A Short Term Study on Dengue Incidence in Relation to Gender in Some Districts of Rajasthan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

District Census Handbook, Bikaner, Rajasthan
CENSUS OF INDIA 1961 RAJASTHAN DISTRICT CENSUS HANDBOOK BIKANER DISTRICT C. S. GUPTA OF THE INDlAN ADMINlS'l'RATlVE: SERVICE Superintendent of Census Operations, Rajasthan Printed by Mafatlal Z. Gandhi. at Nayan Printing Preis. Ahmedabad-I. FOREWORD The Census data has always been considered as indispensable for day to day administration. ] t is increasingly being considered now as the foundation stone or' all regional planning. The publication of this series of District Census Handbooks wherein census statistics is made available for smaller territorial units is. therefore~ a significant occasion for it fills many existing gaps in statistics at the lower levels. Many interesting details have been revealed by the Census 1961 and I hope persons engaged in the administration of the State and public in general will appreciate the value and the effort that has gone into the production of such a standard book of reference. 1 congratulate the Superintendent of Census Operations, Rajasthan, Shri C. S. Gupta I. A. S. and his colleagues who have done a good job with skill and perseverence. B. MEHTA JAIPUR, Chief Secretary 1st March, 1966. to the Government of Rajasthan. iii PREFACE The District Census Handbooks, to which series the present volume belongs. are the gifts of the Census of India and were first introduced in 1951. The 1961 series of District Census Handbooks are more elaborate than their counter-part in 1951 and present all important cen,slls data alon~with such other basic information as is very relevant for an understanding of the district. A wide variety of information which the Census 1961 collected: has already been released in several parts as mentioned elsewhere in this book. -

Circle District Location Acc Code Name of ACC ACC Address
Sheet1 DISTRICT BRANCH_CD LOCATION CITYNAME ACC_ID ACC_NAME ADDRESS PHONE EMAIL Ajmer RJ-AJM AJMER Ajmer I rj3091004 RAJESH KUMAR SHARMA 5849/22 LAKHAN KOTHARI CHOTI OSWAL SCHOOL KE SAMNE AJMER RA9252617951 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3047504 RAKESH KUMAR NABERA 5-K-14, JANTA COLONY VAISHALI NAGAR, AJMER, RAJASTHAN. 305001 9828170836 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3043504 SURENDRA KUMAR PIPARA B-40, PIPARA SADAN, MAKARWALI ROAD,NEAR VINAYAK COMPLEX PAN9828171299 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3002204 ANIL BHARDWAJ BEHIND BHAGWAN MEDICAL STORE, POLICE LINE, AJMER 305007 9414008699 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3021204 DINESH CHAND BHAGCHANDANI N-14, SAGAR VIHAR COLONY VAISHALI NAGAR,AJMER, RAJASTHAN 30 9414669340 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3142004 DINESH KUMAR PUROHIT KALYAN KUNJ SURYA NAGAR DHOLA BHATA AJMER RAJASTHAN 30500 9413820223 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3201104 MANISH GOYAL 2201 SUNDER NAGAR REGIONAL COLLEGE KE SAMMANE KOTRA AJME 9414746796 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3002404 VIKAS TRIPATHI 46-B, PREM NAGAR, FOY SAGAR ROAD, AJMER 305001 9414314295 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3204804 DINESH KUMAR TIWARI KALYAN KUNJ SURYA NAGAR DHOLA BHATA AJMER RAJASTHAN 30500 9460478247 [email protected] Ajmer RJ-AJM AJMER Ajmer I rj3051004 JAI KISHAN JADWANI 361, SINDHI TOPDADA, AJMER TH-AJMER, DIST- AJMER RAJASTHAN 305 9413948647 [email protected] -

Census Atlas, Part IX-B, Vol-XIV, Rajasthan
PRG. 173 B (N) (Ordy.) 1,000 CENSUS OF INDIA 1961 VOLUME XIV RAJASTHAN PART IX-B CENSUS ATLAS C. S. GUPTA OF THE INDIAN ADMINISTRATIVE SERVICE Superintendent of Census Op~rations, RajalJhan 1969 FOREWORD FEW PEOPLE REALIZE, much less appreciate, that apart from the Survey of India and the Geological Survey, the Census of India had' been perhaps the largest single producer of maps of the Indian subcontinent. Intimate collaboration between geographer and demographer began quite early in the modern era, almost two centuries before the first experiments in a permanent decennial Census were made in the 1850's. For example, the population estimates of Fort St. George, Madras, made in 1639 and 1648, and of Masulipatnam and Bombay by Dr. John Fryer, around 1672-73 were supported by cartographic documents of no mean order, Tbe first detailed modern maps, the results of Major James Rennell's stupendous Survey of 1767-74, were published in 1778-1780 and Henry Taylor Colebrooke, almost our first systematic demographer, was quick to make good use of them by making estimates of population in the East India Company's Possessions in the 1780's. Upjohn's map of Calcutta City, drawn in 1792.93, reprinted in the Census Report of Calcutta for 195 I, gives an idea of the standards of cartographic excellence reached at that period. In the first decade of the nineteenth century, Francis Buchanan Hamilton improved upon Colebrooke's method in which he was undoubtedly helped by the improved maps prepared for the areas he surve ed. It is possible that the Great Revenue Survey, begun in the middle of the last century, offered the best guarantee of the success of decennial population censuses proposed shortly before the Mutiny of 1857. -
Audit & Assessment of Qos for Qe-September-2014
AUDIT & ASSESSMENT OF QOS FOR QE-SEPTEMBER-2014-RAJASTHAN CIRCLE Audit & Assessment of Quality of Service Of Cellular Mobile Telephone Service For Telecom Regulatory Authority Of India North Zone – Rajasthan Service Area (July 2014 – September 2014) Prepared by TÜV SÜD SOUTH ASIA PVT. LTD, C-153/1, Okhla Industrial Estate, Phase-1, New Delhi – 110020 Telephone 011- 30889611 TUV-SUD SOUTH ASIA PRIVATEUNICEF LIMITED Lucknow OfficePage 1 Fax: 011-30889595 AUDIT & ASSESSMENT OF QOS FOR QE-SEPTEMBER-2014-RAJASTHAN CIRCLE PREFACE The Telecom Regulatory Authority of India (TRAI) was established in 1997 by an Act of Parliament, called the Telecom Regulatory Authority of India Act, 1997, to regulate telecom services. The Authority‟s mission is to ensure that the interest of consumers are protected and at the same time to nurture conditions for growth of telecommunications, broadcasting and cable services in a manner and at a pace which will enable India to play a leading role in emerging global information society. The Authority, in exercise of its functions as per the provisions in the TRAI Act, has been entrusted to measure the Quality of Service provided by the Service Providers from time to time and to compare them with the benchmarks so as to assess the level of performance. In pursuance of this, TRAI has appointed M/s TUV-SUD South Asia Pvt. Ltd. to carry out “Audit and Assessment of Quality of Service” provided by Basic (Wire line), Cellular Mobile and Broadband service providers in terms of the benchmarks specified in the respective regulations, in North and West Zones. -
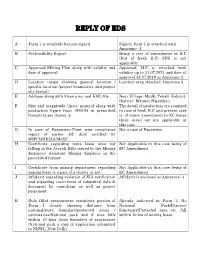
Reply of Eds
REPLY OF EDS A Form 1 is available but not signed Signed form-1 is attached with Annexure -1 B Prefeasibility Report. Being a case of amendment in E.C (Not of fresh E.C) PFR is not applicable C Approved Mining Plan along with validity and Approved M.P is attached with date of approval validity up to 11.07.2024 and date of approval 12.07.2019 as Annexure-2 D Location (maps showing general location / Location map attached Annexure-3 specific location /project boundaries and project site layout). E Address along with khasra no. and KML file. Near Village- Mudh, Tehsil- Koloyat, District- Bikaner,Rajasthan F Size and magnitude (Area, mineral along with The detail of production are required production figure from 1993-94 in prescribed in case of fresh E.C and present case format)As per Annex. g is of minor amendment in EC hence these detail are not applicable in this case. G In case of Expansion-Point wise compliance Not a case of Expansion report of earlier EC duly certified by RSPCB/SEIAA/MoEF. H Certificate regarding mine lease area not Not Applicable in this case being of falling in the Aravali Hills issued by the Mining EC Amendment Engineer/ Assistant Mining Engineer in the prescribed format I Certificate from mining department regarding Not Applicable in this case being of mining lease is a part of a cluster or not EC Amendment J Affidavit regarding violation of EIA notification Affidavit is enclosed as Annexure- 4 and regarding correctness of submitted data & document by consultant as well as project proponent. -

Conserving Water & Biodiversity: Traditions of Sacred Groves in India
European Journal of Sustainable Development (2016), 5, 4, 129-140 ISSN: 2239-5938 Doi: 10.14207/ejsd.2016.v5n4p129 Conserving Water & Biodiversity: Traditions of Sacred Groves in India Mala Agarwal1 Abstract Sacred groves, a wide spread phenomenon in cultures across the world, are often associated with religion & culture, are instrumental in preserving biodiversity and nature without being questioned. Scattered all over India e.g. scrub forests in the Thar Desert of Rajasthan maintained by the Bishnois, Hariyali in Uttarakhand, Shinpin in Himachal Pradesh and associated with religion they are often sacrosanct. The sacred groves are self sustained ecosystem and conserve the endemic, endangered & threatened species, medicinal plants and wide variety of cultivars. Water and soil conservation is the most well documented ecological service provided by the sacred groves that helps prevent flash floods and ensures supply of water in lean season in the desert of Rajasthan. Encountering threats like fragmentation, urbanization, and overexploitation now they need governmental support to exist e.g. Introduction of the ‘Protected Area Category Community Reserves’ under the Wild Life (Protection) Amendment Act, 2002. Key words-Water conservation, eco-system, bio diversity, sacred groves. 1. Introduction Sacred Groves are considered as “Sacred Natural Sites” (IUCN) [1].These are the relic forest patches preserved in the name of religion & culture. They extend from Asia, Africa, and Europe to America mostly in Africa and Asia [2]. In India, Groves are present from North-east Himalayan region, Western & Eastern Ghats, Coastal region, Central Indian Plateau and Western desert [3]. Indian sacred groves have pre-Vedic origin. They are associated with indigenous / tribal communities who believe in divinity of nature and natural resources. -

Give and Take
SIT Graduate Institute/SIT Study Abroad SIT Digital Collections Independent Study Project (ISP) Collection SIT Study Abroad Spring 2014 Give and Take: The trS uggle of Being a Part of the System you Want to Change- Childline: Solving and Perpetuating Child Vulnerability in Bikaner, Rajasthan, India Angela Soley SIT Study Abroad Follow this and additional works at: https://digitalcollections.sit.edu/isp_collection Part of the Family, Life Course, and Society Commons, Inequality and Stratification Commons, Politics and Social Change Commons, and the Social Welfare Commons Recommended Citation Soley, Angela, "Give and Take: The trS uggle of Being a Part of the System you Want to Change- Childline: Solving and Perpetuating Child Vulnerability in Bikaner, Rajasthan, India" (2014). Independent Study Project (ISP) Collection. 1821. https://digitalcollections.sit.edu/isp_collection/1821 This Unpublished Paper is brought to you for free and open access by the SIT Study Abroad at SIT Digital Collections. It has been accepted for inclusion in Independent Study Project (ISP) Collection by an authorized administrator of SIT Digital Collections. For more information, please contact [email protected]. Soley 1 GIVE AND TAKE: THE STRUGGLE OF BEING A PART OF THE SYSTEM YOU WANT TO CHANGE- CHILDLINE: SOLVING AND PERPETUATING CHILD VULNERABILITY IN BIKANER, RAJASTHAN, INDIA Angela Soley Academic Director: Tara Dhakal Project Advisor: Arvind Ojha, URMUL Trust School for International Training India: Sustainable Development and Social Change Program Spring 2014 Soley 2 Ackowledgements: I would like to express my deep gratitude to Tara-ji and Trilochan-ji, for helping me through every step of this process and giving me invaluable advice while in the field. -

Impact of National Food Security Mission with Special Reference to Adoption Level to Field Demonstration Interventions in Gram Crop in Southern Rajasthan
DOI: 10.15740/HAS/AU/12.2/315-318 Agriculture Update Visit us : www.researchjournal.co.in AU Volume 12 | Issue 2 | May, 2017 | 315-318 e ISSN-0976-6847 RESEARCH ARTICLE : Impact of National Food Security Mission with special reference to adoption level to field demonstration interventions in gram crop in southern Rajasthan RAM LAL KHATIK, F.L. SHARMA, H.K. JAIN, SANTOSH DEVI SAMOTA AND R.K. DAMOR ARTICLE CHRONICLE : SUMMARY : The present study was conducted in Banswara and Udaipur districts of Southern Received : Rajasthan. Total 120 gram beneficiary and non-beneficiary farmers were selected on the basis of random 29.03.2017; sampling method from the identified districts. The findings reveal that the extent of adoption of RSG- Received : 888 variety of gram among beneficiary farmers was recorded 86.25 per cent, while in case of non- 12.04.2017; beneficiary farmers it was 61.25 per cent. In case of extent of adoption of the complete package of Accepted : practices of RSG-888 variety of gram, it was found that beneficiary and non-beneficiary farmers had 26.04.2017 83.75 and 62.50 per cent adoption, respectively. How to cite this article : Khatik, Ram Lal, Sharma, F.L., Jain, H.K., Samota, Santosh Devi and Damor, R.K. (2017). Impact of National Food Security Mission with special reference to adoption level to field demonstration KEY WORDS : interventions in gram crop in southern Rajasthan. Agric. Update, 12(2): 315-318; DOI : 10.15740/HAS/AU/12.2/ NFSM, Beneficiary, 315-318. Interventions, Adoption, Demonstration BACKGROUND AND OBJECTIVES Dungarpur and Banswara districts of southern Rajasthan since 2010. -
Annexure-District Survey Report
DISTRICT SURVEY REPORT BIKANER DISTRICT 1. INTRODUCTION: Bikaner district is located in the north-western part of Rajasthan and encompassedbetween north latitudes 27°11’ to 29°03’ and east longitudes 71°52’ to 74°15’covering geographical area of 30247.90 Sq. kms. It is bounded on the north byGanganagar District, on the east by Hanumangarh and Churu Districts, on south byNagaur and Jodhpur Districts and on the west by Jaisalmer District and Internationalborder with Pakistan. For administration and development, the district is divided intoeight sub-divisions i.e. Bikaner, Kolayat, Nokha, Loonkaransar, Khajuwala, Chhattargarh, Pugal and Dungargarh and eight tehsils, i.e., BIkaner, Kolayat, Nokha, Loonkaransar, Khajuwala, Chhattargarh, Poogal and Dungargarh. Thedevelopmental activities of the district are being looked after by six Panchayat Samities, i.e. Bikaner, Kolayat, Nokha, Loonkaransar, Khajuwala and Dungargarh. There are 874 villages and 219 Gram panchayats. There is one independent Sub-Tehsil Bajju situated in Kolayat tehsil for better administration. The district has one Municipal Council, 219 Gram Panchayats and 874 Villages. As per 20011 Census, the total population of the district is 2363937 out of which 1563553 is rural population and 800384 is urban population. 1. OVERVIEW OF MINING ACTIVITY IN THE DISTRICT: In Bikaner district various types of minerals available under minor category such as Gypsum, Ball clay, Fullers earth, Limestone, Bajri-Gravel, sandstone etc. About 240 leases of these minerals are operating in the district. 2. LIST OF MINING LEASES IN DISTRICT WITH LOCATION, AREA AND PERIOD OF VALIDITY: 1 Sl.n Name of Ml No. Mine name Area Village Tehsil District Period o. -

O Rigin Al a Rticle
International Journal of Agricultural Science and Research (IJASR) ISSN(P): 2250-0057; ISSN(E): 2321-0087 Vol. 8, Issue 4 Aug 2018, 27-32 © TJPRC Pvt. Ltd. ANALYSIS OF METEROLOGICAL DROUGHT FOR AJMER AND BIKANER DISTRICT OF RAJASTHAN P. YOGITHA 1 & H. SANDEEP 2 1Senior Research Fellow, Department of Soil and Water Engineering (NRM Natural Resource Management Division), ICAR-CRIDA (Central Research Institute for Dryland Agriculture), Santoshnagar, Hyderabad, India 2Research Associate, Department of Soil and Water Engineering (NRM Natural Resource Management Division), ICAR-CRIDA (Central Research Institute for Dryland Agriculture), Santoshnagar, Hyderabad, India ABSTRACT Drought is an insidious hazard and is a protracted period of deficient precipitation resulting in extensive damage to crops, resulting in loss of yield and its impact vary from region to region. It conditions result from a lack of precipitation and can worsen after prolonged periods of no rainfall, especially in areas where the water supply is short. The main objective of the research to develop an approach and analyses of meteorological droughts based on precipitation data. If the mean weekly rainfall for 30 years of data from 1987 to 2016, then a week receiving rainfall less than 75 per cent of mean weekly rainfall is defined as drought week and greater than 125 per cent of mean weekly Article Original rainfall is defined as the surplus week. Week having rainfall between 75 per cent of mean weekly rainfall and 125 per cent of mean weekly rainfall is considered as the normal week. Rainfall Variability is the availability of water at a particular time and area. -

Final Population Figures, Series-18, Rajasthan
PAPER 1 OF 1982 CENSUS OF INDIA 1981 SERIES 18 RAJASTHAN fINAL POPULATION FIGU~ES (TOTAL POPULATION, SCHEDULED CASTE POPULATION AND .sCHEDULED TRIBE POPULATION) I. C. SRIVASTAVA ·1)f the Indian Administrative Service Director of Census Operations Rajasthan INTRODUCfION The final figures of total population, scheduled caste and scheduled tribe population of Rajasthan Stat~ are now ready for release at State/District/Town and Tehsil levels. This Primary Census Abs tract, as it is called, as against the provisional figures contained in our three publications viz. Paper I, fFacts & Figures' and Supplement to Paper-I has been prepared through manual tabulation by over 1400 census officials including Tabulators, Checkers and Supervisors whose constant and sustained efforts spread over twelve months enabled the Directorate to complete the work as per the schedule prescribed at the national level. As it will take a few months more to publish the final population figures at the viJ1age as well as ward levels in towns in the form of District Census Handbooks, it is hoped, this paper will meet the most essential and immediate demands of various Government departments, autonomous bodies, Cor porations, Universities and rtsearch institutions in relation to salient popUlation statistics of the State. In respect of 11 cities with One lac or more population, it has also been possible to present ~the data by municipal wards as shown in Annexure. With compliments from Director of Census Operations, Rajasthan CONTENTS INTRODUCTION (iii) Total Population, Scheduled Caste and Scheduled Tribt' Population by Districts, 1981 Total Schedu1ed Caste and Scheduled Tribe Population. ( vi) 1. Ganganagar District 1 2. -

Brief Industrial Profile of Bikaner District
Government of India Ministry of MSME Brief Industrial Profile of Bikaner District Carried out by MSME-Development Institute (Ministry of MSME, Govt. of India,) 22 Godam, Industrial Estate, Jaipur-302006 Phone: 0141-2212098, 2213099 Fax: 0141-2210553 e-mail: [email protected] 1 Contents S. No. Topic Page No. 1. General Characteristics of the District 4 1.1 Location & Geographical Area 4 1.2 Topography 4 1.3 Availability of Minerals. 5 1.4 Forest 6 1.5 Administrative set up 6,7 2. District at a glance 7,8,9 2.1 Existing Status of Industrial Area in the District Bikaner 10 3. Industrial Scenario of the District Bikaner 11 3.1 Industry at a Glance 11 3.2 Year Wise Trend Of Units Registered 11 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units In The 12,13 District 3.4 Large Scale Industries / Public Sector undertakings 14 3.5 Major Exportable Item 14 3.6 Growth Trend 14 3.7 Vendorisation / Ancillarisation of the Industry 14 3.8 Medium Scale Enterprises 15 3.8.1 List of the units in Bikaner & nearby Area 15 3.8.2 Major Exportable Item 15 3.9 Service Enterprises 15 3.9.1 List of service enterprises 15 3.9.2 Potentials areas for service industry 16 3.10 Potential for new MSMEs 16,17 4. Existing Clusters of Micro & Small Enterprise 17 4.1 Detail Of Major Clusters 17 4.1.1 Manufacturing Sector 17 4.1.2 Service Sector 17 4.2 Details of Identified cluster 18 4.2.1 Napasar Handloom Cluster, Napasar 18 4.2.2 Kasida Cluster Aaduri Poogal, Bikaner 18,19 5.