Continent Urostomy Guide
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Original Article Characteristics of Incidental Prostate Cancer After Radical Cystoprostatectomy for Bladder Carcinoma in Chinese Men
Int J Clin Exp Pathol 2016;9(3):3743-3750 www.ijcep.com /ISSN:1936-2625/IJCEP0021275 Original Article Characteristics of incidental prostate cancer after radical cystoprostatectomy for bladder carcinoma in Chinese men Guangxiang Liu1, Shiwei Zhang1, Jun Chen2, Xiaozhi Zhao1, Tieshi Liu1, Shuai Zhu1, Qing Zhang1, Weidong Gan1, Xiaogong Li1, Hongqian Guo1 Departments of 1Urology, 2Pathology, Nanjing Drum Tower Hospital, The Affiliated Hospital of Nanjing University Medical School, Institute of Urology Nanjing University, Nanjing Medical University, Nanjing, Jiangsu, China Received December 6, 2015; Accepted February 15, 2016; Epub March 1, 2016; Published March 15, 2016 Abstract: The purpose of this study was to analyze and characterize the clinicopathological features of incidental prostate cancer (PCa) after radical cystoprostatectomy (RCP) for bladder cancer in Chinese patients. We retrospec- tively reviewed 378 male patients who underwent RCP for muscle invasive bladder cancer at our center and identi- fied 47 men with incidental PCa. The clinicopathological data of incidental PCa after RCP were compared with those of clinical T1c PCas who had radical prostatectomy at our institute. Forty-seven of the 378 patients (12.4%) were diagnosed with PCa. The incidental PCa was well-differentiated in 68.1% of patients, compared to 33.5% of patients with T1c PCa, and was significantly more unifocal than the T1c PCas. When compared to T1c PCa, the incidental PCa was more likely to be organ-confined, have negative margins and be classified as clinically insignificant. After a mean 48-month follow-up, only one patient with incidental PCa was confirmed to have bone metastasis. While 9 patients with clinical T1c PCa were found to have tumor recurrence or metastasis and 5 patients had died caused by PCa. -

A Practical Guide for Stoma Problems Developed by the Ostomy Forum
A practical guide for Stoma problems Developed by the Ostomy Forum Dedicated to Stoma Care A practical guide for Stoma and Peristomal skin problems A practical guide for Stoma Developed by: Frances McKenzie, Amanda Smith, Doreen Woolley, Beverley Colton, Bart Tappe and Global Clinical Marketing, Dansac A/S. The practical guide is based on the Observation Index developed by the Ostomy Forum group (a specialized group of ET nurses from Sweden, Norway, The Netherlands, Poland, Japan, UK and Denmark) and is Normal Stoma made to help you manage common stoma and peristomal skin problems you might come across in your nursing practice. Stoma is a Greek word that means opening or mouth. It is a surgically created opening that can be temporary or permanent and allows for the Sharing best practice by use of this educational tool will lead to early excretion of faecal waste (colostomy, ileostomy) or urine (urostomy). detection and appropriate intervention to secure a high standard of stoma care. A stoma is a surgically made opening of the bowel: • The bowel is brought out through the abdominal wall This tool should be used in consultation with your Stoma Care Specialist. • It is matured and sutured subcutaneously • Faeces and urine will pass and be collected in a specially designed Disclaimer: ostomy pouch. We recognize that nurses in other practices will have different ways of treating the identified problems. The scope of this guide is to give first In the following pages you will find examples of different stoma problems step, easy to use, practical advice that is recognized and accepted and concrete suggestions for intervention and management of the stoma. -

Adjustable Gastric Banding
7 Review Article Page 1 of 7 Adjustable gastric banding Emre Gundogdu, Munevver Moran Department of Surgery, Medical School, Istinye University, Istanbul, Turkey Contributions: (I) Conception and design: All authors; (II) Administrative support: All authors; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Emre Gündoğdu, MD, FEBS. Assistant Professor of Surgery, Department of Surgery, Medical School, Istinye University, Istanbul, Turkey. Email: [email protected]; [email protected]. Abstract: Gastric banding is based on the principle of forming a small volume pouch near the stomach by wrapping the fundus with various synthetic grafts. The main purpose is to limit oral intake. Due to the fact that it is a reversible surgery, ease of application and early results, the adjustable gastric band (AGB) operation has become common practice for the last 20 years. Many studies have shown that the effectiveness of LAGB has comparable results with other procedures in providing weight loss. Early studies have shown that short term complications after LAGB are particularly low when compared to the other complicated procedures. Even compared to RYGB and LSG, short-term results of LAGB have been shown to be significantly superior. However, as long-term results began to emerge, such as failure in weight loss, increased weight regain and long-term complication rates, interest in the procedure disappeared. The rate of revisional operations after LAGB is rapidly increasing today and many surgeons prefer to convert it to another bariatric procedure, such as RYGB or LSG, for revision surgery in patients with band removed after LAGB. -

Suprapubic Cystostomy: Urinary Tract Infection and Other Short Term Complications A.T
Suprapubic Cystostomy: Urinary Tract Infection and other short term Complications A.T. Hasan,Q. Fasihuddin,M.A. Sheikh ( Department of Urological Surgery and Transplantation, Jinnah Postgraduate Medical Center, Karachi. ) Abstract Aims: To evaluate the frequency of urinary tract infection in patients with suprapubic cystostomy and other complications of the procedure within 30 days of placement. Methods: Patients characteristics, indication and types of cystostomy and short term (within 30 days); complications were analyzed in 91 patients. Urine analysis and culture was done in all patients to exclude those with urinary tract infection. After 15 and 30 days of the procedure, urine analysis and culture was repeated to evaluate the frequency of urinary tract infection. The prevalence of symptomatic bacteriuria with its organisms was assessed. Antibiotics were given to the postoperative and symptomatic patients and the relationship of antibiotics on the prevention of urinary tract infection was determined. Results: Of the 91 cases 88 were males and 3 females. The mean age was 40.52 ± 18.95 with a range of 15 to 82 years.Obstructive uropathy of lower urinary tract.was present in 81% cases and 17(18.6%) had history of trauma to urethra. All these cases had per-urethral bleeding on examination while x-ray urethrogram showed grade H or grade III injury of urethra. Eighty two of the procedures were performed per-cutaneously and 7 were converted to open cystostomies due to failure of per-cutaneous approach. Nine patients had exploratory laparotomy. Duration of catheterization was the leading risk factor for urinary tract infection found in 24.1% at 15 days and 97.8% at 30 days. -
Cystectomy (Bladder Removal) with Ileal Conduit Urinary Diversion
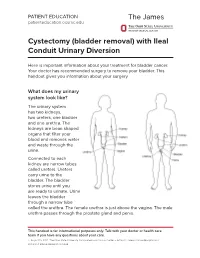
PATIENT EDUCATION patienteducation.osumc.edu Cystectomy (bladder removal) with Ileal Conduit Urinary Diversion Here is important information about your treatment for bladder cancer. Your doctor has recommended surgery to remove your bladder. This handout gives you information about your surgery. What does my urinary system look like? The urinary system has two kidneys, two ureters, one bladder and one urethra. The kidneys are bean shaped organs that filter your blood and removes water and waste through the urine. Connected to each kidney are narrow tubes called ureters. Ureters carry urine to the bladder. The bladder stores urine until you are ready to urinate. Urine leaves the bladder through a narrow tube called the urethra. The female urethra is just above the vagina. The male urethra passes through the prostate gland and penis. This handout is for informational purposes only. Talk with your doctor or health care team if you have any questions about your care. © August 19, 2021. The Ohio State University Comprehensive Cancer Center – Arthur G. James Cancer Hospital and Richard J. Solove Research Institute. Cystectomy (bladder removal) with Ileal Conduit Urinary Diversion A cystectomy is surgery to remove the bladder. In men, the prostate, seminal vesicles and lymph nodes may also be removed. In women, the ovaries, fallopian tubes, uterus, cervix, vagina, urethra and lymph nodes may be removed. Your doctor will talk with you about the surgery and what is best for you. After the bladder is removed, your doctor will make a new urinary system. One option is an ileal conduit, also called a urostomy. This will direct your urine to drain through a small opening in your abdomen (belly) called a “stoma”. -

Bilateral Laparoscopic Nephroureterectomy with Open
enDourology Bilateral laparoscopic nephroureterectomy with open cystoprostatectomy for simultaneous upper urinary tract carcinoma tomasz szydełko1, Jarosław Kasprzak1, Wojciech apoznański2, tadeusz niezgoda1, Marcin Kosiński1, anna Kołodziej1, Janusz Dembowski1, romuald Zdrojowy1 1Department of Urology and Urological Oncology, Wrocław University of Medicine, Wrocław, Poland 2Department of Pediatric Surgery and Urology, Wrocław University of Medicine, Wrocław, Poland describe bilateral laparoscopic nephroureterectomy and retroperi- Key WorDs toneal lymphadenectomy combined with cystectomy performed bilateral upper urinary tract carcinoma because of bilateral tumors of the renal pelvices. » laparoscopic nephroureterectomy » cystectomy MaterIal anD MethoDs aBstraCt patient Synchronous bilateral urothelial tumors of the A 74-year-old man with a history of transurethral resection upper urinary tract are extremely rare and their (TUR) and intravesical immunotherapy (BCG maintenance scheme) treatment constitutes a real challenge for urolo- because of bladder tumor, which was determined to be transitional gists. Whereas low grade superficial tumors can be cell carcinoma (TCC), pT1 grade 3 presented with gross hematuria treated using endoscopic procedures, in the case of in May 2008. Intravesical immunotherapy had been completed in high grade, invasive or large volume tumors bilat- 2003 and since then the patient had not turned up for follow-up. eral radical nephroureterectomy with cystectomy is Cystoscopy with mapping biopsy performed at presentation did not considered the standard of care. The authors present reveal any tumor in the bladder. The diagnostic evaluation, i.e. ul- the case of large volume high grade tumors of the trasound and CT revealed large volume bilateral renal pelvis tumors renal pelvices in a patient with a history of super- (Fig. 1). -

Complications of Urinary Diversion
Complications of Urinary Diversion Jennifer L. Dodson, M.D. Department of Urology Johns Hopkins University Types of Diversion Conduit Diversions Ileal conduit Colon conduit Continent Diversions Continent catheterizable reservoir Continent rectal pouch 1 Overview of Complications Mechanical Stoma problems Bowel obstruction Ureteral obstruction Reservoir perforation Metabolic Altered absorption Altered bone metabolism Growth delay Stones Cancer Conduit Diversions Ileal Conduit: Technically simplest Segment of choice Colon Conduit: Transverse or sigmoid Used when ileum not appropriate (eg: concomitant colon resection, abdominal radiation, short bowel syndrome, IBD) Early complications (< 30 days): 20-56% Late complications : 28-81% Risks: abdominal radiation abdominal surgery poor nutrition chronic steroids Farnham & Cookson, World J Urol, 2004 2 Complications of Ileal Conduit Campbell’s Urology, 8th Edition, 2002 Conduit: Bowel Complications Paralytic ileus 18-20% Conservative management vs NGT Consider TPN Bowel obstruction 5-10% Causes: Adhesions, internal hernia Evaluation: CT scan, Upper GI series Anastomotic leak 1-5 % Risk factors: bowel ischemia, radiation, steroids, IBD, technical error Prevention: Pre-operative bowel prep Attention to technical detail Stapled small-bowel Anastomosis (Campbell’s Blood supply, tension-free anastomosis, Urology, 8th Ed, 2004) realignment of mesentery Farnham & Cookson, World J Urol, 2004 3 Conduit Complications Conduit necrosis: Acute ischemia to bowel -

Paulos Yohannes, MD Board Certified Urologist and Diplomate of the American Board of Urology
Paulos Yohannes, MD Board Certified Urologist and Diplomate of the American Board of Urology Paulos Yohannes, Dr. Yohannes is one of the pioneers M.D. received of robotic urologic surgery in the his medical United States. He performed the first degree from the robotic cystoprostatectomy for bladder University of cancer (2003), robotic intracorporeal Louisville, School ileal conduit urinary diversion (2004), of Medicine and robotic repair of retrocaval and then ureter (2004) in the United States. completed his general surgery He is a reviewer for numerous peer- and urology reviewed journals, book chapters, and residency training has proctored many surgeons around at the University of Kentucky, Albert B. the country on their first prostatectomy Chandler medical center and University and cystoprostatectomy surgical cases. of Louisville Hospital. He completed a fellowship in Endourology/Laparoscopy He has won numerous awards including from Long Island Jewish Medical Center academic essay competitions, the where he specialized in minimally William Brohm Award, Pfizer scholar in invasive endourologic and laparoscopic urology award, and Kentucky Urologic surgery for the management of stone Society Pyelogram Award. In addition, disease; testicular, bladder, kidney, he has received recognition by Vitals and prostate cancer; percutaneous for: The Compassionate Doctor management of urothelial cancer, Award, Castle Connolly Regional as well as reconstructive surgery of Top Doctor Award, On Time Doctor the upper and lower urinary tract. Award, Patients’ Choice Award, and Top Ten Doctors - State award. 11181 Health Park Blvd., Suite 1115, Naples, FL 34110 8340 Collier Blvd., Suite 207, Naples, FL 34114 1839 San Marco Road, Marco Island, FL 34145 Phone: (239) 597-4440 • Fax: (239) 597-4441 Website: www.encoreurology.com • Email: [email protected]. -
Hints and Tips
Hernia Simon, colostomy since 2010 Hints & Tips Dedicated to Stoma Care Dedicated to Stoma Care FOREWORD & ACKNOWLEDGEMENTS This booklet offers guidance to the person undergoing surgery which will result in stoma formation or for those post-operatively who may be at risk of or perhaps already have developed a parastomal hernia. Please discuss the content with your Stomal Therapy Nurse (STN) if you require additional advice or support. CONTENT What is a parastomal hernia? .........................................3 Am I at risk of developing a parastomal hernia? ������������4 What is my ideal weight? ................................................5 Practical hints & tips to reduce risk of developing a parastomal hernia .....................................6 I think I’ve developed a hernia - what should I do? ���������7 Parastomal hernia management �������������������������������������8 Exercise ..........................................................................9 Dansac would like to thank the following for their invaluable contribution to this booklet: Sharon Colman BSc (Hons) Community Stoma Nurse Specialist, Norfolk. Kevin Hayles Dip HE, RN Queens Hospital Romford, Essex. Debbie Johnson RGN, Stoma Specialist, Dansac UK, London Community. Jacqui North RGN BSc(Hons), Senior Clinical Nurse Specialist, Stoma Care, SE London Community. Jo Sica Clinical Nurse Specialist, Stoma Care, Kingston CCG. 2 WHAT IS A PARASTOMAL HERNIA? Parastomal hernia is a common complication which can affect some people following stoma formation. Research has shown that as many as 10-50% of patients may go on to develop a hernia.6, 9, 10 During your surgery an incision is made through the abdominal wall and muscle. This can result in a weakness in the muscle surrounding your stoma which may lead to a noticeable bulge behind or around the stoma. -
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop
Urinary Diversion: Ileovesicostomy/Ileal Loop/Colon Loop Why do I need this surgery? A urinary diversion is a surgical procedure that is performed to allow urine to safely pass from the kidneys into a pouch on a person’s abdomen (belly). It is performed for people who have otherwise untreatable urinary incontinence (leakage) chronic urinary infections, or dangerous bladder conditions that may damage kidney function. The goal of these procedures is to improve a person’s long term health and quality of life. What is a stoma? A stoma is the end of the urinary diversion that protrudes through your abdominal wall. The stoma is red, moist, soft, and has no nerve endings. A pouch is placed around the stoma to collect the urine. You will meet with an enterostomal therapy nurse prior to surgery to find the optimal location for the stoma on your abdomen, provide education regarding stoma and skin management, and show you samples of the ostomy pouches that may be used over your stoma after surgery. What is done during the surgery? A urinary diversion surgery is performed in the operating room under general anesthesia (you are not awake for the procedure). The procedure can take 3 to 5 hours, depending on the complexity. Types of urinary diversions: 1. Ileovesicostomy. Department of Urology 734-936-7030 - 1 - In this procedure, the surgeon isolates a 15cm segment of intestine (ileum) from the GI tract. The bowels are then reconnected so that you will still have regular bowel movements, if you had regular movements before. A small hole is made in the bladder and the isolated segment is then sewn to the bladder. -

EAU Guidelines on Bladder Stones 2019
EAU Guidelines on Bladder Stones C. Türk (Chair), A. Skolarikos (Vice-chair), J.F. Donaldson, A. Neisius, A. Petrik, C. Seitz, K. Thomas Guidelines Associate: Y. Ruhayel © European Association of Urology 2019 TABLE OF CONTENTS PAGE 1. INTRODUCTION 3 1.1 Aims and Scope 3 1.2 Panel Composition 3 1.3 Available Publications 3 1.4 Publication History and Summary of Changes 3 1.4.1 Publication History 3 2. METHODS 3 2.1 Data Identification 3 2.2 Review 4 3. GUIDELINES 4 3.1 Prevalence, aetiology and risk factors 4 3.2 Diagnostic evaluation 4 3.2.1 Diagnostic investigations 5 3.3 Disease Management 5 3.3.1 Conservative treatment and Indications for active stone removal 5 3.3.2 Medical management of bladder stones 5 3.3.3 Bladder stone interventions 5 3.3.3.1 Suprapubic cystolithotomy 5 3.3.3.2 Transurethral cystolithotripsy 5 3.3.3.2.1 Transurethral cystolithotripsy in adults: 5 3.3.3.2.2 Transurethral cystolithotripsy in children: 6 3.3.3.3 Percutaneous cystolithotripsy 6 3.3.3.3.1 Percutaneous cystolithotripsy in adults: 6 3.3.3.3.2 Percutaneous cystolithotripsy in children: 6 3.3.3.4 Extracorporeal shock wave lithotripsy (SWL) 6 3.3.3.4.1 SWL in Adults 6 3.3.3.4.2 SWL in Children 6 3.3.4 Treatment for bladder stones secondary to bladder outlet obstruction (BOO) in adult men 7 3.3.5 Urinary tract reconstructions and special situations 7 3.3.5.1 Neurogenic bladder 7 3.3.5.2 Bladder augmentation 7 3.3.5.3 Urinary diversions 7 4. -
Urinary Sample Collection Methods in Ileal Conduit Urinary Diversion Patients a Randomized Control Trial Markku H
Ostomy Care Ostomy Care J Wound Ostomy Continence Nurs. 2018;45(1):59-62. Published by Lippincott Williams & Wilkins Urinary Sample Collection Methods in Ileal Conduit Urinary Diversion Patients A Randomized Control Trial Markku H. Vaarala ABSTRACT PURPOSE: The purpose of this study was to compare bacteriological urinalysis findings using 3 urinary sample collection methods (clean stoma catheterization, urine dripping from the stoma, urine collected from the clean urostomy pouch) in ileal conduit urinary diversion patients. DESIGN: Randomized controlled trial. SAMPLE AND SETTING: Twenty-seven patients with ileal conduit urinary diversion from an outpatient urology clinic were enrolled; 9 patients were seen twice, for a total of 36 subjects and comparisons. METHODS: Data were collected during a clinic visit by a trained research nurse. Patients were randomized into 2 groups: group A had the first urine sample collected by clean stoma catheterization, followed by sample collection by urine dripping from the stoma; group B had the first urine sample collection by urine dripping from the stoma, followed by sample collected by clean stoma catheterization. All patients had a third urine sample collected from a factory-clean urostomy pouch. Bacteriological urinalysis findings were compared among methods. Descriptive analyses were summarized using mean, percentage, and frequency. The mean ages of the patients between the groups were compared with the t test. Other between-group comparisons were performed using the Fisher exact test. Urinary culture finding differences among the same patients were evaluated using the McNemar test. Sensitivity and specificity of the different urine sample collection methods were calculated assuming urine sample collection by catheterization as a reference method.