The Role of Cystoprostatectomy in Management of Locally Advanced
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Original Article Characteristics of Incidental Prostate Cancer After Radical Cystoprostatectomy for Bladder Carcinoma in Chinese Men
Int J Clin Exp Pathol 2016;9(3):3743-3750 www.ijcep.com /ISSN:1936-2625/IJCEP0021275 Original Article Characteristics of incidental prostate cancer after radical cystoprostatectomy for bladder carcinoma in Chinese men Guangxiang Liu1, Shiwei Zhang1, Jun Chen2, Xiaozhi Zhao1, Tieshi Liu1, Shuai Zhu1, Qing Zhang1, Weidong Gan1, Xiaogong Li1, Hongqian Guo1 Departments of 1Urology, 2Pathology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Institute of Urology Nanjing University, Nanjing Medical University, Nanjing, Jiangsu, China Received December 6, 2015; Accepted February 15, 2016; Epub March 1, 2016; Published March 15, 2016 Abstract: The purpose of this study was to analyze and characterize the clinicopathological features of incidental prostate cancer (PCa) after radical cystoprostatectomy (RCP) for bladder cancer in Chinese patients. We retrospec- tively reviewed 378 male patients who underwent RCP for muscle invasive bladder cancer at our center and identi- fied 47 men with incidental PCa. The clinicopathological data of incidental PCa after RCP were compared with those of clinical T1c PCas who had radical prostatectomy at our institute. Forty-seven of the 378 patients (12.4%) were diagnosed with PCa. The incidental PCa was well-differentiated in 68.1% of patients, compared to 33.5% of patients with T1c PCa, and was significantly more unifocal than the T1c PCas. When compared to T1c PCa, the incidental PCa was more likely to be organ-confined, have negative margins and be classified as clinically insignificant. After a mean 48-month follow-up, only one patient with incidental PCa was confirmed to have bone metastasis. While 9 patients with clinical T1c PCa were found to have tumor recurrence or metastasis and 5 patients had died caused by PCa. -

Continent Urostomy Guide
$POUJOFOU6SPTUPNZ(VJEF "QVCMJDBUJPOPGUIF6OJUFE0TUPNZ"TTPDJBUJPOTPG"NFSJDB *OD i4FJ[FUIF 0QQPSUVOJUZw CONTINENT UROSTOMY GUIDE Ilene Fleischer, MSN, RN, CWOCN, Author Patti Wise, BSN, RN, CWOCN, Author Reviewed by: Authors and Victoria A.Weaver, RN, MSN, CETN Revised 2009 by Barbara J. Hocevar, BSN,RN,CWOCN, Manager, ET/WOC Nursing, Cleveland Clinic © 1985 Ilene Fleischer and Patti Wise This guidebook is available for free, in electronic form, from United Ostomy Associations of America (UOAA). UOAA may be contacted at: www.ostomy.org • [email protected] • 800-826-0826 CONTENTS INTRODUCTION . 3 WHAT IS A CONTINENT UROSTOMY? . 4 THE URINARY TRACT . 4 BEFORE THE SURGERY . .5 THE SURGERY . .5 THE STOMA . 7 AFTER THE SURGERY . 7 Irrigation of the catheter(s) 8 Care of the drainage receptacles 9 Care of the stoma 9 Other important information 10 ROUTINE CARE AT HOME . 10 Catheterization schedule 11 How to catheterize your pouch 11 Special considerations when catheterizing 11 Care of the catheter 12 Other routine care 12 HELPFUL HINTS . .13 SUPPLIES FOR YOUR CONTINENT UROSTOMY . 14 LIFE WITH YOUR CONTINENT UROSTOMY . 15 Clothing 15 Diet 15 Activity and exercise 15 Work 16 Travel 16 Telling others 17 Social relationships 17 Sexual relations and intimacy 17 RESOURCES . .19 GLOSSARY OF TERMS . 20 BIBLIOGRAPHY . .21 1 INTRODUCTION Many people have ostomies and lead full and active lives. Ostomy surgery is the main treatment for bypassing or replacing intestinal or urinary organs that have become diseased or dysfunctional. “Ostomy” means opening. It refers to a number of ways that bodily wastes are re-routed from your body. A urostomy specifi cally redirects urine. -

Bilateral Laparoscopic Nephroureterectomy with Open
enDourology Bilateral laparoscopic nephroureterectomy with open cystoprostatectomy for simultaneous upper urinary tract carcinoma tomasz szydełko1, Jarosław Kasprzak1, Wojciech apoznański2, tadeusz niezgoda1, Marcin Kosiński1, anna Kołodziej1, Janusz Dembowski1, romuald Zdrojowy1 1Department of Urology and Urological Oncology, Wrocław University of Medicine, Wrocław, Poland 2Department of Pediatric Surgery and Urology, Wrocław University of Medicine, Wrocław, Poland describe bilateral laparoscopic nephroureterectomy and retroperi- Key WorDs toneal lymphadenectomy combined with cystectomy performed bilateral upper urinary tract carcinoma because of bilateral tumors of the renal pelvices. » laparoscopic nephroureterectomy » cystectomy MaterIal anD MethoDs aBstraCt patient Synchronous bilateral urothelial tumors of the A 74-year-old man with a history of transurethral resection upper urinary tract are extremely rare and their (TUR) and intravesical immunotherapy (BCG maintenance scheme) treatment constitutes a real challenge for urolo- because of bladder tumor, which was determined to be transitional gists. Whereas low grade superficial tumors can be cell carcinoma (TCC), pT1 grade 3 presented with gross hematuria treated using endoscopic procedures, in the case of in May 2008. Intravesical immunotherapy had been completed in high grade, invasive or large volume tumors bilat- 2003 and since then the patient had not turned up for follow-up. eral radical nephroureterectomy with cystectomy is Cystoscopy with mapping biopsy performed at presentation did not considered the standard of care. The authors present reveal any tumor in the bladder. The diagnostic evaluation, i.e. ul- the case of large volume high grade tumors of the trasound and CT revealed large volume bilateral renal pelvis tumors renal pelvices in a patient with a history of super- (Fig. 1). -

Paulos Yohannes, MD Board Certified Urologist and Diplomate of the American Board of Urology
Paulos Yohannes, MD Board Certified Urologist and Diplomate of the American Board of Urology Paulos Yohannes, Dr. Yohannes is one of the pioneers M.D. received of robotic urologic surgery in the his medical United States. He performed the first degree from the robotic cystoprostatectomy for bladder University of cancer (2003), robotic intracorporeal Louisville, School ileal conduit urinary diversion (2004), of Medicine and robotic repair of retrocaval and then ureter (2004) in the United States. completed his general surgery He is a reviewer for numerous peer- and urology reviewed journals, book chapters, and residency training has proctored many surgeons around at the University of Kentucky, Albert B. the country on their first prostatectomy Chandler medical center and University and cystoprostatectomy surgical cases. of Louisville Hospital. He completed a fellowship in Endourology/Laparoscopy He has won numerous awards including from Long Island Jewish Medical Center academic essay competitions, the where he specialized in minimally William Brohm Award, Pfizer scholar in invasive endourologic and laparoscopic urology award, and Kentucky Urologic surgery for the management of stone Society Pyelogram Award. In addition, disease; testicular, bladder, kidney, he has received recognition by Vitals and prostate cancer; percutaneous for: The Compassionate Doctor management of urothelial cancer, Award, Castle Connolly Regional as well as reconstructive surgery of Top Doctor Award, On Time Doctor the upper and lower urinary tract. Award, Patients’ Choice Award, and Top Ten Doctors - State award. 11181 Health Park Blvd., Suite 1115, Naples, FL 34110 8340 Collier Blvd., Suite 207, Naples, FL 34114 1839 San Marco Road, Marco Island, FL 34145 Phone: (239) 597-4440 • Fax: (239) 597-4441 Website: www.encoreurology.com • Email: [email protected]. -

Quality of Life Outcomes After Brachytherapy for Early Prostate Cancer
Prostate Cancer and Prostatic Diseases (1999) 2 Suppl 3, S19±S20 ß 1999 Stockton Press All rights reserved 1365±7852/99 $15.00 http://www.stockton-press.co.uk/pcan Quality of life outcomes after brachytherapy for early prostate cancer MS Litwin1, JM Brandeis1, CM Burnison1 and E Reiter1 1UCLA Departments of Urology, Health Services, and Radiation Oncology, UCLA, California, USA Despite the absence of empirical evidence, there is a XRT. Sildena®l appeared to have little effect in the radical popular perception that brachytherapy results in less prostatectomy patients. However, brachytherapy patients impairment of health-related quality of life. This study not receiving hormonal ablation or XRT who took silde- compared general and disease-speci®c health-related na®l had better sexual function and bother scores than quality of life in men who had undergone either brachy- those patients who did not. therapy (with and without pre-treatment XRT) or radical prostatectomy, and in healthy age-matched controls. Method Conclusion We surveyed all patients with clinical T2 or less prostate General health-related quality of life did not differ greatly cancer who had undergone interstitial seed brachyther- between the three groups, but there were variations in apy at UCLA during the previous 3±17 months. Each was disease-speci®c (urinary, bowel and sexual) health-related paired with two randomly selected, temporally matched quality of life. Radical prostatectomy patients had the radical prostatectomy patients. Healthy, age-matched worst urinary function (leakage), but brachytherapy controls were drawn from the literature. Surgery and patients were also signi®cantly worse than the controls. -

Prostate Biopsy in the Staging of Prostate Cancer
Prostate Cancer and Prostatic Diseases (1997) 1, 54±58 ß 1997 Stockton Press All rights reserved 1365±7852/97 $12.00 Review Prostate Biopsy in the staging of prostate cancer L Salomon, M Colombel, J-J Patard, D Gasman, D Chopin & C-C Abbou Service d'Urologie, CHU, Henri Mondor, CreÂteil, France The use of prostate biopsies was developed in parallel with progress in our knowledge of prostate cancer and the use of prostate-speci®c antigen (PSA). Prostate biopsies were initially indicated for the diagnosis of cancer, by the perineal approach under general anesthesia. Nowadays prostate biopsies are not only for diagnostic purposes but also to determine the prognosis, particularly before radical prostatectomy. They are performed in patients with elevated PSA levels, by the endorectal approach, sometimes under local anesthesia.(1±3) The gold standard is the sextant biopsy technique described by Hodge4,5, which is best to diagnose prostate cancer, particularly in case of T1c disease (patients with serum PSA elevation).6±13 Patients with a strong suspicion of prostate cancer from a negative series of biopsies can undergo a second series14;15 with transition zone biopsy16,17 or lateral biopsy.18,19 Karakiewicz et al 20 and Uzzo et al 21 proposed that the number of prostate biopsies should depend on prostate volume to improve the positivity rate. After the diagnosis of prostate cancer, initial therapy will depend on several prognostic factors. In the case of radical prostatectomy, the results of sextant biopsy provide a wealth of information.22,23 The aim of this report is to present the information given by prostate biopsy in the staging of prostate cancer. -

Needle Biopsy and Radical Prostatectomy Specimens David J Grignon
Modern Pathology (2018) 31, S96–S109 S96 © 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 Prostate cancer reporting and staging: needle biopsy and radical prostatectomy specimens David J Grignon Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, IUH Pathology Laboratory, Indianapolis, IN, USA Prostatic adenocarcinoma remains the most common cancer affecting men. A substantial majority of patients have the diagnosis made on thin needle biopsies, most often in the absence of a palpable abnormality. Treatment choices ranging from surveillance to radical prostatectomy or radiation therapy are largely driven by the pathologic findings in the biopsy specimen. The first part of this review focuses on important morphologic parameters in needle biopsy specimens that are not covered in the accompanying articles. This includes tumor quantification as well as other parameters such a extraprostatic extension, seminal vesicle invasion, perineural invasion, and lymphovascular invasion. For those men who undergo radical prostatectomy, pathologic stage and other parameters are critical in prognostication and in determining the appropriateness of adjuvant therapy. Staging parameters, including extraprostatic extension, seminal vesicle invasion, and lymph node status are discussed here. Surgical margin status is also an important parameter and definitions and reporting of this feature are detailed. Throughout the article the current reporting guidelines published by the College of American Pathologists and the International Collaboration on Cancer Reporting are highlighted. Modern Pathology (2018) 31, S96–S109; doi:10.1038/modpathol.2017.167 The morphologic aspects of prostatic adenocarcinoma hormonal therapy.4,5 For needle biopsy specimens the have a critical role in the management and prognos- data described below are largely based on standard tication of patients with prostatic adenocarcinoma. -

Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis
www.kjurology.org DOI:10.4111/kju.2010.51.1.70 Case Report Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis Kyung Hwa Choi, Seung Hwan Lee, Won Sug Jung1, Byung Ha Chung Department of Urology, Urological Science Institute, Yonsei University College of Medicine, Seoul, 1National Health Insurance Corporation Ilsan Hospital, Goyang, Korea We report a rare case of robot-assisted laparoscopic radical prostatectomy (RARP) in Article History: a patient with a preexisting penile prosthesis. In this case, we completed RARP without received 27 August, 2009 14 October, 2009 removing the reservoir by using a deflation-inflation technique, and there were no com- accepted plications related to the prosthesis. The patient had a negative surgical margin. The Corresponding Author: preserved three-piece inflatable penile prosthesis continued to function properly in 1 Byung Ha Chung month. Reservoir-preserving RARP is technically feasible and safe. However, it is im- Department of Urology, Yonsei portant to be aware of device-related complications. Long-term studies on the mechan- University Health System, Gangnam Severance Hospital, 712, Eonju-ro, ical survival rate and patient satisfaction should be also performed. Dogok-dong, Gangnam-gu, Seoul Key Words: Robotics, Prostatectomy, Penile prosthesis, Prostatic neoplasms 135-720, Korea TEL: +82-2-2019-3474 FAX: +82-2-3462-8887 E-mail: [email protected] Prostate cancer has been reported to occur most frequently CASE REPORT in men over 40 years of age. In organ-confined cases, radical prostatectomy is the treatment of choice. After the in- 1. Patient troduction of the da VinciⓇ surgical system (Intuitive The patient was a 64-year-old male diagnosed with aci- Surgical, Sunnyvale, USA), robot-assisted laparoscopic nar-type prostate adenocarcinoma with a Gleason score of radical prostatectomy (RARP) has become a mainstay of 6 (3+3) by prostate biopsy. -
Spring 2020 Newsletter
DEPARTMENT OF UROLOGYNEWS Volume 4 | SPRING 2020 CHAIR Benjamin R Lee, MD (interim) FACULTY Juan Chipollini, MD Joel Funk, MD Matthew Gretzer, MD David Tzou, MD Roger Nellans, MD Christian Twiss, MD Deb Jur, FNP Rosa Garcia, FNP Alison Grabowski, FNP Carmen Panizo, FNP Cara Whittingham, FNP RESEARCH Ken Batai, PhD Ava Wong, Coordinator AFFILIATED FACULTY Michael Siroky, MD Maximiliano Sorbellini, MD Mark Cogburn, MD Alex Jule, MD Rajesh Prasad, MD Jonathan Walker, MD Philip Gleason, MD Barry Chang, MD Hiep Nguyen, MD , Ariella Friedman, MD ADAPTABILITY Tamis Thrasher, PNP SOCIAL DISTANCING AND Department of Urology is published annually yearly by the University of Arizona College of Medicine Department of Urology. CRISIS MANAGEMENT CONTACT: Dr. Benjamin R. Lee, MD Chair (Interim) & Professor [email protected] Department of Urology The George W. Drach, MD Endowed Chair Department of Urology College of Medicine, Room 5325 The University of Arizona 1501 N. Campbell Ave. P.O. Box 245077 Tucson, AZ 85724-5077 520-694-4032 Fax: 520-694-5509 urology.arizona.edu All contents © 2020 Arizona Board of Regents. All rights reserved. The UA is an EEO/AA – M/W/D/V Employer. Design: UAHS BioCommunications To read this and past issues of Department of Urology Newsletter online, visit urology.arizona.edu/news-0 Deb Jur, NP Our Newest Nurse Practitioner Banner – University Medical Center Tucson welcomes Deb Jur, FNP to the Urology clinic at 3838 N Campbell Ave. Deb has been enthusiastically providing nursing care for her entire career, and has been an NP Dr. George W. Drach, Dr. Benjamin R Lee, Dean Michael Abecassis at the Investiture Ceremony specializing in urology for for the 1st Endowed Chair of Urology over 10 years. -
Quality of Life After Open Or Robotic Prostatectomy, Cryoablation Or
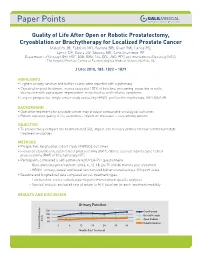
Quality of Life After Open or Robotic Prostatectomy, Cryoablation or Brachytherapy for Localized Prostate Cancer Malcolm JB, Fabrizio MD, Barone BB, Given RW, Lance RS, Lynch DF, Davis JW, Shaves ME, Schellhammer PF Departments of Urology (JBM, MDF, BBB, RWG, RSL, DFL, JWD, PFS) and Interventional Radiology (MES), The Virginia Prostate Center at Eastern Virginia Medical School, Norfolk, VA J Urol 2010, 183: 1822 – 1829 HIGHLIGHTS • Highest urinary function and bother scores were reported with cryotherapy • Cryoablation post treatment scores exceeded 100% of baseline, presuming reduction in outlet obstruction with subsequent improvement in obstructive and irritative symptoms • Largest prospective, single center study evaluating HRQOL profiles for cryotherapy, ORP, RAP, BT BACKGROUND • Operative treatments for prostate cancer may produce comparable oncological outcomes • Patient reported quality of life outcomes – important measures – vary among options OBJECTIVE • To prospectively compare the health related QOL impact and recovery profiles for four common prostate treatment modalities METHODS • Prospective, longitudinal cohort study of HRQOL outcomes • Evaluated cryoablation, open radical prostatectomy (ORP), robotic assisted laparoscopic radical prostatectomy (RAP) or brachytherapy (BT) • Participants completed a self-administered UCLA-PCI questionnaire - Questionnaires pre treatment and 3, 6, 12, 18, 24, 30 and 36 months post treatment - HRQOL urinary, sexual and bowel function and bother scored using a 100-point scale • Baseline and -

ARRO Case: HDR Prostate Brachytherapy
ARRO Case: HDR Prostate Brachytherapy Karna Sura, MD (PGY-5) Faculty Advisor: Sirisha Nandalur, MD Department of Radiation Oncology Beaumont Health Case Presentation • 67 year old male presented with an elevated PSA at 3.55 ng/mL • Found to have no evidence of abnormalities on DRE • Underwent prostate biopsy May 22, 2018 Case presentation continued • Discussed various treatment options including: – Active surveillance – Radical prostatectomy – External beam radiation – HDR prostate brachytherapy as a monotherapy – Other options include LDR brachytherapy and SBRT • Patient wanted to proceed with brachytherapy May 22, 2018 Brief History of Prostate Brachytherapy • 1917 – Barringer inserted radium needles transperineally in the prostate • 1952 – Flocks et al. injected radioactive gold solution into prostate cancer • 1972 – Willet Whitmore described an open implant technique using 125I • 1983 – H. Holm described technique of implanting the prostate with radioactive seeds May 22, 2018 Radiobiology behind prostate brachytherapy • Prostate tumors have small fraction of cycling cells and possibly a low α/β ratio • A meta-analysis of 20+ studies has estimated the α/β ratio between 1-4 Gy with a mean of 2.7 Gy • Thus, hypofractionation might be more effective for prostate cancer Patient history • Urologic history – Prior transurethral or open resection of the prostate or other surgery on the urethra – Prior procedure for BPH – Medication for urinary obstructive symptoms – Erectile function • Prior diagnosis of cancer, especially rectal or bladder -

Robotic-Assisted Laparoscopic Radical Prostatectomy After Aborted Retropubic Radical Prostatectomy
J Robotic Surg (2013) 7:301–304 DOI 10.1007/s11701-012-0377-9 CASE REPORT Robotic-assisted laparoscopic radical prostatectomy after aborted retropubic radical prostatectomy Keith J. Kowalczyk • Andy C. Huang • Stephen B. Williams • Hua-yin Yu • Jim C. Hu Received: 11 March 2012 / Accepted: 31 July 2012 / Published online: 19 August 2012 Ó Springer-Verlag London Ltd 2012 Abstract Robotic-assisted laparoscopic prostatectomy of the endopelvic fascia due to poor visualization, a (RALP) has surged in popularity since US Food and Drug prominent pubic tubercle, and a narrow pelvis. The Administration approval in 2000. Advantages include enhanced visualization and precision of the robotic plat- improved visualization and increased instrument dexterity form allowed adequate exposure of the prostate and within the pelvis. Obesity and narrow pelves have been allowed us to proceed with an uncomplicated prostatecto- associated with increased difficulty during open retropubic my, which was not possible to perform easily via an open radical prostatectomy (RRP), but the robotic platform approach. The bladder was densely adherent to the pubis theoretically allows one to perform a radical prostatectomy and the anterior prostatic contour and apex were difficult to despite these challenges. We present an example of a develop due to a dense fibrotic reaction from the previous RALP performed following an aborted RRP. A 49-year-old endopelvic fascia incision. However, we were able to male with intermediate risk prostate cancer and body mass successfully complete RALP with subtle technical modi- index of 38 kg/m2 presented for RALP after RRP was fications. Estimated blood loss was 160 mL and operating aborted by an experienced open surgeon following incision time was 145 min.