Chps) District-Level Evaluation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Home Office, United Kingdom
GHANA COUNTRY ASSESSMENT APRIL 2002 COUNTRY INFORMATION & POLICY UNIT IMMIGRATION & NATIONALITY DIRECTORATE HOME OFFICE, UNITED KINGDOM CONTENTS I. Scope of Document 1.1 - 1.5 II. Geography 2.1 - 2.2 Economy 2.3 III. History 3.1 - 3.2 IV. State Structures The Constitution 4.1 - 4.3 Political System 4.4 - 4.8 Judiciary 4.9 - 4.15 Military 4.16 (i) National Service 4.17 Internal Security 4.18 - 4.22 Legal Rights/Detention 4.23 - 4.24 Prisons and Prison conditions 4.25 - 4.30 Medical Services 4.31 - 4.38 Educational System 4.39 - 4.41 V. Human Rights V.A Human Rights Issues Overview 5.1 - 5.4 Freedom of Speech and the Media 5.5 - 5.11 Freedom of Religion 5.12 - 5.19 Freedom of Assembly & Association 5.20 - 5.25 Employment Rights 5.26 - 5.28 People Trafficking 5.29 - 5.34 Freedom of Movement 5.35 - 5.36 V.B Human Rights - Specific Groups Women 5.37 - 5.43 (i) Female Genital Mutilation (FGM) 5.44 - 5.45 (ii) The Trokosi system 5.46 - 5.48 Children 5.49 - 5.55 Ethnic Groups 5.56 - 5.60 Homosexuals 5.61 V.C Human Rights - Other Issues Non-Government Organisations (NGOs) 5.62 Annexes: Chronology of Events Political Organisations Prominent People References to Source Material I. Scope of Document 1.1. This assessment has been produced by the Country Information & Policy Unit, Immigration & Nationality Directorate, Home Office, from information obtained from a variety of sources. 1.2. The assessment has been prepared for background purposes for those involved in the asylum determination process. -

Ghana), 1922-1974
LOCAL GOVERNMENT IN EWEDOME, BRITISH TRUST TERRITORY OF TOGOLAND (GHANA), 1922-1974 BY WILSON KWAME YAYOH THESIS SUBMITTED TO THE SCHOOL OF ORIENTAL AND AFRICAN STUDIES, UNIVERSITY OF LONDON IN PARTIAL FUFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY DEPARTMENT OF HISTORY APRIL 2010 ProQuest Number: 11010523 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest ProQuest 11010523 Published by ProQuest LLC(2018). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC. ProQuest LLC. 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106- 1346 DECLARATION I have read and understood regulation 17.9 of the Regulations for Students of the School of Oriental and African Studies concerning plagiarism. I undertake that all the material presented for examination is my own work and has not been written for me, in whole or part by any other person. I also undertake that any quotation or paraphrase from the published or unpublished work of another person has been duly acknowledged in the work which I present for examination. SIGNATURE OF CANDIDATE S O A S lTb r a r y ABSTRACT This thesis investigates the development of local government in the Ewedome region of present-day Ghana and explores the transition from the Native Authority system to a ‘modem’ system of local government within the context of colonization and decolonization. -

The Politics of Accountability in Ghana's National
RESEARCH BRIEFING JUNE 2016 WHEN DOES THE STATE LISTEN? 1 16 How does governmentIDS_Master Logo responsiveness come about? The politics of accountability in Ghana’s National Health Insurance Scheme TERENCE DARKO RESEARCH How does government responsiveness come about? BRIEFING The politics of accountability in Ghana’s National Health Insurance Scheme Author Terence Darko is a Researcher at Capacity Development Consult (CDC), a Ghanaian-based research and consulting firm. He has an MA in Social Policy Studies from the University of Ghana. Before joining CDC, he worked with Innovations for Poverty Action Ghana and the Institute of Statistical, Social and Economic Research, Ghana. His research interests include policy processes, the politics of social development, social protection, citizen participation and political accountability. Email: [email protected] Production credits Production editor: Catherine Setchell, Making All Voices Count, [email protected] Copyeditor: Karen Brock, Green Ink, [email protected] Designer: Lance Bellers, [email protected] Further reading This research briefing forms part of a wider research project called When Does the State Listen? led by the Institute of Development Studies and funded by the Making All Voices Count initiative. The other briefs from this research project are: Cassim, A. (2016) What happens to policy when policy champions move on? The case of welfare 2 in South Africa, Brighton: IDS 16 Katera, L. (2016) Why is it so hard for non-state actors to be heard? Inside Tanzania’s education policies, Brighton: IDS Loureiro, M; Cassim, A; Darko, T; Katera, L; and Salome, N. (2016) ‘When Does the State Listen?’ IDS Bulletin Vol 47 No. -

A Case Comparison of Ghana, Kenya, and Senegal
1 Democratization and Universal Health Coverage: A Case Comparison of Ghana, Kenya, and Senegal Karen A. Grépin and Kim Yi Dionne This article identifies conditions under which newly established democracies adopt Universal Health Coverage. Drawing on the literature examining democracy and health, we argue that more democratic regimes – where citizens have positive opinions on democracy and where competitive, free and fair elections put pressure on incumbents – will choose health policies targeting a broader proportion of the population. We compare Ghana to Kenya and Senegal, two other countries which have also undergone democratization, but where there have been important differences in the extent to which these democratic changes have been perceived by regular citizens and have translated into electoral competition. We find that Ghana has adopted the most ambitious health reform strategy by designing and implementing the National Health Insurance Scheme (NHIS). We also find that Ghana experienced greater improvements in skilled attendance at birth, childhood immunizations, and improvements in the proportion of children with diarrhea treated by oral rehydration therapy than the other countries since this policy was adopted. These changes also appear to be associated with important changes in health outcomes: both infant and under-five mortality rates declined rapidly since the introduction of the NHIS in Ghana. These improvements in health and health service delivery have also been observed by citizens with a greater proportion of Ghanaians reporting satisfaction with government handling of health service delivery relative to either Kenya or Senegal. We argue that the democratization process can promote the adoption of particular health policies and that this is an important mechanism through which democracy can improve health. -

Interest Groups, Issue Definition and the Politics of Healthcare in Ghana
CORE Metadata, citation and similar papers at core.ac.uk Provided by International Institute for Science, Technology and Education (IISTE): E-Journals Public Policy and Administration Research www.iiste.org ISSN 2224-5731(Paper) ISSN 2225-0972(Online) Vol.4, No.6, 2014 Interest Groups, Issue Definition and the Politics of Healthcare in Ghana Edward Brenya 1* Samuel Adu-Gyamfi 2 1. History and Political Studies, Kwame Nkrumah University of Science and Technology, PMB, Kumasi Ashanti, Ghana 2. History and Political Studies, Kwame Nkrumah University of Science and Technology, PMB, Kumasi Ashanti, Ghana *Email of corresponding author: [email protected] Abstract The provision of healthcare in Ghana from the pre-colonial period to the 4 th Republic has been characterized by struggles to maintain dominance. While the politics in the pre-independence period focused on the manner of providing healthcare, the post-independence period encapsulates healthcare financing. Using the interest groups theory, the study examines the manner and motive of healthcare management in Ghana. The study finds that a coalition of healthcare interest groups often comprising healthcare providers, government functionaries, bureaucrats, and the World Bank and IMF etc., (from the 1970s), uses the definition of healthcare management to maintain leverage in the management of healthcare. Healthcare management in the pre-colonial period was defined as interventionism while the colonial administration focused on scientific therapy. The post-colonial period witnessed a shift of focus to healthcare financing and Nkrumah’ government adopted free healthcare system financed by the state. The Busia’s government focused on sustainability based on payment of small user fee. -

RSPO NEW Planting Procedures Summary Report of SEIA and HCV Assessment
RSPO Roundtable on Sustainable Palm Oil RSPO NEW Planting Procedures Summary Report of SEIA and HCV Assessment SG Sustainable Oils Limited, Brewaniase, Nkwanta South District of the Volta Region, Republic of Ghana. 1.0 Executive Summary SG Sustainable Oils Ghana Ltd (SGSOG), a wholly owned subsidiary of Herakles Farms, is developing approximately 3,715 hectares of sustainable oil palm plantations in Republic of Ghana. SGSOG was incorporated within Ghana in 2008. SGSOG is a subsidiary of Herakles Farms, which was previously known as SG Sustainable Oils (SGSO). SGSO has been a member of RSPO since March 2008, and recently an application by the parent company to RSPO for its membership to be recognized under Herakles Farms has been approved. The company’s palm oil estate is located in the Volta Region, near the village of Brewaniase, Nkwanta South District, Republic of Ghana. This document outlines the Social and Environmental Impact Assessment (SEIA) and High Conservation Value (HCV) Assessment process and documentation for SGSOG’s oil palm development summarized by assessors from SAL Consult Limited and Ghana Wildlife Society. A comprehensive and participatory independent SEIA and HCV Assessment which included internal and external stakeholders were completed. The results incorporated into planning, management and operational ongoing work. The independent assessments recognised the following: There was no primary forest in the location. All area required to maintain or enhance one or more HCV. There was no peat soil identified. All peoples’ private land. Abbreviations Used EIA Environmental Impact Assessment EPA Environmental Protection Agency HCV High Conservation Value IUCN International Union for Conservation of Nature RSPO Roundtable on Sustainable Palm Oil SGSOG SG Sustainable Oils Ghana SEIA Social and Environmental Impact Assessment SIA Social Impact Assessment 2.0 Scope of SEIA and HCV Assessment SG Sustainable Oils Ghana Ltd (SGSOG) is a wholly owned subsidiary of Herakles Farms. -

Misconceptions, Misinformation and Politics of COVID-19 on Social Media: a Multi-Level Analysis in Ghana
ORIGINAL RESEARCH published: 05 May 2021 doi: 10.3389/fcomm.2021.613794 Misconceptions, Misinformation and Politics of COVID-19 on Social Media: A Multi-Level Analysis in Ghana Philip Teg-Nefaah Tabong 1* and Martin Segtub 2 1 Department of Social and Behavioural Sciences, School of Public Health, College of Health Sciences, University of Ghana Legon, Accra, Ghana, 2 Department of Communication Studies, University of Professional Studies, Accra, Ghana Background: Ghana developed an Emergency Preparedness and Response Plan (EPRP) in response to the Severe Acute Respiratory Syndrome Coronavirus (SARS CoV-2) pandemic. A key strategy in the EPRP is to mobilize national resources and put in place strategies for improved risk and behavioral change communication. Nonetheless, concerns have been raised on social media about COVID-19 misinformation and misconceptions. This study used social media content to determine the types, forms and the effects of the myths, misconceptions and misinformation in Ghana’s COVID-19 containment. Method: The study was conducted in three phases involving the use of both primary and secondary data. Review of social media information on COVID-19 was done. This was complemented with document review and interviews with key stakeholders with expertise in the management of public health emergencies and mass communication Edited by: experts (N = 18). All interviews were transcribed verbatim and analyzed using NVivo 12. Fredrick Ogenga, Rongo University, Kenya Results: The study showed a changing pattern in the misconceptions and Reviewed by: misinformation about COVID-19. Initially myths were largely on causes and vulnerability. Rasha El-Ibiary, It was widely speculated that black people had some immunity against COVID-19. -
Volta Region
REGIONAL ANALYTICAL REPORT VOLTA REGION Ghana Statistical Service June, 2013 Copyright © 2013 Ghana Statistical Service Prepared by: Martin K. Yeboah Augusta Okantey Emmanuel Nii Okang Tawiah Edited by: N.N.N. Nsowah-Nuamah Chief Editor: Nii Bentsi-Enchill ii PREFACE AND ACKNOWLEDGEMENT There cannot be any meaningful developmental activity without taking into account the characteristics of the population for whom the activity is targeted. The size of the population and its spatial distribution, growth and change over time, and socio-economic characteristics are all important in development planning. The Kilimanjaro Programme of Action on Population adopted by African countries in 1984 stressed the need for population to be considered as a key factor in the formulation of development strategies and plans. A population census is the most important source of data on the population in a country. It provides information on the size, composition, growth and distribution of the population at the national and sub-national levels. Data from the 2010 Population and Housing Census (PHC) will serve as reference for equitable distribution of resources, government services and the allocation of government funds among various regions and districts for education, health and other social services. The Ghana Statistical Service (GSS) is delighted to provide data users with an analytical report on the 2010 PHC at the regional level to facilitate planning and decision-making. This follows the publication of the National Analytical Report in May, 2013 which contained information on the 2010 PHC at the national level with regional comparisons. Conclusions and recommendations from these reports are expected to serve as a basis for improving the quality of life of Ghanaians through evidence-based policy formulation, planning, monitoring and evaluation of developmental goals and intervention programs. -
Expanded PDF Profile
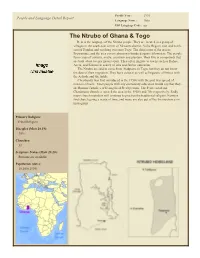
Profile Year: 1993 People and Language Detail Report Language Name: Delo ISO Language Code: ntr The Ntrubo of Ghana & Togo Delo is the language of the Ntrubo people. They are located in a group of villages in the south-east corner of Nkwanta district, Volta Region, east and north- east of Dambai and reaching over into Togo. The chief town of the area is Brewaniase, and the area covers about two-hundred square kilometers. The people farm crops of cassava, maize, cocoyam and plantain. They live in compounds that are built about twenty meters apart. They often migrate to towns such as Hohoe, Accra, and Kumasi in search of jobs and further education. The Ntrubo are said to come from Atakpame in Togo, but they do not know the date of their migration. They have cultural as well as linguistic affinities with the Achode and the Adele. Christianity was first introduced in the 1950's with the post war spread of mission schools. Most people with any elementary education would say that they are Roman Catholics or Evangelical Presbyterians. The Pentecostal and Charismatic churches entered the area in the 1960's and 70's respectively. Sadly many church members still continue to practice the traditional religion. Farmers find church going a waste of time, and many are also put off by the insistence on monogamy. Primary Religion: Tribal Religion Disciples (Matt 28.19): 30% Churches: 33 Scripture Status (Matt 28.20): Portions are available Population (date): 10,100 (1995) The Ntrubo of Ghana & Togo Item Name Item Note Have They Heard The Gospel? Profile Summary Call Themselves Christian (%) 30% Believe In Jesus As God & Only Savior (%) 30% Number Of Pastors 20 Number Of Communities There are 9 listed Ntrubo localities Number Of Churches 33 Is The Word Of God Translated? Yes - Portions. -

Working Paper Cover
WORKING PAPER UNICEF GOOD PRACTICES IN INTEGRATING BIRTH REGISTRATION INTO HEALTH SYSTEMS (2000-2009) CASE STUDIES: BANGLADESH, BRAZIL, THE GAMBIA AND DELHI, INDIA JANUARY 2010 Fall08 WORKING PAPER UNICEF GOOD PRACTICES IN INTEGRATING BIRTH REGISTRATION INTO HEALTH SYSTEMS (2000–2009) CASE STUDIES: BANGLADESH, BRAZIL, THE GAMBIA AND DELHI, INDIA Mariana Muzzi JANUARY 2010 UNICEF Good Practices in Integrating Birth Registration into Health Systems (2000–2009); Case Studies: Bangladesh, Brazil, the Gambia and Delhi, India © United Nations Children‟s Fund (UNICEF), New York, 2009 UNICEF 3 UN Plaza, NY, NY 10017 December, 2009 This is a working document. It has been prepared to facilitate the exchange of knowledge and to stimulate discussion. The text has not been edited to official publication standards and UNICEF accepts no responsibility for errors. The designations in this publication do not imply an opinion on legal status of any country or territory, or of its authorities, or the delimitation of frontiers. About the author Mariana Muzzi is a Brazilian-Finnish political scientist who has worked on child protection and human rights issues since 2001 with the International Organization for Migration, the European Union, UNICEF, non-govermental organizations and research institutes in several countries, including Belgium, Bolivia, Brazil, India, Peru, and the United States. She has been published in English and Spanish in the fields of birth registration, counter-trafficking in human beings, domestic violence prevention, sexual exploitation of children, juvenile justice, children’s rights and public health. Recent research initiatives include Children in Administrative Detention in India (2009), Child Protection and Islam (2008), and State Obligations vis-à- vis the Right to Health: Child Abuse and the Health-System based Child Abuse Attention Modules in Peru (2006). -

Download Date 28/09/2021 19:08:59
Ghana: From fragility to resilience? Understanding the formation of a new political settlement from a critical political economy perspective Item Type Thesis Authors Ruppel, Julia Franziska Rights <a rel="license" href="http://creativecommons.org/licenses/ by-nc-nd/3.0/"><img alt="Creative Commons License" style="border-width:0" src="http://i.creativecommons.org/l/by- nc-nd/3.0/88x31.png" /></a><br />The University of Bradford theses are licenced under a <a rel="license" href="http:// creativecommons.org/licenses/by-nc-nd/3.0/">Creative Commons Licence</a>. Download date 28/09/2021 19:08:59 Link to Item http://hdl.handle.net/10454/15062 University of Bradford eThesis This thesis is hosted in Bradford Scholars – The University of Bradford Open Access repository. Visit the repository for full metadata or to contact the repository team © University of Bradford. This work is licenced for reuse under a Creative Commons Licence. GHANA: FROM FRAGILITY TO RESILIENCE? J.F. RUPPEL PHD 2015 Ghana: From fragility to resilience? Understanding the formation of a new political settlement from a critical political economy perspective Julia Franziska RUPPEL Submitted for the Degree of Doctor of Philosophy Faculty of Social Sciences and Humanities University of Bradford 2015 GHANA: FROM FRAGILITY TO RESILIENCE? UNDERSTANDING THE FORMATION OF A NEW POLITICAL SETTLEMENT FROM A CRITICAL POLITICAL ECONOMY PERSPECTIVE Julia Franziska RUPPEL ABSTRACT Keywords: Critical political economy; electoral politics; Ghana; political settle- ment; power relations; social change; statebuilding and state formation During the late 1970s Ghana was described as a collapsed and failed state. In contrast, today it is hailed internationally as beacon of democracy and stability in West Africa. -

A Political Economy of Social Protection Policy Uptake in Ghana
Advancing research excellence for governance and public policy in Africa PASGR Working Paper 008 A Political Economy of Social Protection Policy Uptake in Ghana de-Graft Aikins, Ama University of Ghana Alidu, Seidu University of Ghana Aryeetey, Ellen Bortei-Doku University of Ghana Domfe, George University of Ghana Armar , Ralph University of Ghana Koram , Mary Eve Independent Researcher, Legon Accra January , 2016 This report was produced in the context of a multi-country study on the ‘Political Economy Analysis of So- cial Protection Policy Uptake in Africa’, generously supported by the UK Department for International De- velopment (DFID) through the Partnership for African Social and Governance Research (PASGR). The views herein are those of the authors and do not necessarily represent those held by PASGR or DFID. Author contact information: Ama de-Graft Aikins University of Ghana [email protected] de-Graft Aikins, A., Alidu, S., Aryeetey,E. B., Domfe, G., Armah, R., & Koram, M. (2016). A Political Econo- my of Social Protection Policy Uptake in Ghana.Partnership for African Social and Governance Re- search Working Paper No. 008, Nairobi, Kenya. ©Partnership for African Social & Governance Research, 2015 Nairobi, Kenya [email protected] www.pasgr.org ISBN 978-9966-087-40-9 Contents List of Tables ........................................................................................................................... 2 List of Figures ........................................................................................................................