Robot-Assisted Radical Prostatectomy in a Patient with a Preexisting Three-Piece Inflatable Penile Prosthesis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Jared J. Wallen MD MBA
Jared J. Wallen MD MBA Education Post American Board of Urology – Board Certification (Expires 02/28/2029) Massachusetts Institute of Technology – Certificate Commercial Real Estate Analysis and Investing (Class of 2019) London School of Economics and Political Science – Certificate Masters of Business Administration Essentials (Class of 2019) Masters in Real Estate Fortune Builders (Class of 2020) Florida Real Estate Sales Associate License Certification (09/2020) Designation as National Commercial Real Estate Advisor and Certified Real Estate Investment Planning Specialist (01/2021) Fell. Boston Scientific Men’s Sexual Health Research Fellow, Class of 2018 P.G. University of Southern Florida – Morsani College of Medicine, Urologic Surgery Residency, Class of 2017 University of Southern Florida – Morsani College of Medicine, General Surgery Internship, Class of 2013 M.D. Rush Medical College, Doctorate in Medicine, Class of 2012 B.S. University of Illinois Urbana/Champaign, Bachelors with Honors in Molecular and Cellular Biology and Psychology, Class of 2008 A.A. Rock Valley Community College, Associates in Arts, Concentration in Psychology, Class of 2004 Experience • Manager and Lead Urologic Surgeon – YOU & WEE Urologic 10/2020 – present Surgery and Wellness • Manager – RUFF & RESTORE EcoFriendly Properties 11/2019 – present • Founder Men’s Health Survivorship Foundation 10/2018 - present • Board Certified Urologic Surgeon – Advent Health Tampa 10/2017 - 10/2020 Physician Group Urology • Adjunct Faculty - Lincoln Memorial University DCOM 02/2018 – 10/2020 • Consultant Boston Scientific 05/2019 – present 05/2019 - present • Consultant Myriad Genetics • Aquatics Student Coordinator Campus Recreation at University 06/2006 - 06/2008 of Illinois • Assistant Store Manager Valvoline Instant Oil Change 06/2001 - 08/2004 Jared J. -

Counter Incision Is a Safe and Effective Method for Alternative Reservoir Placement During Inflatable Penile Prosthesis Surgery
2696 Original Article Counter incision is a safe and effective method for alternative reservoir placement during inflatable penile prosthesis surgery Dominic Grimberg1^, Sabrina Wang2, Evan Carlos1, Brent Nosé1, Shelby Harper2, Aaron C. Lentz1 1Division of Urology, Duke University Medical Center, Durham, NC, USA; 2Duke University School of Medicine, Durham NC, USA Contributions: (I) Conception and Design: D Grimberg, E Carlos, AC Lentz; (II) Administrative support: D Grimberg, B Nosé, S Wang, S Harper; (III) Provision of study materials or patients: AC Lentz; (IV) Collection and assembly of data: D Grimberg, B Nosé, S Wang, S Harper, E Carlos; (V) Data analysis and interpretation: D Grimberg, E Carlos, B Nosé, AC Lentz; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Dr. Dominic Grimberg. Division of Urology, Duke University Medical Center, Room 1573, White Zone, Durham, NC, 27710, USA. Email: [email protected]. Background: Alternative reservoir placement is increasingly popular during inflatable penile prosthesis (IPP) surgery to prevent intraperitoneal positioning, bowel, bladder, or vascular injury in patients with prior pelvic surgeries. Counter incision (CI) can be used for submuscular reservoir placement in high risk patients, however series exploring the safety remain limited. Methods: A database of IPP surgeries was queried for use of a CI during reservoir placement to compare 90-day clinical outcomes in a retrospective case-control study. Primary outcome was device infections, with secondary outcomes including reservoir herniation, hematoma, device malfunction rates, and operative times. Groups were compared using Kruskal-Wallis and Chi-Squared tests, with multivariate logistic regression models to identify predictors of infectious complications. -

Quality of Life Outcomes After Brachytherapy for Early Prostate Cancer
Prostate Cancer and Prostatic Diseases (1999) 2 Suppl 3, S19±S20 ß 1999 Stockton Press All rights reserved 1365±7852/99 $15.00 http://www.stockton-press.co.uk/pcan Quality of life outcomes after brachytherapy for early prostate cancer MS Litwin1, JM Brandeis1, CM Burnison1 and E Reiter1 1UCLA Departments of Urology, Health Services, and Radiation Oncology, UCLA, California, USA Despite the absence of empirical evidence, there is a XRT. Sildena®l appeared to have little effect in the radical popular perception that brachytherapy results in less prostatectomy patients. However, brachytherapy patients impairment of health-related quality of life. This study not receiving hormonal ablation or XRT who took silde- compared general and disease-speci®c health-related na®l had better sexual function and bother scores than quality of life in men who had undergone either brachy- those patients who did not. therapy (with and without pre-treatment XRT) or radical prostatectomy, and in healthy age-matched controls. Method Conclusion We surveyed all patients with clinical T2 or less prostate General health-related quality of life did not differ greatly cancer who had undergone interstitial seed brachyther- between the three groups, but there were variations in apy at UCLA during the previous 3±17 months. Each was disease-speci®c (urinary, bowel and sexual) health-related paired with two randomly selected, temporally matched quality of life. Radical prostatectomy patients had the radical prostatectomy patients. Healthy, age-matched worst urinary function (leakage), but brachytherapy controls were drawn from the literature. Surgery and patients were also signi®cantly worse than the controls. -

Penile Prosthesis Implantation Fried Symposium 2016
Penile Prosthesis Implantation Fried Symposium 2016 Culley C. Carson III, MD, FACS, FRCS(hon) University of North Carolina Chapel Hill, N.C. Management of ED All Patients Sexual/ Physical Exam Laboratory Tests Medical History Discuss Options Noninvasive Tx Additional Tests (Oral, VED, MUSE, PEP) (NPT, Doppler, DICC) Surgical/Invasive Tx ** Penile Prosthesis History • Bogaras(1936)-Rib • Pearman(1967)- cartilage Trimable silicone • Frumkin(1943)-Rib implant cartilage • Morales(1973)- • Scardino (1950)- Intracavernosal Acrylic stent implant • Goodwin & • Small & Scott(1952)-Acrylic Carrion(1973)- stent Intracavernosal • Lash(1964)-Silicone implant implant • Scott(1973)-Inflatable implant Types of Prostheses • Malleable/semirigid – AMS, Coloplast, Jonas • Mechanical rod – AMS Dura II • Inflatable – 2-piece – AMS Ambicor – 3-piece – • AMS 700 (CX, CXR, LGX) • Coloplast (Alpha-1, Titan, Narrow Base) Penile Prosthesis Modifications • Single tubing connectors • Lock-out valve in fluid reservoir or pump to prevent autoinflation • Parylene Coating • Pump Improvements – MS (AMS) – OTR (Coloplast) • Prevention of infections – Antibiotic-impregnated coating (InhibiZone™, AMS) – Hydrophilic/anti-adherence surface (Titan, Mentor) Penile Implant Indications • Oral drug (PDE5 inhibitor) failure • Radical Prostatectomy • Diabetes mellitus • Cardiovascular • Scarred penis – Priapism – Previous implant – Trauma • Peyronie’s disease • Severe venous leak Issues Regarding Informed Consent • Size of penis—usually slight loss in penile length • Possible need -

Prostate Biopsy in the Staging of Prostate Cancer
Prostate Cancer and Prostatic Diseases (1997) 1, 54±58 ß 1997 Stockton Press All rights reserved 1365±7852/97 $12.00 Review Prostate Biopsy in the staging of prostate cancer L Salomon, M Colombel, J-J Patard, D Gasman, D Chopin & C-C Abbou Service d'Urologie, CHU, Henri Mondor, CreÂteil, France The use of prostate biopsies was developed in parallel with progress in our knowledge of prostate cancer and the use of prostate-speci®c antigen (PSA). Prostate biopsies were initially indicated for the diagnosis of cancer, by the perineal approach under general anesthesia. Nowadays prostate biopsies are not only for diagnostic purposes but also to determine the prognosis, particularly before radical prostatectomy. They are performed in patients with elevated PSA levels, by the endorectal approach, sometimes under local anesthesia.(1±3) The gold standard is the sextant biopsy technique described by Hodge4,5, which is best to diagnose prostate cancer, particularly in case of T1c disease (patients with serum PSA elevation).6±13 Patients with a strong suspicion of prostate cancer from a negative series of biopsies can undergo a second series14;15 with transition zone biopsy16,17 or lateral biopsy.18,19 Karakiewicz et al 20 and Uzzo et al 21 proposed that the number of prostate biopsies should depend on prostate volume to improve the positivity rate. After the diagnosis of prostate cancer, initial therapy will depend on several prognostic factors. In the case of radical prostatectomy, the results of sextant biopsy provide a wealth of information.22,23 The aim of this report is to present the information given by prostate biopsy in the staging of prostate cancer. -

Selected Non-Moderated Posters
International Journal of Impotence Research (2001) 13, Suppl 2, S17±S21 ß 2001 Nature Publishing Group All rights reserved 0955-9930/01 $15.00 www.nature.com/ijir Selected Non-moderated Posters 12 \' ASECOMY llEHA \'!ORAL EFFECTS IN MEN Authors: T. Bandel; R. Bauer; T. Sigerson. Bayer AG., Wuppertal, Germany Aragao, A J, Rodrigues A 0., Agostinho AG., Juliano, RV. \1arinc!li CM., Affiliation: Pharmacology, Bayer AG, Wuppertal, Germany Wroclavski, ER., Bozzo, I.S Objective: Evaluate the satisfaction degree and the behavioral effecb or vasectomy in the couple and in the man in matter VARDENAFIL'S IMPROVEMENT ON THE QUALITY OF ERECTIONS CAN BE Method There were selected 113 men submit1ed to sterilization by vasectomy, in DEMONSTRATED EARLY IN RIGfSCAN™ STUDIES. the period from January of 1996 to January of 1999, after approval of the Ethics ·commission of Family Planning Service from the Faculdadc de Medicina do ABC. A.JI the patients were called b~· Introduction and Objectives letter. telegram or phone calls, in a spontaneous way and not obligatory A di red questionnaire Vardenafil is a new highly selective PDE5 inhibitor that is being developed for treatment of \Vas used approaching the following: self-esteem aspects, orgasm corHroL sexual satisfaction, erectile dysfunction. ln two Phase Ila studies with patients with mild to moderate erectile complications, sexual habit and masturbation dysfunction, Rigiscan™ measurements of quality of erections were determined. The objective Results: 23,5% of the patients told that, the sexual relationship performance got of this retrospective analysis was to compare the effect ofvardcnafil on the strength of better and 71% didn't notice difference, 5,9% thought worst. -

Needle Biopsy and Radical Prostatectomy Specimens David J Grignon
Modern Pathology (2018) 31, S96–S109 S96 © 2018 USCAP, Inc All rights reserved 0893-3952/18 $32.00 Prostate cancer reporting and staging: needle biopsy and radical prostatectomy specimens David J Grignon Department of Pathology and Laboratory Medicine, Indiana University School of Medicine, IUH Pathology Laboratory, Indianapolis, IN, USA Prostatic adenocarcinoma remains the most common cancer affecting men. A substantial majority of patients have the diagnosis made on thin needle biopsies, most often in the absence of a palpable abnormality. Treatment choices ranging from surveillance to radical prostatectomy or radiation therapy are largely driven by the pathologic findings in the biopsy specimen. The first part of this review focuses on important morphologic parameters in needle biopsy specimens that are not covered in the accompanying articles. This includes tumor quantification as well as other parameters such a extraprostatic extension, seminal vesicle invasion, perineural invasion, and lymphovascular invasion. For those men who undergo radical prostatectomy, pathologic stage and other parameters are critical in prognostication and in determining the appropriateness of adjuvant therapy. Staging parameters, including extraprostatic extension, seminal vesicle invasion, and lymph node status are discussed here. Surgical margin status is also an important parameter and definitions and reporting of this feature are detailed. Throughout the article the current reporting guidelines published by the College of American Pathologists and the International Collaboration on Cancer Reporting are highlighted. Modern Pathology (2018) 31, S96–S109; doi:10.1038/modpathol.2017.167 The morphologic aspects of prostatic adenocarcinoma hormonal therapy.4,5 For needle biopsy specimens the have a critical role in the management and prognos- data described below are largely based on standard tication of patients with prostatic adenocarcinoma. -

WEB UCLA1671 the Men's Clinic at UCLA Brochure
The Men’s Clinic at UCLA Discretion, dignity and respect Te Men’s Clinic at UCLA is dedicated to male health and, in particular, to the treatment of conditions afecting men’s urologic, sexual and reproductive health. With years of clinical experience in male reproductive medicine and surgery, our team has treated a wide variety of conditions and performed thousands of surgeries, providing patients with the highest level of quality, leading-edge care. Our providers understand the intimate nature of male fertility and sexual difculties and treat all men with discretion, dignity and respect. Our clinical programs specialize in: • Infertility • Sperm retrieval • Vasectomy • Vasectomy reversal • Erectile dysfunction (ED) • Post-prostatectomy erectile dysfunction (PPED) and penile rehabilitation • Peyronie’s disease • Low testosterone (hypogonadism) The patient experience Nearly one-third of men today report that they do not use a regular source of healthcare and are typically less likely than women to undergo routine checkups or openly discuss their medical issues. As a result, men are missing impactful opportunities for a healthy lifestyle, as well as preventive screenings for a variety of male medical conditions. At Te Men's Clinic at UCLA, our uniquely tailored program allows men to feel welcome, at ease and cared for when seeking answers to intimate health issues. 1 Male fertility Infertility When couples struggle with infertility, timely evaluation of the male partner is crucial. Te Men’s Clinic at UCLA ofers all aspects of male fertility diagnosis and treatment, as well as in-house, same-day semen analysis testing for instant results, so couples don’t have to anxiously wait. -
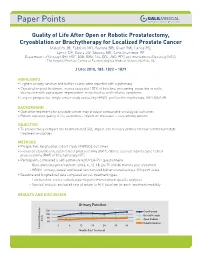
Quality of Life After Open Or Robotic Prostatectomy, Cryoablation Or
Quality of Life After Open or Robotic Prostatectomy, Cryoablation or Brachytherapy for Localized Prostate Cancer Malcolm JB, Fabrizio MD, Barone BB, Given RW, Lance RS, Lynch DF, Davis JW, Shaves ME, Schellhammer PF Departments of Urology (JBM, MDF, BBB, RWG, RSL, DFL, JWD, PFS) and Interventional Radiology (MES), The Virginia Prostate Center at Eastern Virginia Medical School, Norfolk, VA J Urol 2010, 183: 1822 – 1829 HIGHLIGHTS • Highest urinary function and bother scores were reported with cryotherapy • Cryoablation post treatment scores exceeded 100% of baseline, presuming reduction in outlet obstruction with subsequent improvement in obstructive and irritative symptoms • Largest prospective, single center study evaluating HRQOL profiles for cryotherapy, ORP, RAP, BT BACKGROUND • Operative treatments for prostate cancer may produce comparable oncological outcomes • Patient reported quality of life outcomes – important measures – vary among options OBJECTIVE • To prospectively compare the health related QOL impact and recovery profiles for four common prostate treatment modalities METHODS • Prospective, longitudinal cohort study of HRQOL outcomes • Evaluated cryoablation, open radical prostatectomy (ORP), robotic assisted laparoscopic radical prostatectomy (RAP) or brachytherapy (BT) • Participants completed a self-administered UCLA-PCI questionnaire - Questionnaires pre treatment and 3, 6, 12, 18, 24, 30 and 36 months post treatment - HRQOL urinary, sexual and bowel function and bother scored using a 100-point scale • Baseline and -

ARRO Case: HDR Prostate Brachytherapy
ARRO Case: HDR Prostate Brachytherapy Karna Sura, MD (PGY-5) Faculty Advisor: Sirisha Nandalur, MD Department of Radiation Oncology Beaumont Health Case Presentation • 67 year old male presented with an elevated PSA at 3.55 ng/mL • Found to have no evidence of abnormalities on DRE • Underwent prostate biopsy May 22, 2018 Case presentation continued • Discussed various treatment options including: – Active surveillance – Radical prostatectomy – External beam radiation – HDR prostate brachytherapy as a monotherapy – Other options include LDR brachytherapy and SBRT • Patient wanted to proceed with brachytherapy May 22, 2018 Brief History of Prostate Brachytherapy • 1917 – Barringer inserted radium needles transperineally in the prostate • 1952 – Flocks et al. injected radioactive gold solution into prostate cancer • 1972 – Willet Whitmore described an open implant technique using 125I • 1983 – H. Holm described technique of implanting the prostate with radioactive seeds May 22, 2018 Radiobiology behind prostate brachytherapy • Prostate tumors have small fraction of cycling cells and possibly a low α/β ratio • A meta-analysis of 20+ studies has estimated the α/β ratio between 1-4 Gy with a mean of 2.7 Gy • Thus, hypofractionation might be more effective for prostate cancer Patient history • Urologic history – Prior transurethral or open resection of the prostate or other surgery on the urethra – Prior procedure for BPH – Medication for urinary obstructive symptoms – Erectile function • Prior diagnosis of cancer, especially rectal or bladder -

Robotic-Assisted Laparoscopic Radical Prostatectomy After Aborted Retropubic Radical Prostatectomy
J Robotic Surg (2013) 7:301–304 DOI 10.1007/s11701-012-0377-9 CASE REPORT Robotic-assisted laparoscopic radical prostatectomy after aborted retropubic radical prostatectomy Keith J. Kowalczyk • Andy C. Huang • Stephen B. Williams • Hua-yin Yu • Jim C. Hu Received: 11 March 2012 / Accepted: 31 July 2012 / Published online: 19 August 2012 Ó Springer-Verlag London Ltd 2012 Abstract Robotic-assisted laparoscopic prostatectomy of the endopelvic fascia due to poor visualization, a (RALP) has surged in popularity since US Food and Drug prominent pubic tubercle, and a narrow pelvis. The Administration approval in 2000. Advantages include enhanced visualization and precision of the robotic plat- improved visualization and increased instrument dexterity form allowed adequate exposure of the prostate and within the pelvis. Obesity and narrow pelves have been allowed us to proceed with an uncomplicated prostatecto- associated with increased difficulty during open retropubic my, which was not possible to perform easily via an open radical prostatectomy (RRP), but the robotic platform approach. The bladder was densely adherent to the pubis theoretically allows one to perform a radical prostatectomy and the anterior prostatic contour and apex were difficult to despite these challenges. We present an example of a develop due to a dense fibrotic reaction from the previous RALP performed following an aborted RRP. A 49-year-old endopelvic fascia incision. However, we were able to male with intermediate risk prostate cancer and body mass successfully complete RALP with subtle technical modi- index of 38 kg/m2 presented for RALP after RRP was fications. Estimated blood loss was 160 mL and operating aborted by an experienced open surgeon following incision time was 145 min. -

Life After Prostate Cancer Insights to Help You Live Life Restored Hope
Life after prostate cancer Insights to help you live life restored Hope. Recovery. Support. Every year, more than 1.1 million men are diagnosed with prostate cancer globally. It is the second most commonly diagnosed cancer in men worldwide.1 If detected early, prostate cancer is usually curable. Prostate cancer is a journey, now Like many men, you have undergone surgical treatment for your prostate cancer. Advances in surgical techniques have allowed surgeons to successfully it’s your time to be in the driver’s operate on a growing number of patients, and surgery offers the greatest chance for cure for localized prostate cancer.2 seat with your recovery. As you move into the recovery phase of your journey, we have put together this resource kit designed to provide you with important information about what to expect after your surgery, tracking your progress, support options and other important things to know during the coming months. 2 3 Recovering bladder control and erections In order to remove the cancer, the mechanisms in your body that help control ONE your urine flow and ability to get an erection may have been damaged. Most men are understandably concerned about their ability to regain bladder control and erections following their prostate surgery. Regaining continence You are beating back cancer, so hold your head up with dignity. While getting rid of the cancer is most patients’ top concern, the fear of While men often experience incontinence (leaking of urine) immediately following surgery, the leakage usually tapers off within several weeks or months.3 When incontinence persists beyond becoming incontinent is often on a man’s mind.