Posterolateral and Posteromedial Corner Injuries of the Knee
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Synovial Joints Permit Movements of the Skeleton
8 Joints Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes 8.1 Contrast the major categories of joints, and explain the relationship between structure and function for each category. 8.2 Describe the basic structure of a synovial joint, and describe common accessory structures and their functions. 8.3 Describe how the anatomical and functional properties of synovial joints permit movements of the skeleton. © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes (continued) 8.4 Describe flexion/extension, abduction/ adduction, and circumduction movements of the skeleton. 8.5 Describe rotational and special movements of the skeleton. © 2018 Pearson Education, Inc. Module 8.1: Joints are classified according to structure and movement Joints, or articulations . Locations where two or more bones meet . Only points at which movements of bones can occur • Joints allow mobility while preserving bone strength • Amount of movement allowed is determined by anatomical structure . Categorized • Functionally by amount of motion allowed, or range of motion (ROM) • Structurally by anatomical organization © 2018 Pearson Education, Inc. Module 8.1: Joint classification Functional classification of joints . Synarthrosis (syn-, together + arthrosis, joint) • No movement allowed • Extremely strong . Amphiarthrosis (amphi-, on both sides) • Little movement allowed (more than synarthrosis) • Much stronger than diarthrosis • Articulating bones connected by collagen fibers or cartilage . Diarthrosis (dia-, through) • Freely movable © 2018 Pearson Education, Inc. Module 8.1: Joint classification Structural classification of joints . Fibrous • Suture (sutura, a sewing together) – Synarthrotic joint connected by dense fibrous connective tissue – Located between bones of the skull • Gomphosis (gomphos, bolt) – Synarthrotic joint binding teeth to bony sockets in maxillae and mandible © 2018 Pearson Education, Inc. -

Chapter Nine- Joints and Articulations
Chapter 9 Activity: Joints 1. List the three structural categories of joints and briefly describe the criteria used for structural classification of joints. 2. List the three functional classifications of joints, and briefly describe the basis for the functional classification of joints. 3. Which functional class of joints contains joints that are freely movable? 1. Synarthrosis 2. Amphiarthrosis 3. Diarthrosis a) 1 only c) 3 only e) All of these choices b) 2 only d) Both 2 and 3 4. Which of the following is a type of fibrous joint composed of a thin layer of dense irregular fibrous connective tissue found between the bones of the skull? 1. Syndesmoses 2. Gomphosis 3. Suture a) 1 only c) 3 only e) None of these choices b) 2 only d) Both 1 and 2 5. The epiphyseal plate in a long bone is an example of which type of joint? a) Gomphosis c) Symphysis e) Synchondrosis b) Suture d) Synovial 6. The joint between the first rib and the manubrium of the sternum is classified as a) a synchondrosis. c) a cartilaginous joint. e) None of these choices. b) a synarthrosis. d) All of these choices. 7. Which of the following is(are) made from dense regular connective tissue? a) Ligaments c) Articular fat pads e) Synovial fluid b) Articular cartilage d) Synovial membrane 8. What unique characteristics would a person who is "double-jointed” possess? Answer: 9. Briefly describe the functions of synovial fluid. Answer: 10. Briefly describe what is happening when a person “cracks their knuckles”. Answer: 11. Which of the following structures include the fibular and tibial collateral ligaments of the knee joint? a) Synovial membranes c) Menisci e) Tendon sheath b) Articular fat pads d) Extracapsular ligaments 12. -

The Influence of Altered Lower-Extremity Kinematics on Patellofemoral Joint Dysfunction: a Theoretical Perspective
The Influence of Altered Lower-Extremity Kinematics on Patellofemoral Joint Dysfunction: A Theoretical Perspective Christopher M. Powers, PT, PhD 1 Although patellofemoral pain (PFP) is recognized as being one of the most common disorders of It has been recognized by sev- the lower extremity, treatment guidelines and underlying rationales remain vague and controver- eral authors that the patel- sial. The premise behind most treatment approaches is that PFP is the result of abnormal patellar lofemoral joint may be influenced CLINICAL COMMENTARY tracking and/or patellar malalignment. Given as such, interventions typically focus on the joint by the segmental interactions of itself and have traditionally included strengthening the vastus medialis oblique, taping, bracing, the lower extremity.6,7,21,27,34,45 Ab- soft tissue mobilization, and patellar mobilization. More recently, it has been recognized that the normal motion(s) of the tibia and patellofemoral joint and, therefore, PFP may be influenced by the interaction of the segments and femur in the transverse and frontal joints of the lower extremity. In particular, abnormal motion of the tibia and femur in the transverse and frontal planes may have an effect on patellofemoral joint mechanics. With this in planes are believed to have an mind, interventions aimed at controlling hip and pelvic motion (proximal stability) and ankle/foot effect on patellofemoral joint me- motion (distal stability) may be warranted and should be considered when treating persons with chanics and therefore PFP. An un- patellofemoral joint dysfunction. The purpose of this paper is to provide a biomechanical derstanding of how lower- overview of how altered lower-extremity mechanics may influence the patellofemoral joint. -

An Evidence Based Medicine Understanding of Meniscus Injuries and How to Treat Them
An Evidence Based Medicine Understanding of Meniscus Injuries and How to Treat Them Patrick S. Buckley, MD University Orthopaedic Associates June 1, 2019 Disclosures • None www.UOANJ.com Anatomy of the Meniscus • Act as functional extensions of the tibial plateaus to increase depth of tibial articular surface • The meniscotibial attachment contributes to knee stability • Triangular in cross-section Gross Anatomy of the Meniscus • Ultrastructural Anatomy – Primarily Type I collagen (90%) – 70% water – Fiber orientation is circumferential (hoop stressing) Meniscal Vascularity • Relatively avascular • Vascular penetration – 10 - 30% medial – 10 - 25% lateral • Non-vascularized portions gain nutrients from mechanical loading and joint motion Medial Meniscus • Semilunar shape • Thin anterior horn • Broader posterior horn • More stable & less motion than the lateral = tears more often Lateral Meniscus • Almost circular in shape • Intimately associated with the ACL tibial insertion • Posterior horn attachments – Ligament of Humphrey – Ligament of Wrisberg • Lateral meniscus is a more dynamic structure with more motion Main Importance of Menisci • Load transmission • Joint stability Load Bearing / Shock Absorption • MM 50% and 70% LM of load transmitted through mensicus in extension • 85 % at 90° of flexion • Meniscectomy – 50 % decrease in contact area – 20 % less shock absorption www.UOANJ.com Meniscal effect on joint stability • Secondary restraints to anterior tibial translation in normal knees • In an ACL-deficient knee: the posterior horn of the medial meniscus is more important than the lateral meniscus Interaction of ACL and PHMM • Lack of MM in ACLD knees significantly ↑ anterior tibial translation at all knee flexion angles • Think about with high grade pivot! (Levy, JBJS,1982) (Allen, JOR,2000) C9ristiani, AJSM, 2017) Meniscus Function -Now known to be important structure for load distribution and secondary stabilizer to the knee. -

Meniscus Tear
291 North Fireweed Soldotna, AK 99669 907-262-6454 www.kenaipeninsulaortho.com ______________________________________________________________________________________ Orthopaedic Surgeon: Hand and Wrist Specialist: Henry G. Krull, M.D. Edwin D. Vyhmeister, M.D. Meniscus Tear The meniscus is the rubbery, soft cartilage cushion in the knee. There are two of the C-shaped cushions in each knee, a medial (inner) and lateral (outer) meniscus. They sit between the two bones that form the knee joint, and function to cushion and support the knee. The meniscus can tear with injury or degeneration, or a combination of both. The medial meniscus is torn about 10X more frequently than the lateral meniscus. In young people, the meniscus usually tears with an injury. In older people, the cartilage can degenerate (weaken) with age, and can tear with or without an injury; spontaneous tears can occur. Meniscal tears can occur in association with other injuries to the knee. Symptoms: Pain is the usual symptom of complaint with a meniscus tear. There is often a noticeable “pop.” Swelling and stiffness can also occur. Mechanical symptoms are common—clicking, popping, and locking. Sometimes there is just a feeling that something is wrong inside the knee. Pain can be sharp, or can be dull and aching. Meniscus tears do not heal, but sometimes the symptoms dissipate. Chronic, intermittent symptoms is very common. Meniscal tears can cause a feeling of instability, or can cause the knee to buckle or give way. Cause: Injuries, particularly with sports, are a common cause of meniscal tears in young people. As people age, the meniscus tissue weakens through the normal degenerative process, and tears can occur spontaneously, or with simple activities, such as getting up from a chair, and changing direction while walking. -

About Your Knee
OrthoInfo Basics About Your Knee What are the parts of the knee? Your knee is Your knee is made up of four main things: bones, cartilage, ligaments, the largest joint and tendons. in your body Bones. Three bones meet to form your knee joint: your thighbone and one of the (femur), shinbone (tibia), and kneecap (patella). Your patella sits in most complex. front of the joint and provides some protection. It is also vital Articular cartilage. The ends of your thighbone and shinbone are covered with articular cartilage. This slippery substance to movement. helps your knee bones glide smoothly across each other as you bend or straighten your leg. Because you use it so Two wedge-shaped pieces of meniscal cartilage act as much, it is vulnerable to Meniscus. “shock absorbers” between your thighbone and shinbone. Different injury. Because it is made from articular cartilage, the meniscus is tough and rubbery to help up of so many parts, cushion and stabilize the joint. When people talk about torn cartilage many different things in the knee, they are usually referring to torn meniscus. can go wrong. Knee pain or injury Femur is one of the most (thighbone) common reasons people Patella (kneecap) see their doctors. Most knee problems can be prevented or treated with simple measures, such as exercise or Articular cartilage training programs. Other problems require surgery Meniscus to correct. Tibia (shinbone) 1 OrthoInfo Basics — About Your Knee What are ligaments and tendons? Ligaments and tendons connect your thighbone Collateral ligaments. These are found on to the bones in your lower leg. -

Anterior (Cranial) Cruciate Ligament Rupture
Cranial Cruciate Ligament Rupture in Dogs The cruciate ligaments are tough fibrous bands that connect the distal femur (thigh bone) to the proximal tibia (shin bone). Two cruciate ligaments, the cranial (anterior) and the posterior cruciate ligaments, are found in the knee joint of dogs and cats (and most other domestic animals). These ligaments work like a hinge joint in the knee and are responsible for providing anterior-posterior stability to the knee joint. Normal Knee Joint of a Dog Rupture of the cranial cruciate ligament is rare in cats. It occurs frequently in overweight, middle- and older-aged dogs. Certain dog breeds appear to be predisposed to cranial cruciate ligament rupture. Most commonly, the cocker spaniel and rottweiler are affected. The miniature and toy poodle, Lhasa apso, bichon frise, golden retriever, Labrador retriever, German shepherd and mastiff seem to be predisposed as well. The normal knee joint works as a hinge, keeping the knee stable as it bends. Tearing of the cranial cruciate ligament causes instability of the knee joint and it ceases to function properly. Most cranial cruciate ligament tears in dogs occur gradually, resulting in a low-level lameness that may or nay not improve over time. After the ligament tears, inflammation occurs within the joint. Continued use and weight bearing by the dog often causes the ligament to rupture completely. Dogs that rupture one cruciate ligament have about a fifty percent chance of rupturing the other. Normal Knee Joint of a Dog Rupture of the cranial cruciate ligament in dogs can also occur acutely. Similar to cranial cruciate ligament rupture in humans, resulting from athletic injuries to the knee, dogs can tear this ligament by jumping up to catch a ball or Frisbee or by jumping out of a truck or off a porch. -

Joints Classification of Joints
Joints Classification of Joints . Functional classification (Focuses on amount of movement) . Synarthroses (immovable joints) . Amphiarthroses (slightly movable joints) . Diarthroses (freely movable joints) . Structural classification (Based on the material binding them and presence or absence of a joint cavity) . Fibrous mostly synarthroses . Cartilagenous mostly amphiarthroses . Synovial diarthroses Table of Joint Types Functional across Synarthroses Amphiarthroses Diarthroses (immovable joints) (some movement) (freely movable) Structural down Bony Fusion Synostosis (frontal=metopic suture; epiphyseal lines) Fibrous Suture (skull only) Syndesmoses Syndesmoses -fibrous tissue is -ligaments only -ligament longer continuous with between bones; here, (example: radioulnar periosteum short so some but not interosseous a lot of movement membrane) (example: tib-fib Gomphoses (teeth) ligament) -ligament is periodontal ligament Cartilagenous Synchondroses Sympheses (bone united by -hyaline cartilage -fibrocartilage cartilage only) (examples: (examples: between manubrium-C1, discs, pubic epiphyseal plates) symphesis Synovial Are all diarthrotic Fibrous joints . Bones connected by fibrous tissue: dense regular connective tissue . No joint cavity . Slightly immovable or not at all . Types . Sutures . Syndesmoses . Gomphoses Sutures . Only between bones of skull . Fibrous tissue continuous with periosteum . Ossify and fuse in middle age: now technically called “synostoses”= bony junctions Syndesmoses . In Greek: “ligament” . Bones connected by ligaments only . Amount of movement depends on length of the fibers: longer than in sutures Gomphoses . Is a “peg-in-socket” . Only example is tooth with its socket . Ligament is a short periodontal ligament Cartilagenous joints . Articulating bones united by cartilage . Lack a joint cavity . Not highly movable . Two types . Synchondroses (singular: synchondrosis) . Sympheses (singular: symphesis) Synchondroses . Literally: “junction of cartilage” . Hyaline cartilage unites the bones . Immovable (synarthroses) . -

Closure of Patellar Tendon Defect in ACL Reconstruction
Systematic Review Closure of Patellar Tendon Defect in Anterior Cruciate Ligament Reconstruction With BoneePatellar TendoneBone Autograft: Systematic Review of Randomized Controlled Trials Rachel M. Frank, M.D., Randy Mascarenhas, M.D., Marc Haro, M.D., Nikhil N. Verma, M.D., Brian J. Cole, M.D., M.B.A., Charles A. Bush-Joseph, M.D., and Bernard R. Bach Jr., M.D. Purpose: This study aimed to systematically review the highest level of evidence on anterior cruciate ligament (ACL) reconstruction with boneepatellar tendonebone (BPTB) autografts with patellar tendon defect closure versus no closure after surgery. Methods: We performed a systematic review of multiple medical databases using Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Level I and Level II randomized controlled trials comparing patellar tendon defect closure to no closure during ACL reconstruction with BPTB autografts were included. Two inde- pendent reviewers analyzed all studies. Descriptive statistics were calculated. Study methodological quality was analyzed using the Modified Coleman Methodology Score (MCMS) and Jadad scale. Results: Four studies with a combined 221 patients (154 male patients and 67 female patients) with an average age of 26.6 Æ 2.4 years (range, 17 to 54 years) were included. All studies randomized patients before surgery into ACLR with BPTB autografts either with patellar tendon defect closure or without closure. There were no differences in clinical outcomes (Lysholm score, Tegner scale, International Knee Documentation Committee [IKDC] classification, modified Larsen score, and Lauridsen rating) between groups. There were no significant differences in knee pain between groups. All studies reported imaging findings of the patellar tendon defect, with 2 studies showing no difference in appearance between groups, one study showing excessive scar formation with defect repair, and one study showing improved restoration of normal tendon appearance with defect repair. -
NOTES: Joints and Types of Movements, Continued (Ch 7, Part 4)
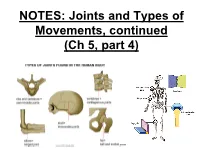
NOTES: Joints and Types of Movements, continued (Ch 5, part 4) *Joints are functional junctions between bones. TYPES OF JOINTS **Joints can be classified according to the type of tissue that binds the bones together.** FIBROUS JOINTS: • bones at fibrous joints are tightly joined by a layer of dense connective tissue. • little or no movement occurs at a fibrous joint • Example: the sutures between the flat bones of the skull CARTILAGINOUS JOINTS: • a layer of hyaline cartilage, or fibrocartilage, joins bones of cartilaginous joints • allow limited movement • Example: the joints that separate the vertebrae SYNOVIAL JOINTS: • most joints in the body are synovial joints • allow free movement • bones at synovial joints are covered with hyaline cartilage (“articular cartilage”) and held together by a fibrous JOINT CAPSULE. SYNOVIAL JOINTS: • the joint capsule consists of an outer layer of ligaments and an inner lining of synovial membrane (which secretes synovial fluid to lubricate the joint). • some synovial joints have flattened, shock- absorbing pads of fibrocartilage called MENISCI between the articulating surfaces of the bones SYNOVIAL JOINTS: • some synovial joints may also have BURSAE, which are fluid-filled sacs located between the skin and the underlying bony prominences. • Example: at the knee joint, the patella is sandwiched between 2 bursae. TYPES OF SYNOVIAL JOINTS: • Ball-and-socket - round head of one bone rests within a cup-shaped depression of another - all angular and rotational movements, including circumduction can be performed by this joint TYPES OF SYNOVIAL JOINTS: • Gliding (planar) – Have flattened or slightly curved faces – Flat articular surfaces slide across one another – Amount of movements is slightly TYPES OF SYNOVIAL JOINTS: • Condylar (ellipsoid) – Oval articular face nests within a depression in opposing surface – Angular movements occur in 2 planes: along or across length of oval TYPES OF SYNOVIAL JOINTS: • Hinge – Permits angular motion in single plane (e.g. -

Musculoskeletal Morphing from Human to Mouse
Procedia IUTAM Procedia IUTAM 00 (2011) 1–9 2011 Symposium on Human Body Dynamics Musculoskeletal Morphing from Human to Mouse Yoshihiko Nakamuraa,∗, Yosuke Ikegamia, Akihiro Yoshimatsua, Ko Ayusawaa, Hirotaka Imagawaa, and Satoshi Ootab aDepartment of Mechano-Informatics, Graduate School of Information and Science and Technology, University of Tokyo, 7-3-1, Hongo, Bunkyo-ku, Tokyo, Japan bBioresource Center, Riken, 3-1-1 Takanodai, Tsukuba-shi, Ibaragi, Japan Abstract The analysis of movement provides various insights of human body such as biomechanical property of muscles, function of neural systems, physiology of sensory-motor system, skills of athletic movements, and more. Biomechan- ical modeling and robotics computation have been integrated to extend the applications of musculoskeletal analysis of human movements. The analysis would also provide valuable means for the other mammalian animals. One of current approaches of post-genomic research focuses to find connections between the phenotype and the genotype. The former means the visible morphological or behavioral expression of an animal, while the latter implies its genetic expression. Knockout mice allows to study the developmental pathway from the genetic disorders to the behavioral disorders. Would musculoskeletal analysis of mice also offer scientific means for such study? This paper reports our recent technological development to build the musculoskeletal model of a laboratory mouse. We propose mapping the musculoskeletal model of human to a laboratory mouse based on the morphological similarity between the two mammals. Although the model will need fine adjustment based on the CT data or else, we can still use the mapped musculoskeletal model as an approximate model of the mouse’s musculoskeletal system. -

Avulsion of the Anterior Lateral Meniscal Root Secondary to Tibial Eminence Fracture
Avulsion of the Anterior Lateral Meniscal Root Secondary to Tibial Eminence Fracture Publish date: May 8, 2018 Authors: Travis J. Menge, MD Jorge Chahla, MD Justin J. Mitchell, MD Chase S. Dean, MD and Robert F. LaPrade, MD Author Affiliation | Disclosures Authors’ Disclosure Statement: Dr. LaPrade reports that he receives royalties and is a paid consultant for Smith and Nephew, Arthrex, and Össur. Dr. Menge reports that he is a paid consultant for Smith and Nephew. Dr. Mitchell reports that he has received educational and grant support from Arthrex, Smith and Nephew, and DJO, LLC. The other authors report no actual or potential conflict of interest in relation to this article. Dr. Menge is an Orthopaedic and Sports Medicine Surgeon, Spectrum Health Medical Group, Grand Rapids, Michigan. Dr. Mitchell is an Orthopaedic and Sports Medicine Surgeon, Gundersen Health System, La Crosse, Wisconsin. Dr. Chahla is a Clinical Fellow, Cedars Sinai Kerlan Jobe Institute, Santa Monica, California. Dr. Dean is an Orthopaedic Surgical Resident, University of Colorado Hospital, Denver, Colorado. Dr. LaPrade is an Orthopaedic Complex Knee and Sports Medicine Surgeon, and Chief Medical Officer and Co-Director of the Sports Medicine Fellowship, Steadman Philippon Research Institute, The Steadman Clinic, Vail, Colorado. Address correspondence to: Robert F. LaPrade MD, PhD, Steadman Philippon Research Institute, The Steadman Clinic, 181 West Meadow Drive, Suite 400, Vail, Colorado 81657 (email, [email protected]). Am J Orthop. 2018;47(5). Copyright Frontline Medical Communications Inc. 2018. All rights reserved. Take-Home Points Root tears of all meniscal attachments have been described. A comprehensive anatomic understanding of the meniscal roots is of utmost importance to suspect root lesions.