Basal Forebrain Volume, but Not Hippocampal Volume, Is a Predictor of Global Cognitive Decline in Patients with Alzheimer’S Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Synaptic Organization of Claustral and Geniculate Afferents to the Visual Cortex of the Cat
The Journal of Neuroscience December 1986, 6(12): 3564-3575 Synaptic Organization of Claustral and Geniculate Afferents to the Visual Cortex of the Cat Simon LeVay Robert Bosch Vision Research Center, Salk Institute for Biological Studies, San Diego, California 92138 Claustral and geniculate afferents to area 17 were labeled by sponses of some cortical neurons, previously called “hypercom- anterograde axonal transport of peroxidase-conjugated wheat- plex cells” by Hubel and Wiesel (1965), are suppressed as the germ agglutinin, and examined in the electron microscope. A length of the stimulating slit of light is extended beyond some peroxidase reaction protocol that led to labeling in the form of optimal value. Interestingly, neurons in the visual claustrum minute holes in the EM sections was used. Both types of affer- behave in a complementary fashion: Their responses to an ori- ents formed type 1 (presumed excitatory) synapses exclusively. ented stimulus increase monotonically with stimulus length, In agreement with previous reports the great majority of genic- sometimes showing length summation up to 40” or more-a ulate afferents to layers 4 and 6 contacted dendritic spines. The sizable portion of the animal’s entire field of view (Sherk and claustral afferents to layers 1 and 6 also predominantly con- LeVay, 198 1). tacted spines. In layer 4, however, claustral afferents contacted These observations suggest that claustral neurons contribute spines and dendritic shafts about equally. The results suggest a to end-stopping by exerting a length-dependent inhibition on substantial Claus&al input to smooth-dendrite cells in layer 4, some neurons in the visual cortex. -
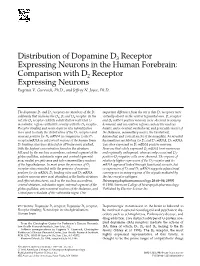
Distribution of Dopamine D3 Receptor Expressing Neurons in the Human Forebrain: Comparison with D2 Receptor Expressing Neurons Eugenia V
Distribution of Dopamine D3 Receptor Expressing Neurons in the Human Forebrain: Comparison with D2 Receptor Expressing Neurons Eugenia V. Gurevich, Ph.D., and Jeffrey N. Joyce, Ph.D. The dopamine D2 and D3 receptors are members of the D2 important difference from the rat is that D3 receptors were subfamily that includes the D2, D3 and D4 receptor. In the virtually absent in the ventral tegmental area. D3 receptor rat, the D3 receptor exhibits a distribution restricted to and D3 mRNA positive neurons were observed in sensory, mesolimbic regions with little overlap with the D2 receptor. hormonal, and association regions such as the nucleus Receptor binding and nonisotopic in situ hybridization basalis, anteroventral, mediodorsal, and geniculate nuclei of were used to study the distribution of the D3 receptors and the thalamus, mammillary nuclei, the basolateral, neurons positive for D3 mRNA in comparison to the D2 basomedial, and cortical nuclei of the amygdala. As revealed receptor/mRNA in subcortical regions of the human brain. by simultaneous labeling for D3 and D2 mRNA, D3 mRNA D2 binding sites were detected in all brain areas studied, was often expressed in D2 mRNA positive neurons. with the highest concentration found in the striatum Neurons that solely expressed D2 mRNA were numerous followed by the nucleus accumbens, external segment of the and regionally widespread, whereas only occasional D3- globus pallidus, substantia nigra and ventral tegmental positive-D2-negative cells were observed. The regions of area, medial preoptic area and tuberomammillary nucleus relatively higher expression of the D3 receptor and its of the hypothalamus. In most areas the presence of D2 mRNA appeared linked through functional circuits, but receptor sites coincided with the presence of neurons co-expression of D2 and D3 mRNA suggests a functional positive for its mRNA. -

Characterization of Basal Forebrain Glutamate Neurons Suggests a Role in Control of Arousal and Avoidance Behavior
bioRxiv preprint doi: https://doi.org/10.1101/2020.06.17.157479; this version posted June 18, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. This article is a US Government work. It is not subject to copyright under 17 USC 105 and is also made available for use under a CC0 license. Title: Characterization of basal forebrain glutamate neurons suggests a role in control of arousal and avoidance behavior Authors: James T. McKenna1, Chun Yang1, Thomas Bellio2, Marissa B. Anderson-Chernishof1, Mackenzie C. Gamble2, Abigail Hulverson2, John G. McCoy2, Stuart Winston1, James M. McNally1, Radhika Basheer1 and Ritchie E. Brown1 ORCIDs: James McKenna: 0000-0002-9710-3553 Chun Yang: 0000-0002-1979-0335 Radhika Basheer: 0000-0002-4052-6897 Ritchie Brown: 0000-0002-7164-4132 Institutional Affiliations: 1 Laboratory of Neuroscience, VA Boston Healthcare System and Harvard Medical School, Department of Psychiatry, 1400 VFW Parkway, West Roxbury, MA, 02132, USA. 2 Stonehill College, Easton, MA, 02357, USA. Running head: Basal Forebrain Glutamatergic Neurons Key words: calretinin, calbindin, parvalbumin, GAD67-GFP knock-in mice, nucleus basalis, ventral pallidum Corresponding author: Ritchie E. Brown, Dr. Rer. Nat., Address: Dept. of Psychiatry, VA Boston Healthcare System & Harvard Medical School, VA Medical Center, West Roxbury, 1400 VFW Parkway, MA, 02132, USA. Email: [email protected] Declarations: Funding: This work was supported by United States Veterans Administration Biomedical Laboratory Research and Development Service Merit Awards I01 BX004673, BX001356, I01 BX001404, I01 BX002774, I01 BX004500 and United States National Institute of Health support from NINDS R21 NS093000, NIMH R01 MH039683, NHLBI HL095491, R03- MH107650 and by SURE fellowships from Stonehill College. -

Basal Forebrain Glutamatergic Modulation of Cortical Acetylcholine Release
SYNAPSE 39:201–212 (2001) Basal Forebrain Glutamatergic Modulation of Cortical Acetylcholine Release JIM FADEL, MARTIN SARTER, AND JOHN P. BRUNO* Departments of Psychology and Neuroscience, The Ohio State University, Columbus, Ohio KEY WORDS acetylcholine; basal forebrain; cortex; microdialysis; glutamate recep- tors; kainate; NMDA ABSTRACT The mediation of cortical ACh release by basal forebrain glutamate receptors was studied in awake rats fitted with microdialysis probes in medial prefrontal cortex and ipsilateral basal forebrain. Repeated presentation of a stimulus consisting of exposure to darkness with the opportunity to consume a sweetened cereal resulted in a transient increase in cortical ACh efflux. This stimulated release was dependent on basal forebrain glutamate receptor activity as intrabasalis perfusion with the ionotropic glutamate receptor antagonist kynurenate (1.0 mM) markedly attenuated darkness/ cereal-induced ACh release. Activation of AMPA/kainate receptors by intrabasalis per- fusion of kainate (100 M) was sufficient to increase cortical ACh efflux even under basal (nonstimulated) conditions. This effect of kainate was blocked by coperfusion with the antagonist DNQX (0.1–5.0 mM). Stimulation of NMDA receptors with intrabasalis perfusion of NMDA (50 or 200 M) did not increase basal cortical ACh efflux. However, perfusion of NMDA in rats following exposure to the darkness/cereal stimulus resulted in a potentiation of both the magnitude and duration of stimulated cortical ACh efflux. Moreover, intrabasalis perfusion of the higher dose of NMDA resulted in a rapid increase in cortical ACh efflux even before presentation of the darkness/cereal stimulus, suggesting an anticipatory change in the excitability of basal forebrain cholinergic neurons. These data demonstrate that basal forebrain glutamate receptors contribute to the stimulation of cortical ACh efflux in response to behavioral stimuli. -

Amygdaloid and Basal Forebrain Direct Connections with the Nucleus of the Solitary Tract and the Dorsal Motor Nucleus
0270~6474/82/0210-1424$02.00/O The Journal of Neuroscience Copyright 0 Society for Neuroscience Vol. 2, No. 10, pp. 1424-1438 Printed in U.S.A. October 1982 AMYGDALOID AND BASAL FOREBRAIN DIRECT CONNECTIONS WITH THE NUCLEUS OF THE SOLITARY TRACT AND THE DORSAL MOTOR NUCLEUS JAMES S. SCHWABER,2 BRUCE S. KAPP,* GERALD A. HIGGINS, AND PETER R. RAPP Departments of Anatomy and Neurobiology and of *Psychology, College of Medicine, University of Vermont, Burlington, Vermont 05405 Received August 3, 1981; Revised May 3, 1982; Accepted May 13, 1982 Abstract Although the amygdala complex has long been known to exert a profound influence on cardiovas- cular activity, the neuronal and connectional substrate mediating these influences remains unclear. This paper describes a direct amygdaloid projection to medullary sensory and motor structures involved in cardiovascular regulation, the nucleus of the solitary tract (NTS) and the dorsal motor nucleus (DVN), by the use of autoradiographic anterograde transport and retrograde horseradish peroxidase (HRP) techniques in rabbits. Since all of these structures are highly heterogeneous structurally and functionally, details of the specific areas of the neuronal origin and efferent distribution of the projection were examined in relation to these features and with reference to a cytoarchitectonic description of the relevant forebrain regions in the rabbit. Amygdaloid projections to the NTS and DVN, as determined from HRP experiments, arise from an extensive population of neurons concentrated exclusively within the ipsilateral central nucleus and confined to and distrib- uted throughout a large medial subdivision of this nucleus. Projection neurons, however, also distribute without apparent interruption beyond the amygdala dorsomedially into the sublenticular substantia innominata and the lateral part of the bed nucleus of the stria terminalis and thus delineate a single entity of possible anatomical unity across all three structures, extending rostro- caudally within the basal forebrain as a diagonal band. -

The Input-Output Relationship of the Cholinergic Basal Forebrain
Resource The Input-Output Relationship of the Cholinergic Basal Forebrain Graphical Abstract Authors Matthew R. Gielow, Laszlo Zaborszky Correspondence [email protected] In Brief Monosynaptic viral tracing in transgenic rats reveals that patterns of input cells contacting cholinergic neurons are biased according to their cortical or amygdalar output. Mapping inputs across the entire brain, Gielow and Zaborszky provide structural evidence for networks enabling differential acetylcholine release. Highlights d Inputs to cholinergic cells are biased, varying by cortical output target d Proportions of input to a given cortical cholinergic output are reproducible d The most prominent input to many cholinergic cells is the caudate putamen d Medial prefrontal cortex-projecting cholinergic cells receive little caudate input Gielow & Zaborszky, 2017, Cell Reports 18, 1817–1830 February 14, 2017 ª 2017 The Author(s). http://dx.doi.org/10.1016/j.celrep.2017.01.060 Cell Reports Resource The Input-Output Relationship of the Cholinergic Basal Forebrain Matthew R. Gielow1 and Laszlo Zaborszky1,2,* 1Center for Molecular and Behavioral Neuroscience, Rutgers, the State University of New Jersey, Newark, NJ 07102, USA 2Lead Contact *Correspondence: [email protected] http://dx.doi.org/10.1016/j.celrep.2017.01.060 SUMMARY Lesions of the BF in experimental animals or humans cause enhancement of slow oscillations and severe attention and mem- Basal forebrain cholinergic neurons influence cortical ory deficits (Botly and De Rosa, 2012; Buzsa´ ki et al., 1988; Lut- state, plasticity, learning, and attention. They collec- kenhoff et al., 2015), while BF stimulation increases the sponta- tively innervate the entire cerebral cortex, differen- neous and visually driven cortical firing rates, improving neuronal tially controlling acetylcholine efflux across different response reliability (Pinto et al., 2013). -

Anatomical Relationship Between the Basal Ganglia and the Basal
Proc. Nati. Acad. Sci. USA Vol. 84, pp. 1408-1412, March 1987 Medical Sciences Anatomical relationship between the basal ganglia and the basal nucleus of Meynert in human and monkey forebrain (enkephalin/acetylcholinesterase/primate/human) SUZANNE HABER Department of Neurobiology and Anatomy, University of Rochester, Rochester, NY 14642 Communicated by Walle J. H. Nauta, October 20, 1986 ABSTRACT Previous immunohistochemical studies have suggestion that the basal ganglia could serve cognitive as well provided evidence that the external segment of the globus as motor functions (7). Because this notion places the basal pallidus extends ventrally beneath the transverse limb of the ganglia in a functional category comparable, in part at least, anterior commissure into the area of the substantia in- to that of the basal nucleus of Meynert, a more detailed nominata. Enkephalin-positive staining in the form of "woolly description ofthe relationship ofthese two structures to each fibers" has been used as a marker for the globus pallidus and other seemed of interest. its ventral extension. Acetylcholinesterase staining of both The globus pallidus (in particular its most ventral part, the fibers and cell bodies, frequently used as a marker for the basal ventral pallidum) and the basal nucleus of Meynert are nucleus of Meynert, is also found in the area of the substantia adjacent structures (Fig. 2 A-C and 3 A and B). The large innominata. This study describes the differential distribution of acetylcholinesterase (AcChoEase)-positive neurons in the enkephalin-positive woolly fibers and acetylcholinesterase substantia innominata (i.e., the infrapallidal region of the staining on adjacent sections in both the monkey and human basal forebrain) are regarded as a characteristic marker for basal forebrain area in an attempt to define the relationship the basal nucleus of Meynert and are therefore considered to between the basal ganglia and the basal nucleus of Meynert. -

Where Dopaminergic and Cholinergic Systems Interact: a Gateway for Tuning Neurodegenerative Disorders
fnbeh-15-661973 July 21, 2021 Time: 11:29 # 1 MINI REVIEW published: 22 July 2021 doi: 10.3389/fnbeh.2021.661973 Where Dopaminergic and Cholinergic Systems Interact: A Gateway for Tuning Neurodegenerative Disorders Marianne Amalric1, Tommy Pattij2, Ioannis Sotiropoulos3,4, Joana M. Silva3,4, Nuno Sousa4, Samira Ztaou1,5, Cristiano Chiamulera6, Lars U. Wahlberg7, Dwaine F. Emerich8 and Giovanna Paolone6* 1 Centre National de la Recherche Scientifique (CNRS), UMR 7291, Laboratoire de Neurosciences Cognitives, Aix-Marseille University (AMU), Marseille, France, 2 Amsterdam Neuroscience, Department of Anatomy and Neurosciences, Amsterdam University Medical Centers, Amsterdam, Netherlands, 3 Life and Health Sciences Research Institute (ICVS), School of Medicine, University of Minho, Braga, Portugal, 4 ICVS/3B’s – PT Government Associate Laboratory, Braga, Portugal, 5 Department of Molecular Therapeutics, New York State Psychiatric Institute, Department of Psychiatry, Columbia University, New York, NY, United States, 6 Department of Diagnostic and Public Health, Section of Pharmacology, University of Verona, Verona, Italy, 7 Gloriana Therapeutics, Inc., Warren, RI, United States, 8 Independent Researcher, Glocester, RI, United States Edited by: Sara Morley-Fletcher, Historically, many investigations into neurodegenerative diseases have focused on Lille University of Science and Technology, France alterations in specific neuronal populations such as, for example, the loss of midbrain Reviewed by: dopaminergic neurons in Parkinson’s disease (PD) and loss of cholinergic transmission Ling Shan, in Alzheimer’s disease (AD). However, it has become increasingly clear that mammalian Netherlands Institute for Neuroscience (KNAW), Netherlands brain activities, from executive and motor functioning to memory and emotional Nicolaas Bohnen, responses, are strictly regulated by the integrity of multiple interdependent neuronal University of Michigan, United States circuits. -

Redalyc.Vascular Dementia and the Cholinergic Pathways
Dementia & Neuropsychologia ISSN: 1980-5764 [email protected] Associação Neurologia Cognitiva e do Comportamento Brasil Engelhardt, Eliasz; Madeira Moreira, Denise; Laks, Jerson Vascular dementia and the cholinergic pathways Dementia & Neuropsychologia, vol. 1, núm. 1, enero-marzo, 2007, pp. 2-9 Associação Neurologia Cognitiva e do Comportamento São Paulo, Brasil Available in: http://www.redalyc.org/articulo.oa?id=339528997005 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Materia 01 07.03.07 16:01 Page 2 Dementia & Neuropsychologia 2007;1:2-9 Vascular dementia and the cholinergic pathways Eliasz Engelhardt1, Denise Madeira Moreira2, Jerson Laks3 Abstract – Vascular cognitive impairment/vascular dementia have been the subject of a large number of stud- ies, due to their high prevalence and broad preventive and compensatory therapeutic potential. The knowledge of the cerebral anatomy correlated to the vascular territories of irrigation enables understanding of clinical manifestations, as well as classification into the several types of syndromic presentations. The central choliner- gic system exercises important neuromodulatory functions on cerebral circuits related to cognitive and behav- ioral integration, as well as on vasomotor control related to cerebral blood flow adjustments. The acquisition of data on the anatomy of the cholinergic pathways, including the localization of the nuclei of the basal prosen- cephalon and the routes of their projections, established an important milestone. The knowledge of the vascu- lar distribution and of the trajectories of the cholinergic pathways allows identification of the strategic points where a vascular lesion can cause interruption. -

Neurogenesis in the Olfactory Tubercle and Islands of Calleja in the Rat
Int. J. Devl. Neuroscience, Vol. 3, No. 2, pp. 135-147, 1985. 0736-5748/85 $03.00+0.00 Printed in Great Britain. Pergamon Press Ltd. © 1985 ISDN NEUROGENESIS IN THE OLFACTORY TUBERCLE AND ISLANDS OF CALLEJA IN THE RAT SHIRLEY A. BAYER Department of Biology, Indiana-Purdue University, 1125 East 38th Street, Indianapolis, IN 46223, U.S.A. (Accepted 26 July 1984) Abstraet--Neurogenesis in the rat olfactory tubercle and islands of Calleja was examined with [3H]thymidine autoradiography. Animals in the prenatal groups were the offspring of pregnant females given an injection of [3H]thymidine on two consecutive gestational days. Ten groups of embryos (E) were exposed to [3H]thymidine on EI2-EI3, E13-EI4 .... E21-E22, respectively. Three groups of postnatal animals (P) were given four consecutive injections of [3H]thymidine on P0-P3, P2-P5, and P4- P7, respectively. On P60, the percentage of labeled cells and the proportion of cells originating during either 24 or 48 h periods were quantified at several anatomical levels. Three populations of neurons were studied: (1) large cells in layer Ill, (2) small to medium-sized cells in layers 11 and Ill, and in the striatal bridges, (3) granule cells in the islands of Calleja. Neurogenesis is sequential between these three popu- lations with No. 1 oldest and No. 3 youngest. The large neurons in layer Ill originate mainly between El3 and El6 in a strong lateral-to-medial gradient. Neurons in population No. 2 are generated between El5 and E20, also in a lateral-to-medial gradient; neurogenesis is simultaneous along the superficial- deep plane. -

Pt 311 Neuroscience
Internal Capsule and Deep Gray Matter Medical Neuroscience | Tutorial Notes Internal Capsule and Deep Gray Matter 1 MAP TO NEUROSCIENCE CORE CONCEPTS NCC1. The brain is the body's most complex organ. NCC3. Genetically determined circuits are the foundation of the nervous system. LEARNING OBJECTIVES After study of the assigned learning materials, the student will: 1. Identify major white matter and gray matter structures that are apparent in sectional views of the forebrain, including the structures listed in the chart and figures in this tutorial. 2. Describe and sketch the relations of the deep gray matter structures to the internal capsule in coronal and axial sections of the forebrain. 3. Describe the distribution of the ventricular spaces in the forebrain and brainstem. NARRATIVE by Leonard E. WHITE and Nell B. CANT Duke Institute for Brain Sciences Department of Neurobiology Duke University School of Medicine Overview Now that you have acquired a framework for understanding the regional anatomy of the human brain, as viewed from the surface, and some understanding of the blood supply to both superficial and deep brain structures, you are ready to explore the internal organization of the brain. This tutorial will focus on the sectional anatomy of the forebrain (recall that the forebrain includes the derivatives of the embryonic prosencephalon). As you will discover, much of our framework for exploring the sectional anatomy of the forebrain is provided by the internal capsule and the deep gray matter, including the basal ganglia and the thalamus. But before beginning to study this internal anatomy, it will be helpful to familiarize yourself with some common conventions that are used to describe the deep structures of the central nervous system. -
Basal Forebrain-Cortical Circuits in Rodents. Implications of Anatomical Pathways and Cell Toxicity in Alzheimer´S Disease
UNIVERSIDAD AUTÓNOMA DE MADRID School of Medicine Anatomy, Histology and Neuroscience Department Basal Forebrain-Cortical circuits in rodents. Implications of anatomical pathways and cell toxicity in Alzheimer´s Disease. Doctoral Thesis Irene Chaves-Coira 2017 1 UNIVERSIDAD AUTÓNOMA DE MADRID Facultad de Medicina Departamento de Anatomía, Histología y Neurociencia Basal Forebrain-Cortical circuits in rodents. Implications of anatomical pathways and cell toxicity in Alzheimer´s Disease. Memory presented by Irene Chaves Coira to qualify for the Doctor's Degree by the Autonomous University of Madrid (UAM) in the Program of Doctorate in Neuroscience, in agreement to the work realized under the direction of the Teachers Margarita Rodrigo Angulo and Ángel Núñez Molina in the Department of Anatomy, Histology and Neuroscience of Medical School of the UAM. Memoria presentada por Irene Chaves Coira para optar al título de Doctor por la Universidad Autónoma de Madrid (UAM) en el Programa de Doctorado en Neurociencia, de acuerdo al trabajo realizado bajo la dirección de los Profesores Margarita Rodrigo Angulo y Ángel Núñez Molina en el Departamento de Anatomía, Histología y Neurociencia de la Facultad de Medicina de la UAM. 2 List of contents 4 LIST OF CONTENTS ABREVIATIONS SUMMARY………………………………………………………………………………………….3 RESUMEN…………………………………………………………………………………………...6 1. INTRODUCTION 1.1. Basal forebrain……………………………………………………………………9 1.2. Acetilcholine………………………………………………………………………..14 1.3. Alzheimer Desease……………………………………………………………....18 1.4. IGF1…………………………………………………………………………………….19 1.5. Cell culture………………………………………………………………………….22 2. HYPOTHESIS AND OBJECTIVES 2.1. Main Hypothesis…………………………………………………………………26 2.2. General and Specific Aims……………………………………………………26 3. MATERIALS AND METHODS 3.1. In vivo procedures……………………………………………………………….30 3.1.1. Biological material used for the experiments………………30 3.1.2.