hunter W. Storaci,z MSc, Elizabeth R. Morris,z BA, Colin M. Robbins,z BA, Lars Engebretsen,§ MD, PhD, and Robert F. LaPrade,*k MD, PhD Investigation performed at Steadman Philippon Research Institute, Vail, Colorado, USA Background: Meniscal ramp lesions have been defined as a tear of the peripheral attachment of the posterior horn of the medial meniscus (PHMM) at the meniscocapsular junction or an injury to the meniscotibial attachment. Precise anatomic descriptions of these structures are limited in the current literature. Purpose: To quantitatively and qualitatively describe the PHMM and posteromedial capsule anatomy pertaining to the location of a meniscal ramp lesion with reference to surgically relevant landmarks. Study Design: Descriptive laboratory study. Methods: Fourteen male nonpaired fresh-frozen cadavers were used. The locations of the posteromedial meniscocapsular and meniscotibial attachments were identified. Measurements to surgically relevant landmarks were performed with a coordinate measuring system. To further analyze the posteromedial meniscocapsular and meniscotibial attachments, hematoxylin and eosin and alcian blue staining were conducted on a separate sample of 10 nonpaired specimens. Results: The posterior meniscocapsular attachment had a mean 6 SD length of 20.2 6 6.0 mm and attached posteroinferiorly to the PHMM at a mean depth of 36.4% of the total posterior meniscal height. The posterior meniscotibial ligament attached on the PHMM 16.5 mm posterior and 7.7 mm medial to the center of the posterior medial meniscal root attachment.