Robotic-Assisted Laparoscopic Radical Prostatectomy After Aborted Retropubic Radical Prostatectomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Quality of Life Outcomes After Brachytherapy for Early Prostate Cancer
Prostate Cancer and Prostatic Diseases (1999) 2 Suppl 3, S19±S20 ß 1999 Stockton Press All rights reserved 1365±7852/99 $15.00 http://www.stockton-press.co.uk/pcan Quality of life outcomes after brachytherapy for early prostate cancer MS Litwin1, JM Brandeis1, CM Burnison1 and E Reiter1 1UCLA Departments of Urology, Health Services, and Radiation Oncology, UCLA, California, USA Despite the absence of empirical evidence, there is a XRT. Sildena®l appeared to have little effect in the radical popular perception that brachytherapy results in less prostatectomy patients. However, brachytherapy patients impairment of health-related quality of life. This study not receiving hormonal ablation or XRT who took silde- compared general and disease-speci®c health-related na®l had better sexual function and bother scores than quality of life in men who had undergone either brachy- those patients who did not. therapy (with and without pre-treatment XRT) or radical prostatectomy, and in healthy age-matched controls. Method Conclusion We surveyed all patients with clinical T2 or less prostate General health-related quality of life did not differ greatly cancer who had undergone interstitial seed brachyther- between the three groups, but there were variations in apy at UCLA during the previous 3±17 months. Each was disease-speci®c (urinary, bowel and sexual) health-related paired with two randomly selected, temporally matched quality of life. Radical prostatectomy patients had the radical prostatectomy patients. Healthy, age-matched worst urinary function (leakage), but brachytherapy controls were drawn from the literature. Surgery and patients were also signi®cantly worse than the controls. -

Prostate Biopsy in the Staging of Prostate Cancer
Prostate Cancer and Prostatic Diseases (1997) 1, 54±58 ß 1997 Stockton Press All rights reserved 1365±7852/97 $12.00 Review Prostate Biopsy in the staging of prostate cancer L Salomon, M Colombel, J-J Patard, D Gasman, D Chopin & C-C Abbou Service d'Urologie, CHU, Henri Mondor, CreÂteil, France The use of prostate biopsies was developed in parallel with progress in our knowledge of prostate cancer and the use of prostate-speci®c antigen (PSA). Prostate biopsies were initially indicated for the diagnosis of cancer, by the perineal approach under general anesthesia. Nowadays prostate biopsies are not only for diagnostic purposes but also to determine the prognosis, particularly before radical prostatectomy. They are performed in patients with elevated PSA levels, by the endorectal approach, sometimes under local anesthesia.(1±3) The gold standard is the sextant biopsy technique described by Hodge4,5, which is best to diagnose prostate cancer, particularly in case of T1c disease (patients with serum PSA elevation).6±13 Patients with a strong suspicion of prostate cancer from a negative series of biopsies can undergo a second series14;15 with transition zone biopsy16,17 or lateral biopsy.18,19 Karakiewicz et al 20 and Uzzo et al 21 proposed that the number of prostate biopsies should depend on prostate volume to improve the positivity rate. After the diagnosis of prostate cancer, initial therapy will depend on several prognostic factors. In the case of radical prostatectomy, the results of sextant biopsy provide a wealth of information.22,23 The aim of this report is to present the information given by prostate biopsy in the staging of prostate cancer. -

Needle Biopsy and Radical Prostatectomy Specimens David J Grignon
Modern Pathology (2018) 31, S96–S109 S96 © 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 Prostate cancer reporting and staging: needle biopsy and radical prostatectomy specimens David J Grignon Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, IUH Pathology Laboratory, Indianapolis, IN, USA Prostatic adenocarcinoma remains the most common cancer affecting men. A substantial majority of patients have the diagnosis made on thin needle biopsies, most often in the absence of a palpable abnormality. Treatment choices ranging from surveillance to radical prostatectomy or radiation therapy are largely driven by the pathologic findings in the biopsy specimen. The first part of this review focuses on important morphologic parameters in needle biopsy specimens that are not covered in the accompanying articles. This includes tumor quantification as well as other parameters such a extraprostatic extension, seminal vesicle invasion, perineural invasion, and lymphovascular invasion. For those men who undergo radical prostatectomy, pathologic stage and other parameters are critical in prognostication and in determining the appropriateness of adjuvant therapy. Staging parameters, including extraprostatic extension, seminal vesicle invasion, and lymph node status are discussed here. Surgical margin status is also an important parameter and definitions and reporting of this feature are detailed. Throughout the article the current reporting guidelines published by the College of American Pathologists and the International Collaboration on Cancer Reporting are highlighted. Modern Pathology (2018) 31, S96–S109; doi:10.1038/modpathol.2017.167 The morphologic aspects of prostatic adenocarcinoma hormonal therapy.4,5 For needle biopsy specimens the have a critical role in the management and prognos- data described below are largely based on standard tication of patients with prostatic adenocarcinoma. -

Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis
www.kjurology.org DOI:10.4111/kju.2010.51.1.70 Case Report Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis Kyung Hwa Choi, Seung Hwan Lee, Won Sug Jung1, Byung Ha Chung Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, 1National Health Insurance Corporation Ilsan Hospital, Goyang, Korea We report a rare case of robot-assisted laparoscopic radical prostatectomy (RARP) in Article History: a patient with a preexisting penile prosthesis. In this case, we completed RARP without received 27 August, 2009 14 October, 2009 removing the reservoir by using a deflation-inflation technique, and there were no com- accepted plications related to the prosthesis. The patient had a negative surgical margin. The Corresponding Author: preserved three-piece inflatable penile prosthesis continued to function properly in 1 Byung Ha Chung month. Reservoir-preserving RARP is technically feasible and safe. However, it is im- Department of Urology, Yonsei portant to be aware of device-related complications. Long-term studies on the mechan- University Health System, Gangnam Severance Hospital, 712, Eonju-ro, ical survival rate and patient satisfaction should be also performed. Dogok-dong, Gangnam-gu, Seoul Key Words: Robotics, Prostatectomy, Penile prosthesis, Prostatic neoplasms 135-720, Korea TEL: +82-2-2019-3474 FAX: +82-2-3462-8887 E-mail: [email protected] Prostate cancer has been reported to occur most frequently CASE REPORT in men over 40 years of age. In organ-confined cases, radical prostatectomy is the treatment of choice. After the in- 1. Patient troduction of the da VinciⓇ surgical system (Intuitive The patient was a 64-year-old male diagnosed with aci- Surgical, Sunnyvale, USA), robot-assisted laparoscopic nar-type prostate adenocarcinoma with a Gleason score of radical prostatectomy (RARP) has become a mainstay of 6 (3+3) by prostate biopsy. -
Quality of Life After Open Or Robotic Prostatectomy, Cryoablation Or
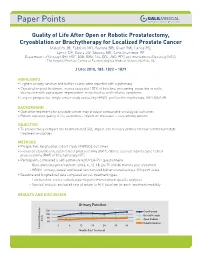
Quality of Life After Open or Robotic Prostatectomy, Cryoablation or Brachytherapy for Localized Prostate Cancer Malcolm JB, Fabrizio MD, Barone BB, Given RW, Lance RS, Lynch DF, Davis JW, Shaves ME, Schellhammer PF Departments of Urology (JBM, MDF, BBB, RWG, RSL, DFL, JWD, PFS) and Interventional Radiology (MES), The Virginia Prostate Center at Eastern Virginia Medical School, Norfolk, VA J Urol 2010, 183: 1822 – 1829 HIGHLIGHTS • Highest urinary function and bother scores were reported with cryotherapy • Cryoablation post treatment scores exceeded 100% of baseline, presuming reduction in outlet obstruction with subsequent improvement in obstructive and irritative symptoms • Largest prospective, single center study evaluating HRQOL profiles for cryotherapy, ORP, RAP, BT BACKGROUND • Operative treatments for prostate cancer may produce comparable oncological outcomes • Patient reported quality of life outcomes – important measures – vary among options OBJECTIVE • To prospectively compare the health related QOL impact and recovery profiles for four common prostate treatment modalities METHODS • Prospective, longitudinal cohort study of HRQOL outcomes • Evaluated cryoablation, open radical prostatectomy (ORP), robotic assisted laparoscopic radical prostatectomy (RAP) or brachytherapy (BT) • Participants completed a self-administered UCLA-PCI questionnaire - Questionnaires pre treatment and 3, 6, 12, 18, 24, 30 and 36 months post treatment - HRQOL urinary, sexual and bowel function and bother scored using a 100-point scale • Baseline and -

ARRO Case: HDR Prostate Brachytherapy
ARRO Case: HDR Prostate Brachytherapy Karna Sura, MD (PGY-5) Faculty Advisor: Sirisha Nandalur, MD Department of Radiation Oncology Beaumont Health Case Presentation • 67 year old male presented with an elevated PSA at 3.55 ng/mL • Found to have no evidence of abnormalities on DRE • Underwent prostate biopsy May 22, 2018 Case presentation continued • Discussed various treatment options including: – Active surveillance – Radical prostatectomy – External beam radiation – HDR prostate brachytherapy as a monotherapy – Other options include LDR brachytherapy and SBRT • Patient wanted to proceed with brachytherapy May 22, 2018 Brief History of Prostate Brachytherapy • 1917 – Barringer inserted radium needles transperineally in the prostate • 1952 – Flocks et al. injected radioactive gold solution into prostate cancer • 1972 – Willet Whitmore described an open implant technique using 125I • 1983 – H. Holm described technique of implanting the prostate with radioactive seeds May 22, 2018 Radiobiology behind prostate brachytherapy • Prostate tumors have small fraction of cycling cells and possibly a low α/β ratio • A meta-analysis of 20+ studies has estimated the α/β ratio between 1-4 Gy with a mean of 2.7 Gy • Thus, hypofractionation might be more effective for prostate cancer Patient history • Urologic history – Prior transurethral or open resection of the prostate or other surgery on the urethra – Prior procedure for BPH – Medication for urinary obstructive symptoms – Erectile function • Prior diagnosis of cancer, especially rectal or bladder -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Radical Prostatectomy
RADICAL PROSTATECTOMY RADICAL PROSTATECTOMY Location of Surgery: Saint John’s Health Center 2121 Santa Monica Blvd Valet parking available Hospital Phone: 310-829-5511 Patient Name: Date and Time of Surgery: Check-in Arrival Time (2 hours prior to surgery): Physician: Duration of Procedure: Approximate Total Time (arrival to discharge): Office Telephone: 310-582-7137 Office Fax: 310-582-7140 BE SURE TO ARRANGE FOR A FAMILY OR FRIEND TO DRIVE YOU HOME. IT IS RECOMMENDED THAT SOMEONE STAY WITH YOU FOR THE FIRST 24 HOURS AFTER THE PROCEDURE. John Wayne Cancer Institute | Department of Urology and Urologic Oncology | Updated 5/6/20 | Page 1 RADICAL PROSTATECTOMY AFTER SURGERY APPOINTMENTS Radiology Appointment: You will have your cystogram done at this appointment. • Date: • Time: • Location: Saint John’s Health Center 1st Floor 2121 Santa Monica Blvd Santa Monica, CA 90404 1-week Follow-up Appointment: Your urinary catheter will be removed at this visit. Take an antibiotic prior to appointment. • Date: • Time: • Location: Saint John’s Health Center Cancer Clinic (Garden Level) 2121 Santa Monica Blvd John Wayne Cancer Institute | Department of Urology and Urologic Oncology | Updated 5/6/20 | Page 2 RADICAL PROSTATECTOMY GENERAL INFORMATION Prostate cancer is a type of cancer that occurs in the prostate. The prostate is a small walnut-shaped gland, and its function is to create seminal fluid that insulates and transports sperm cells. Prostate cancer is one of the most common cancer in men. About 1 out of 9 men will be diagnosed with prostate cancer during his lifetime. A radical prostatectomy is a surgical treatment for prostate cancer that removes the entire prostate gland. -

Solitary Testicular Metastasis from Prostate Cancer: a Rare Case of Isolated Recurrence After Radical Prostatectomy
ANTICANCER RESEARCH 30: 1747-1750 (2010) Solitary Testicular Metastasis from Prostate Cancer: A Rare Case of Isolated Recurrence after Radical Prostatectomy STEFAN JANSSEN1, JOACHIM BERNHARDS2, ARISTOTELIS G. ANASTASIADIS3 and FRANK BRUNS1 1Department of Radiation Oncology, Hannover Medical School, Hannover, Germany; 2Department of Pathology, Robert Koch Krankenhaus Gehrden, Germany; 3Department of Urology, Großburgwedel Hospital, Germany Abstract. Background: The prognosis of prostate cancer spread of prostate cancer to the testis is commonly accepted (PC) is mainly determined by the presence or absence of as a sign of advanced disease and is often accompanied by metastases. An isolated testicular metastasis of PC is rare. multiple metastases to other organs, especially to the skeletal Case Report: A 71-year-old patient with PC presented with system (4). an increased serum prostate-specific antigen (PSA) level of We report the case of a 71-year-old patient who presented 2.07 ng/ml two and a half years after radical prostatectomy. with a solitary testicular metastasis of prostate cancer two Assuming a local recurrence in the prostatic fossa, local and a half years after prostatectomy. The patient remains free radiotherapy with 64.8 Gy was performed. Unfortunately, the of disease two years after unilateral orchiectomy. PSA level rose again, accompanied by a swelling of the left testis approximately one month after radiotherapy. A Case Report unilateral orchiectomy was then performed, presenting a testicular metastasis of the PC. After orchiectomy, the PSA A 71-year-old Caucasian male consulted his family doctor decreased to <0.07 ng/ml. Two years later, the patient is still complaining of haematospermia. -

Robot-Assisted Prostatectomy Post-Operative Instructions
Robot-Assisted Prostatectomy Post-Operative Instructions FOLLOW-UP APPOINTMENT_______________________________________________________ Following a robot assisted prostatectomy, your attention to proper post-operative follow-up will contribute to the success of your surgery. You are being provided written instructions and information that addresses common questions and concerns. Please review the following prior to surgery. 1. Diet ● Frequent light, soft food. Examples: Oatmeal, smoothies, grits, cream of wheat, eggs, soup, mashed potatoes, fish, and chicken. ● No fried foods, red meat, or spicy foods. Bloating is common after surgery, so limit gas producing foods such as beans, broccoli, cabbage, garlic, etc. ● After your first bowel movement you may slowly advance to a regular diet. 2. Drink ● It is important to drink six to eight 16 ounce bottles of liquid a day. ● DO NOT drink carbonated beverages as they can cause bloating. ● Avoid caffeine, citrus, and alcohol because they irritate the bladder and can cause bladder spasms. ● Please drink plenty of water. 3. Activity ● Within 4 to 6 hours after surgery you will be walking with the assistance of your nurse. Once home, we encourage you to walk at least one mile per day and stretch regularly. Build up slowly to your pre-surgery activity level. ● DO NOT sit in one position for more than 45 minutes. When sitting you may have some discomfort in the perineum (the area you sit on). If this becomes bothersome, you may sit on a donut shaped pillow. ● DO NOT lift, push, or pull anything more than 5lbs. for the first week after surgery and 15lbs for 4 weeks after surgery. -
The Case of Mr. Powers' Prostate Cancer Recurrence
Prostate Cancer 2 - The Case of Mr. Powers’ Prostate Cancer Recurrence Mr. Powers is a young appearing, healthy 73-year old male who underwent a radical prostatectomy nine years ago for prostate cancer. He now has evidence of prostate cancer recurrence. You are expected to direct the evaluation, education, and management of this patient. LEARNING OBJECTIVES 1.Describe the natural history and the common patterns of progression of prostate cancer 2.List the signs & symptoms of metastatic prostate cancer 3.List the options for management of metastatic prostate cancer and describe the mechanisms by which these treatments work Mr. Powers Finally Returns to Clinic Mr. Powers has spent the last several years travelling the world and enjoying himself (“Yea, baby”). He underwent a radical prostatectomy nine years ago for Gleason 6 prostate cancer. While his initial PSA was undetectable his first year, it began to rise slowly after that. He suffered moderate erectile dysfunction after the procedure, but has now recovered fully. Unfortunately, his jet setting lifestyle has filled up his schedule and he was lost to follow-up. Now, Mr. Powers reports no urinary problems and no bone pain. On physical exam, his MoJo is intact and the prostate bed is empty on DRE (as would be expected). His PSA level is checked and comes back 68 ng/ml. Managing Mr. Powers High PSA Mr. Powers cringes upon learning that the traditional therapy for advanced prostate cancer was bilateral orchiectomy. "Not my wedding tackle, Baby," he rants. The rationale for this therapy is that testosterone (and other androgens) actively stimulate the growth of prostate cancer. -

Radical Prostatectomy Innovation and Outcomes at Military and Civilian Institutions
CLINICAL Radical Prostatectomy Innovation and Outcomes at Military and Civilian Institutions Jeffrey J. Leow, MBBS, MPH; Joel S. Weissman, PhD; Linda Kimsey, PhD; Andrew Hoburg, PhD; Lorens A. Helmchen, PhD; Wei Jiang, MS; Nathanael Hevelone, MPH; Stuart R. Lipsitz, ScD; Louis L. Nguyen, MD, MPH, MBA; and Steven L. Chang, MD, MS he rapid pace of clinical innovation—including the development of novel drugs, devices, diagnostic tech- ABSTRACT T niques, and surgical interventions—makes the practice of medicine in the United States dynamic. Hospitals and physicians OBJECTIVES: Limited data are available regarding the impact of the type of healthcare delivery system on constantly seek to offer new technologies that are effective and technology diffusion and associated clinical outcomes. help speed recovery, thereby achieving the best possible results We assessed the adoption of minimally invasive radical for patients. One example of clinical innovation is minimally prostatectomy (MIRP), a recent clinical innovation, and whether this adoption altered surgical morbidity for prostate invasive surgery (MIS), which is associated with fewer complica- cancer surgery. tions across a range of procedures.1 Recently, the introduction of STUDY DESIGN: Retrospective review of administrative robotic surgery has made MIS feasible for even complex surgical data from TRICARE, the healthcare program of the United procedures such as radical prostatectomy (RP) for the manage- States Military Health System. Surgery occurred at military ment of prostate cancer