A Ureteral Mass Presenting As Deep Vein Thrombosis: a Very Rare Presentation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prep for Practical II
Images for Practical II BSC 2086L "Endocrine" A A B C A. Hypothalamus B. Pineal Gland (Body) C. Pituitary Gland "Endocrine" 1.Thyroid 2.Adrenal Gland 3.Pancreas "The Pancreas" "The Adrenal Glands" "The Ovary" "The Testes" Erythrocyte Neutrophil Eosinophil Basophil Lymphocyte Monocyte Platelet Figure 29-3 Photomicrograph of a human blood smear stained with Wright’s stain (765). Eosinophil Lymphocyte Monocyte Platelets Neutrophils Erythrocytes "Blood Typing" "Heart Coronal" 1.Right Atrium 3 4 2.Superior Vena Cava 5 2 3.Aortic Arch 6 4.Pulmonary Trunk 1 5.Left Atrium 12 9 6.Bicuspid Valve 10 7.Interventricular Septum 11 8.Apex of The Heart 9. Chordae tendineae 10.Papillary Muscle 7 11.Tricuspid Valve 12. Fossa Ovalis "Heart Coronal Section" Coronal Section of the Heart to show valves 1. Bicuspid 2. Pulmonary Semilunar 3. Tricuspid 4. Aortic Semilunar 5. Left Ventricle 6. Right Ventricle "Heart Coronal" 1.Pulmonary trunk 2.Right Atrium 3.Tricuspid Valve 4.Pulmonary Semilunar Valve 5.Myocardium 6.Interventricular Septum 7.Trabeculae Carneae 8.Papillary Muscle 9.Chordae Tendineae 10.Bicuspid Valve "Heart Anterior" 1. Brachiocephalic Artery 2. Left Common Carotid Artery 3. Ligamentum Arteriosum 4. Left Coronary Artery 5. Circumflex Artery 6. Great Cardiac Vein 7. Myocardium 8. Apex of The Heart 9. Pericardium (Visceral) 10. Right Coronary Artery 11. Auricle of Right Atrium 12. Pulmonary Trunk 13. Superior Vena Cava 14. Aortic Arch 15. Brachiocephalic vein "Heart Posterolateral" 1. Left Brachiocephalic vein 2. Right Brachiocephalic vein 3. Brachiocephalic Artery 4. Left Common Carotid Artery 5. Left Subclavian Artery 6. Aortic Arch 7. -

Vessels and Circulation
CARDIOVASCULAR SYSTEM OUTLINE 23.1 Anatomy of Blood Vessels 684 23.1a Blood Vessel Tunics 684 23.1b Arteries 685 23.1c Capillaries 688 23 23.1d Veins 689 23.2 Blood Pressure 691 23.3 Systemic Circulation 692 Vessels and 23.3a General Arterial Flow Out of the Heart 693 23.3b General Venous Return to the Heart 693 23.3c Blood Flow Through the Head and Neck 693 23.3d Blood Flow Through the Thoracic and Abdominal Walls 697 23.3e Blood Flow Through the Thoracic Organs 700 Circulation 23.3f Blood Flow Through the Gastrointestinal Tract 701 23.3g Blood Flow Through the Posterior Abdominal Organs, Pelvis, and Perineum 705 23.3h Blood Flow Through the Upper Limb 705 23.3i Blood Flow Through the Lower Limb 709 23.4 Pulmonary Circulation 712 23.5 Review of Heart, Systemic, and Pulmonary Circulation 714 23.6 Aging and the Cardiovascular System 715 23.7 Blood Vessel Development 716 23.7a Artery Development 716 23.7b Vein Development 717 23.7c Comparison of Fetal and Postnatal Circulation 718 MODULE 9: CARDIOVASCULAR SYSTEM mck78097_ch23_683-723.indd 683 2/14/11 4:31 PM 684 Chapter Twenty-Three Vessels and Circulation lood vessels are analogous to highways—they are an efficient larger as they merge and come closer to the heart. The site where B mode of transport for oxygen, carbon dioxide, nutrients, hor- two or more arteries (or two or more veins) converge to supply the mones, and waste products to and from body tissues. The heart is same body region is called an anastomosis (ă-nas ′tō -mō′ sis; pl., the mechanical pump that propels the blood through the vessels. -

Cat Dissection
Cat Dissection Muscular Labs Tibialis anterior External oblique Pectroalis minor Sartorius Gastrocnemius Pectoralis major Levator scapula External oblique Trapezius Gastrocnemius Semitendinosis Trapezius Latissimus dorsi Sartorius Gluteal muscles Biceps femoris Deltoid Trapezius Deltoid Lumbodorsal fascia Sternohyoid Sternomastoid Pectoralis minor Pectoralis major Rectus abdominis Transverse abdominis External oblique External oblique (reflected) Internal oblique Lumbodorsal Deltoid fascia Latissimus dorsi Trapezius Trapezius Trapezius Deltoid Levator scapula Deltoid Trapezius Trapezius Trapezius Latissimus dorsi Flexor carpi radialis Brachioradialis Extensor carpi radialis Flexor carpi ulnaris Biceps brachii Triceps brachii Biceps brachii Flexor carpi radialis Flexor carpi ulnaris Extensor carpi ulnaris Triceps brachii Extensor carpi radialis longus Triceps brachii Deltoid Deltoid Deltoid Trapezius Sartorius Adductor longus Adductor femoris Semimembranosus Vastus Tensor fasciae latae medialis Rectus femoris Vastus lateralis Tibialis anterior Gastrocnemius Flexor digitorum longus Biceps femoris Tensor fasciae latae Semimembranosus Semitendinosus Gluteus medius Gluteus maximus Extensor digitorum longus Gastrocnemius Soleus Fibularis muscles Brachioradiallis Triceps (lateral and long heads) Brachioradialis Biceps brachii Triceps (medial head) Trapezius Deltoid Deltoid Levator scapula Trapezius Deltoid Trapezius Latissimus dorsi External oblique (right side cut and reflected) Rectus abdominis Transversus abdominis Internal oblique Pectoralis -

Surgical Anatomy of the Common Iliac Veins During Para-Aortic and Pelvic Lymphadenectomy for Gynecologic Cancer
Original Article J Gynecol Oncol Vol. 25, No. 1:64-69 http://dx.doi.org/10.3802/jgo.2014.25.1.64 pISSN 2005-0380·eISSN 2005-0399 Surgical anatomy of the common iliac veins during para-aortic and pelvic lymphadenectomy for gynecologic cancer Kazuyoshi Kato, Shinichi Tate, Kyoko Nishikimi, Makio Shozu Department of Gynecology, Chiba University School of Medicine, Chiba, Japan See accompanying editorial by Lee on page 1. Objective: Compression of the left common iliac vein between the right common iliac artery and the vertebrae is known to be associated with the occurrence of left iliofemoral deep vein thrombosis (DVT). In this study, we described the variability in vascular anatomy of the common iliac veins and evaluated the relationship between the degree of iliac vein compression and the presence of DVT using the data from surgeries for gynecologic cancer. Methods: The anatomical variations and the degrees of iliac vein compression were determined in 119 patients who underwent systematic para-aortic and pelvic lymphadenectomy during surgery for primary gynecologic cancer. Their medical records were reviewed with respect to patient-, disease-, and surgery-related data. Results: The degrees of common iliac vein compression were classified into three grades: grade A (n=28, 23.5%), with a calculated percentage of 0%-25% compression; grade B (n=47, 39.5%), with a calculated percentage of 26%-50% compression; and grade C (n=44, 37%), with a calculated percentage of more than 50% compression. Seven patients (5.9%) had common iliac veins with anomalous anatomies; three were divided into small caliber vessels, two with a flattened structure, and two had double inferior vena cavae. -

Co-Existence of the Double Inferior Vena Cava with Complex Interiliac
Folia Morphol. Vol. 77, No. 1, pp. 151–155 DOI: 10.5603/FM.a2017.0074 C A S E R E P O R T Copyright © 2018 Via Medica ISSN 0015–5659 www.fm.viamedica.pl Co-existence of the double inferior vena cava with complex interiliac venous communication and aberrant common hepatic artery arising from superior mesenteric artery: a case report V. Chentanez, N. Nateniyom, T. Huanmanop, S. Agthong Department of Anatomy, Faculty of Medicine, King Chulalongkorn Memorial Hospital, Chulalongkorn University, Bangkok, Thailand [Received: 19 June 2017; Accepted: 31 July 2017] Variations of the arterial and venous system of the abdomen and pelvis have im- portant clinical significance in hepatobiliary surgery, abdominal laparoscopy, and radiological intervention. A case of double inferior vena cava (IVC) with complex interiliac communication and variation of the common hepatic artery (CHA) arising from superior mesenteric artery (SMA) in a 79-year-old male cadaver is presented. Both IVCs ascended on either side of the abdominal aorta. The left-sided IVC crossed anterior to the aorta at the level of the left renal vein. The union of both IVCs was at the level just above the right renal vein. The diameter of right-sided IVC, left-sided IVC and the common IVC were 16.73 mm, 21.57 mm and 28.75 mm, respectively. In the pelvic cavity, the right common iliac vein was formed by a union of right external and internal iliac veins while the formation of left common iliac vein was from the external iliac vein and two internal iliac veins. An interiliac vein ran from right internal iliac vein to left common iliac vein with an additional communicating vein running from the middle of this interiliac vein to the right common iliac vein. -

Pelvic Venous Disorders
PELVIC VENOUS DISORDERS Anatomy and Pathophysiology Two Abdomino-Pelvic Compression Syndromes DIAGNOSIS of ABDOMINOO-PELVICP z Nutcracker Syndrome 9 Compression of the left renal vein COMPRESSIONCO SS O SYNDROMES S O with venous congestion of the left (with Emphasis on Duplex Ultrasound) kidney and left ovarian vein reflux R. Eugene Zierler, M.D. z May-Thurner Syndrome 9 Compression of the left common iliac vein by the right common The DD.. EE.. StrandnessStrandness,, JrJr.. Vascular Laboratory iliac artery with left lower University of Washington Medical Center extremity venous stasis and left DivisionDivision of Vascular Surgery internal iliac vein reflux University of Washington, School of Medicine ABDOMINO-PELVIC COMPRESSION Nutcracker Syndrome Left Renal Vein Entrapment z Grant 1937: Anatomical observation “…the left renal vein, as it lies between the aorta and superior mesenteric artery, resembles a nut between the jaws of a nutcracker.” X z El-Sadr 1950: Described first patient with the clinical syndrome X z De Shepper 1972: Named the disorder “Nutcracker Syndrome” Copy Here z Nutcracker Phenomenon z Nutcracker Syndrome 9 Anatomic finding only 9 Hematuria, proteinuria 9 Compression of left renal 9 Flank pain vein - medial narrowing 9 Pelvic pain/congestion with lateral (hilar) dilation 9 Varicocele ABDOMINO-PELVIC COMPRESSION ABDOMINO-PELVIC COMPRESSION Nutcracker Syndrome - Diagnosis Nutcracker Syndrome z Anterior Nutcracker z Posterior Nutcracker z Evaluate the left renal vein for aorto-mesenteric compression 9 Compression between -

Download Download
EJMED, European Journal of Medical and Health Sciences Vol. 2, No. 4, July 2020 Nonseminomatous Germ Cell Testicular Tumour With Metastatic Retroperitoneal Lymphadenopathy Presenting As Severe Backache Due To Ivc Thrombosis Sanjay M. Khaladkar, Rubab Kaur Sekhon, Khushboo Agrawal, Vikas LB Jadhav, and Rajesh S. Kuber Abstract — IVC thrombosis is often under-recognized. I. CASE REPORT Malignancy can cause spontaneous IVC thrombosis due to its A 26 years old male patient presented with lower back prothrombotic potential. Malignant tumors can compress, adhere or infiltrate the IVC wall causing endothelial damage ache, weight loss and fever. MRI Lumbosacral spine (Fig. 1) with subsequent thrombosis. Retroperitoneal done in an outside center showed a soft tissue signal lymphadenopathy can cause compressive distortion of IVC intensity retroperitoneal mass in aorto-caval region causing venous stasis and turbulent flow. Metastatic compressing IVC- likely lymph nodal mass. retroperitoneal lymphadenopathy from testicular tumor is a rare cause of IVC invasion with resultant IVC thrombosis which can rarely present as backache. High index of suspicion is needed to detect primary testicular tumor in cases of IVC thrombosis, especially in young individuals. A 26 -year old male presented with lower back ache, weight loss and fever. MRI Lumbosacral spine done outside showed a soft tissue signal intensity retroperitoneal mass in aortocaval region compressing IVC. Ultrasound (done outside) revealed mild right sided hydroureteronephrosis secondary to a lobulated heterogeneous mass in inter-aortocaval region encasing right ureter and invading IVC causing thrombosis. Contrast enhanced Computerized axial tomography of abdomen showed a heterogeneously enhancing lobulated mass with multiple internal calcifications, in inter-aortocaval region at L3-4 level invading the IVC causing IVC thrombosis. -
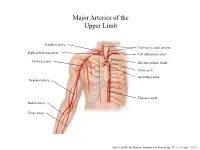
Major Arteries of the Upper Limb
Major Arteries of the Upper Limb Vertebral artery Common carotid arteries Right subclavian artery Left subclavian artery Axillary artery Brachiocephalic trunk Aortic arch Ascending aorta Brachial artery Thoracic aorta Radial artery Ulnar artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.23 Major Arteries of the Abdominal Region Renal artery Celiac trunk Abdominal aorta Superior mesenteric artery Gonadal artery Inferior mesenteric artery Common iliac artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.24 Common iliac artery Internal iliac artery Major Arteries of the External iliac artery Lower Limb Femoral artery Popliteal artery Anterior tibial artery Fibular artery Posterior tibial artery Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.25 Major Veins of the Upper Limb Internal jugular vein (left) Subclavian vein (right) External jugular vein (left) Axillary vein Brachiocephalic veins Cephalic vein Superior vena cava Brachial vein Basilic vein Median cubital vein Inferior vena cava Radial vein Ulnar vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.28 Major Veins of the Abdominal Cavity – Part 1 Hepatic veins Inferior vena cava Renal vein (left) Gonadal vein (left) Gonadal vein (right) Common iliac vein (left) Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Major Veins of the Abdominal Cavity – Part 2 (Hepatic portal circulation) Hepatic portal vein Splenic vein Inferior mesenteric vein Superior mesenteric vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.29 Common iliac vein (left) Internal iliac vein Major Veins of the External iliac vein Lower Limb Great saphenous vein Femoral vein Popliteal vein Fibular vein Small saphenous vein Anterior tibial Posterior tibial vein vein Marieb & Hoehn (Human Anatomy and Physiology, 9th ed.) – Figure 19.30 . -

Sources of Venous Blood Supply of Kidneys in Chicken of Haysex White Breed
M. V. Pervenetskaya et al /J. Pharm. Sci. & Res. Vol. 10(10), 2018, 2639-2641 Sources of Venous Blood Supply of Kidneys in Chicken of Haysex White Breed M. V. Pervenetskaya, L. V. Fomenko, G. A. Honin Omsk State Agrarian University named after P.A. Stolypin, 644008, Omsk, Russian Federation, Institutskaya Square, 1 Abstract: As a result of our studies, it has been found that blood from pelvic extremities in chicken flows along the right and left external iliac veins into the pelvic cavity. The caudal portal vein of the kidney branches from it in the caudal direction - from cranial part of kidneys. The caudal portal vein collects blood from middle and caudal parts of the kidney. The caudal portal vein, slightly bending in the caudomedial direction, joins the caudal portal vein from the opposite side. Coccygeal mesenteric vein branches from junctions of these veins. The right and left renal veins when joining together with an acute angle flow into the common iliac vein, which in turn enters caudal vena cava. Intraorgan veins of the kidney are divided into interlobular, perilobular, intralobular veins and capillaries. Venous blood from kidneys flows by three different ways. The first way is carried out by the hepatic veins from the midst and caudal parts of kidney. Firstly, these veins flow into the common iliac vein, and then into the caudal part of vena cava. The second way of outflow is carried out through the coccygeal mesenteric vein in the liver. The third way is carried out along the right and left cranial anterior portal veins from the anterior part of the kidney into the vertebral venous canal. -

A Case of May-Thurner Syndrome
Open Access Case Report DOI: 10.7759/cureus.10489 A Case of May-Thurner Syndrome Harini Lakshman 1 , Mahmoud Barbarawi 1 , Pal Satyajit Singh Athwal 2 , Michele Obeid 1 , Ghassan Bachuwa 1 1. Internal Medicine, Michigan State University at Hurley Medical Center, Flint, USA 2. Internal Medicine, Saraswathi Institute of Medical Sciences, Hapur, IND Corresponding author: Pal Satyajit Singh Athwal, [email protected] Abstract May-Thurner syndrome, which is also known as iliac vein compression syndrome, is caused when an anatomical variant of the left common iliac vein with a lateral or anterior spur is compressed by the right iliac artery, resulting in thrombosis of the vein. It can present as left deep vein thrombosis which can lead to pulmonary embolism or chronic changes of venous insufficiency in the left lower limb. We report a 27-year- old female with pain abdomen, who was diagnosed to have May-Thurner syndrome. Categories: Internal Medicine, Radiology Keywords: iliac vein thrombosis, may-thurner syndrome Introduction May-Thurner syndrome was first described by May and Thurner in 1957, in which a spur-like projection in the left common iliac vein is compressed by the right common iliac artery [1]. This compression is reportedly associated with intimal hyperplasia and venous stasis, which can be a potential cause of thrombosis [2]. Autopsy data reported this "spur" in more than 20% of the population but is rarely considered in the diagnosis of deep vein thrombosis (DVT) involving iliac veins [1]. The right common iliac artery compresses the left iliac vein against the fifth lumbar vertebrae leading to spur formation and venous thrombosis due to impaired venous return and fulfilling one of Virchow's triad, which is stasis, hypercoagulability state, and endothelial injury. -

A Rare Case of Anatomical Variation of the Femoral Artery and Vein
CASE REPORT Anatomy Journal of Africa. 2020. Vol 9 (2): 1826 - 1830. A RARE CASE OF ANATOMICAL VARIATION OF THE FEMORAL ARTERY AND VEIN Ba B1, Touré T1, Kanté A1, 2, Koné M1, Kouamenou KD1, Koné M1, Guissé F3, Coulibaly T3, Ongoïba N1,2, Koumaré AK1 1) Anatomy laboratory of the Faculty of Medicine and Odontostomatology of Bamako, Mali 2) Surgery Department B of the Point-G University Hospital Center, Bamako, Mali 3) Trauma Department of the Gabriel Touré University Hospital Center, Bamako, Mali Correspondence to Ba Habou Baye dit Babou, Anatomy laboratory of the Faculty of Medicine and Odontostomatology of Bamako, BP : 1805, Email : [email protected] : 66756860/ 76756860 ABSTRACT During a dissection of the two femoral trigons in a female corpse, about 14 years old, we discovered on the right side, the deep artery of the thigh arising from the medial side of the femoral artery and passed in front of the femoral vein above the mouth of the great saphenous vein; on both sides, there was the presence of a collateral canal which communicated the external iliac vein with the femoral vein on the right, on the left, it communicated the external iliac vein with the quadricipital vein. The lower part of the femoral vein was duplicated on both sides, but on the right, there was an interconnecting channel between the two trunks of the duplication. Variations of the femoral vessels are very frequent and can be responsible for an incident during the practice of certain gestures at the level of the femoral trigon such as: catheterization of the femoral artery or vein, the treatment of femoral hernias. -

1. Brachiocephalic Vein 2. External Jugular Vein 3. Internal Jugular Vein 4
Veins 1 Head and Thoracic Veins 1. Given the following veins: 1. brachiocephalic vein 2. external jugular vein 3. internal jugular vein 4. subclavian vein 5. superior vena cava 6. venous sinus Select and arrange the veins in the order blood passes through going. From the brain to the heart From the right (or left) side of the face to the heart. 2. Given the following veins: 1. azygos vein 2. brachiocephalic vein 3. inferior vena cava 4. subclavian vein 5. superior vena cava Select and arrange the veins in the order blood passes through them going. From the RIGHT upper limb to the heart. From the LEFT upper limb to the heart. 1 3. Given the following veins: 1. azygos vein 2. brachiocephalic vein 3. hemiazygos and accessory hemiazygos veins 4. internal thoracic vein 5. subclavian vein 6. superior vena cava Select and arrange the veins in the order blood passes through them going. From the ANTERIOR thoracic wall to the heart. From the LEFT, POSTERIOR thoracic wall to the heart. From the RIGHT, POSTERIOR thoracic wall to the heart. 4. Given the following veins: 1. azygos vein 2. brachiocephalic vein 3. intercostal vein 3. inferior vena cava 5. superior vena cava Select and arrange the veins in the order blood passes through them going from the esophagus to the heart. 5. In one type of heart failure, the RIGHT side of the heart does not pump out enough blood. As a result, blood tends to "backup" in the blood vessels that carry blood to the right side of the heart.