Traumatic Brachial Plexus Injury: a Study of 510 Surgical Cases from Multicenter Services in Guangxi, China
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

15-1117 ) Issued: July 6, 2016 U.S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) T.T., Appellant ) ) and ) Docket No. 15-1117 ) Issued: July 6, 2016 U.S. POSTAL SERVICE, POST OFFICE, ) Philadelphia, PA, Employer ) __________________________________________ ) Appearances: Case Submitted on the Record Michael D. Overman, Esq., for the appellant Office of Solicitor, for the Director DECISION AND ORDER Before: CHRISTOPHER J. GODFREY, Chief Judge PATRICIA H. FITZGERALD, Deputy Chief Judge COLLEEN DUFFY KIKO, Judge JURISDICTION On April 21, 2015 appellant, through counsel, filed a timely appeal of a December 9, 2014 merit decision of the Office of Workers’ Compensation Programs (OWCP). Pursuant to the Federal Employees’ Compensation Act1 (FECA) and 20 C.F.R. §§ 501.2(c)(1) and 501.3, the Board has jurisdiction to consider the merits of the case. ISSUE The issue is whether appellant has met her burden of proof to establish either cervical radiculopathy or a brachial plexus injury, causally related to factors of her federal employment. On appeal counsel alleges that the impartial medical specialist failed to provide sufficient medical reasoning to resolve the existing conflict of medical opinion evidence. 1 5 U.S.C. § 8101 et seq. FACTUAL HISTORY This case has previously been on appeal before the Board.2 The facts and the circumstances outlined in the Board’s prior decision are incorporated herein by reference. The facts relevant to this appeal are set forth below. On March 20, 2008 appellant, then a 44-year-old distribution clerk, filed a timely occupational disease claim (Form CA-2), alleging that she developed neck and shoulder conditions due to repetitive work tasks, commencing June 1, 2006. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Strategies to Improve Nerve Regeneration After Radical Prostatectomy: a Narrative Review
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Institutional Research Information System University of Turin Strategies to improve nerve regeneration after radical prostatectomy: a narrative review Stefano Geuna 1, 2, Luisa Muratori1, 2, Federica Fregnan 1, 2, Matteo Manfredi4 , Riccardo Bertolo 3, 4 , Francesco Porpiglia4. 1 Department of Clinical and Biological Sciences, University of Turin, Orbassano (To), 10043, Italy. 2 Neuroscience Institute Cavalieri Ottolenghi (NICO), Orbassano (To), 10043, Italy. 3 Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, US. 4 Department of Oncology, University of Turin, Orbassano (To), 10043, Italy. Abstract Peripheral nerves are complex organs that spread throughout the entire human body. They are frequently affected by lesions not only as a result of trauma but also following radical tumor resection. In fact, despite the advancement in surgical techniques, such as nerve- sparing robot assisted radical prostatectomy, some degree of nerve injury may occur resulting in erectile dysfunction with significant impairment of the quality of life. The aim of this review is to provide an overview on the mechanisms of the regeneration of injured peripheral nerves and to describe the potential strategies to improve the regeneration process and the functional recovery. Yet, the recent advances in bio- engineering strategies to promote nerve regeneration in the urological field are outlined with a view on the possible future regenerative therapies which might ameliorate the functional outcome after radical prostatectomy. 1 Introduction Radical prostatectomy is the gold standard surgical treatment for organ-confined prostate cancer. The employment of innovative surgical technique such as nerve-sparing robot assisted radical prostatectomy allowed to magnify the anatomical field leading to a three- dimensional perspective obtained through the robotic lenses and a better anatomical knowledge. -

Central Adaptation Following Brachial Plexus Injury
UCSF UC San Francisco Previously Published Works Title Central Adaptation following Brachial Plexus Injury. Permalink https://escholarship.org/uc/item/2ds5z53m Authors Simon, Neil G Franz, Colin K Gupta, Nalin et al. Publication Date 2016 DOI 10.1016/j.wneu.2015.09.027 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Literature Reviews Central Adaptation following Brachial Plexus Injury Neil G. Simon1, Colin K. Franz2,3, Nalin Gupta4, Tord Alden5,6, Michel Kliot6 Key words Brachial plexus trauma (BPT) often affects young patients and may result in - Apraxia lasting functional deficits. Standard care following BPT involves monitoring for - Brachial plexus injury - Central adaptation clinical and electrophysiological evidence of muscle reinnervation, with sur- - Nerve trauma gical treatment decisions based on the presence or absence of spontaneous - Neuroplasticity recovery. Data are emerging to suggest that central and peripheral adaptation may play a role in recovery following BPT. The present review highlights Abbreviations and Acronyms BPT: Brachial plexus trauma adaptive and maladaptive mechanisms of central and peripheral nervous system CIMT: Constraint-induced movement therapy changes following BPT that may contribute to functional outcomes. Rehabili- CNS: Central nervous system tation and other treatment strategies that harness or modulate these intrinsic EMG: Electromyography adaptive mechanisms may improve functional outcomes following BPT. ES: Electrical stimulation H-reflex: Hoffman reflex MRI: Magnetic resonance imaging OBPP: Obstetric brachial plexus palsy PNI: Peripheral nerve injury RECOVERY FROM BPT functional recovery, with no residual def- fi Recovery of nerve tracts following BPT icits identi ed on serial clinician or phys- 1St. Vincent’s Clinical School, University of New South 1 2 relies on a complex cascade of peripheral iotherapist review. -

International Standards for Neurological Classification of Spinal Cord Injury (Revised 2011)
International standards for neurological classification of spinal cord injury (Revised 2011) Steven C. Kirshblum1,2, Stephen P. Burns3, Fin Biering-Sorensen4, William Donovan5, Daniel E. Graves6, Amitabh Jha7, Mark Johansen7, Linda Jones8, Andrei Krassioukov9, M.J. Mulcahey10, Mary Schmidt-Read11, William Waring12 The authors are the members of the International Standards Committee of ASIA. 1UMDNJ/New Jersey Medical School, 2Kessler Institute for Rehabilitation, 3University of Washington School of Medicine, Seattle, Washington, 4Clinic for Spinal Cord Injuries, Rigshospitalet, and Faculty of Health Sciences, University of Copenhagen, Denmark, 5University of Texas, Houston, Texas, 6University of Kentucky, 7Craig Hospital, Englewood, CO, 8Geron Corporation, Menlo Park, CA, USA, 9International Collaboration on Repair Discoveries, Vancouver, British Columbia, Canada, 10Shriners Hospital for Children, 11Magee Rehabilitation Hospital, Philadelphia, PA, 12Medical College of Wisconsin, Milwaukee, Wisconsin Introduction above which they exit (i.e. C1 exits above the C1 vertebra, This article represents the content of the booklet, just below the skull and C6 nerve roots pass between the International Standards for Neurological Classification C5 and C6 vertebrae) whereas C8 exists between the C7 of Spinal Cord Injury, revised 2011, published by the and T1 vertebra; as there is no C8 vertebra. The C1 American Spinal Injury Association (ASIA). For further nerve root does not have a sensory component that is explanation of the clarifications and changes in this tested on the International Standards Examination. revision, see the accompanying article (Kirshblum S., The thoracic spine has 12 distinct nerve roots and the et al. J Spinal Cord Med. 2011:DOI 10.1179/ lumbar spine consists of 5 distinct nerve roots that are 107902611X13186000420242 each named accordingly as they exit below the level of the The spinal cord is the major conduit through which respective vertebrae. -

Neuropathology Category Code List
Neuropathology Page 1 of 27 Neuropathology Major Category Code Headings Revised 10/2018 1 General neuroanatomy, pathology, and staining 65000 2 Developmental neuropathology, NOS 65400 3 Epilepsy 66230 4 Vascular disorders 66300 5 Trauma 66600 6 Infectious/inflammatory disease 66750 7 Demyelinating diseases 67200 8 Complications of systemic disorders 67300 9 Aging and neurodegenerative diseases 68000 10 Prion diseases 68400 11 Neoplasms 68500 12 Skeletal Muscle 69500 13 Peripheral Nerve 69800 14 Ophthalmic pathology 69910 Neuropathology Page 2 of 27 Neuropathology 1 General neuroanatomy, pathology, and staining 65000 A Neuroanatomy, NOS 65010 1 Neocortex 65011 2 White matter 65012 3 Entorhinal cortex/hippocampus 65013 4 Deep (basal) nuclei 65014 5 Brain stem 65015 6 Cerebellum 65016 7 Spinal cord 65017 8 Pituitary 65018 9 Pineal 65019 10 Tracts 65020 11 Vascular supply 65021 12 Notochord 65022 B Cell types 65030 1 Neurons 65031 2 Astrocytes 65032 3 Oligodendroglia 65033 4 Ependyma 65034 5 Microglia and mononuclear cells 65035 6 Choroid plexus 65036 7 Meninges 65037 8 Blood vessels 65038 C Cerebrospinal fluid 65045 D Pathologic responses in neurons and axons 65050 1 Axonal degeneration/spheroid/reaction 65051 2 Central chromatolysis 65052 3 Tract degeneration 65053 4 Swollen/ballooned neurons 65054 5 Trans-synaptic neuronal degeneration 65055 6 Olivary hypertrophy 65056 7 Acute ischemic (hypoxic) cell change 65057 8 Apoptosis 65058 9 Protein aggregation 65059 10 Protein degradation/ubiquitin pathway 65060 E Neuronal nuclear inclusions 65100 -

OIICS Manual 2012
SECTION 2 Definitions, Rules of Selection, and Titles and Descriptions SECTION CONTENTS 2.1 Nature of Injury or Illness 2.2 Part of Body Affected 2.3 Source and Secondary Source of Injury or Illness 2.4 Event or Exposure *-Asterisks denote a summary level code not assigned to individual cases. _____________________________________________________________________________________________ 01/12 6 SECTION 2.1 Nature of Injury or Illness SECTION CONTENTS 2.1.1 Definition, Rules of Selection 2.1.2 Titles and Descriptions *-Asterisks denote a summary level code not assigned to individual cases. _____________________________________________________________________________________________ 01/12 7 2.1.1 Nature of Injury or Illness—Definition, Rules of Selection 1.0 DEFINITION The nature of injury or illness identifies the principal physical characteristic(s) of the work related injury or illness. RULES OF SELECTION: 1.1 Name the injury or illness indicated on the source document. Example: For strained back, choose Strains. 1.2 When two or more injuries or illnesses are indicated, and one is a sequela, aftereffect, complication due to medical treatment, or re-injury, choose the initial injury or illness. Example: If a laceration became infected developing into septicemia, choose Cuts, lacerations. 1.3 When two or more injuries or illnesses are indicated and one is more severe than the other(s) and is not a sequela or complication of the other injury or illness, select the more severe injury or illness. Example: For sprained finger and fractured wrist, choose Fractures. 1.3.1 When a single event or exposure produces an injury and transmits a disease simultaneously, and one is more severe than the other(s), select the more severe injury or disease. -
Brachial Plexus Injury
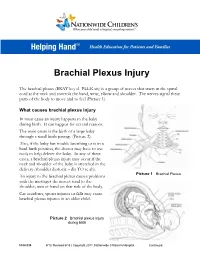
Brachial Plexus Injury The brachial plexus (BRAY key el PLEK sis) is a group of nerves that starts in the spinal cord at the neck and controls the hand, wrist, elbow and shoulder. The nerves signal these parts of the body to move and to feel (Picture 1). What causes brachial plexus injury In most cases an injury happens to the baby during birth. It can happen for several reasons. The main cause is the birth of a large baby through a small birth passage (Picture 2). Also, if the baby has trouble breathing or is in a hard birth position, the doctor may have to use tools to help deliver the baby. In any of these cases, a brachial plexus injury may occur if the neck and shoulder of the baby is stretched in the delivery (shoulder dystocia – dis TO se ah). Picture 1 Brachial Plexus An injury to the brachial plexus causes problems with the messages the nerves send to the shoulder, arm or hand on that side of the body. Car accidents, sports injuries or falls may cause brachial plexus injuries in an older child. Picture 2 Brachial plexus injury during birth HH-I-334 9/13, Revised 6/18 | Copyright 2011, Nationwide Children’s Hospital Continued… Symptoms Your child may have all or only some of the following symptoms on the side of the injury: . Limited or no movement in the shoulder, arm and hand . Muscle weakness or a limp arm . Loss of feeling in the shoulder, arm and hand . Drooping eyelid . Constricted (smaller) pupil in the eye . -

Nerve Transfers for Restoration of Finger Flexion in Patients with Tetraplegia
CLINICAL ARTICLE J Neurosurg Spine 26:55–61, 2017 Nerve transfers for restoration of finger flexion in patients with tetraplegia Jayme A. Bertelli, MD, PhD,1,2 and Marcos F. Ghizoni, MD, MSc2 1Center of Biological and Health Sciences, Department of Neurosurgery, University of the South of Santa Catarina (Unisul), Tubarão; and 2Department of Orthopedic Surgery, Governador Celso Ramos Hospital, Florianópolis, Santa Catarina, Brazil OBJECTIVE The purpose of this paper was to report the authors’ results with finger flexion restoration by nerve transfer in patients with tetraplegia. METHOds Surgery was performed for restoration of finger flexion in 17 upper limbs of 9 patients (8 male and 1 female) at a mean of 7.6 months (SD 4 months) after cervical spinal cord injury. The patients’ mean age at the time of surgery was 28 years (SD 15 years). The motor level according to the ASIA (American Spinal Injury Association) classification was C-5 in 4 upper limbs, C-6 in 10, and C-7 in 3. In 3 upper limbs, the nerve to the brachialis was transferred to the anterior interosseous nerve (AIN), which was sepa- rated from the median nerve from the antecubital fossa to the midarm. In 5 upper limbs, the nerve to the brachialis was transferred to median nerve motor fascicles innervating finger flexion muscles in the midarm. In 4 upper limbs, the nerve to the brachioradialis was transferred to the AIN. In the remaining 5 upper limbs, the nerve to the extensor carpi radialis brevis (ECRB) was transferred to the AIN. Patients were followed for an average of 16 months (SD 6 months). -

Novel Cryoneurolysis Device for the Treatment of Sensory and Motor Peripheral Nerves
UC San Diego UC San Diego Previously Published Works Title Novel cryoneurolysis device for the treatment of sensory and motor peripheral nerves. Permalink https://escholarship.org/uc/item/7s25k7xt Journal Expert review of medical devices, 13(8) ISSN 1743-4440 Authors Ilfeld, Brian M Preciado, Jessica Trescot, Andrea M Publication Date 2016-08-01 DOI 10.1080/17434440.2016.1204229 Peer reviewed eScholarship.org Powered by the California Digital Library University of California EXPERT REVIEW OF MEDICAL DEVICES, 2016 VOL. 13, NO. 8, 713–725 http://dx.doi.org/10.1080/17434440.2016.1204229 REVIEW Novel cryoneurolysis device for the treatment of sensory and motor peripheral nerves Brian M. Ilfelda, Jessica Preciadob and Andrea M. Trescotc aDepartment of Anesthesiology, University California San Diego, San Diego, CA, USA; bMyoscience, Inc., Fremont, CA, USA; cAlaska Pain Management Center, Wasilla, AK, USA ABSTRACT ARTICLE HISTORY Introduction: Cryoneurolysis is the direct application of low temperatures to reversibly ablate periph- Received 5 January 2016 eral nerves to provide pain relief. Recent development of a handheld cryoneurolysis device with small Accepted 17 June 2016 gauge probes and an integrated skin warmer broadens the clinical applications to include treatment of Published online superficial nerves, further enabling treatments for pre-operative pain, post-surgical pain, chronic pain, 13 July 2016 and muscle movement disorders. KEYWORDS Areas covered: Cryoneurolysis is the direct application of cold temperatures to a peripheral nerve, Cryoneurolysis; resulting in reversible ablation due to Wallerian degeneration and nerve regeneration. Use over the last cryoanalgesia; 50 years attests to a very low incidence of complications and adverse effects. -

Bilateral Brachial Plexus Injury Fahim Anwar, Danny Mclaughlin and Bhupinder S
CASE REPORT Bilateral Brachial Plexus Injury Fahim Anwar, Danny McLaughlin and Bhupinder S. Panesar ABSTRACT Brachial plexus injuries can occur as a result of various mechanisms such as stretching, direct and indirect trauma or following childbirth. Bilateral brachial plexus injuries are uncommon and associated with a poor functional outcome. We report a case of bilateral brachial plexus injury resulting from prolonged immobilization of the arms in hyper-abducted position resulting in compression of the brachial plexus on both sides. The injuries were treated conservatively and following 4 months of active rehabilitation in our unit, the patient still had poor arm functions and required care and support in the community on discharge. Key words: Bilateral. Brachial plexus. Injury. Rehabilitation. INTRODUCTION Table I: Summary of neurological findings. Brachial plexus is a network of nerves originating from Medical research council grading of muscle power fifth to seventh cervical (C5-C7) and the first two At admission Following rehabilitation thoracic (T1-T2) spinal nerves. These networks of Right Left Right Left nerves innervate the muscles and skin of the chest, Shoulder abduction 2 1 4 3 Shoulder flexion 0 0 4 3 shoulder, arm and hand. Damage to these nerves Elbow flexion 0 0 0 0 lead to symptoms ranging from a completely paralyzed Elbow extension 0 0 0 0 upper limb to a lack of muscle control in the arm, Wrist flexion 0 0 3 2 wrist or hand and diminished sensations. Injury to the Wrist extension 0 0 0 0 brachial plexus could be the result of trauma to the Finger flexion 1 0 3 2 1 shoulder, traction injury to the spine, inflammation or Finger extension 0 0 0 0 tumour. -
Brachial Plexus Injury Reversing Paralysis & Restoring Function
The Paralysis Center PATIENT GUIDE Brachial Plexus Injury Reversing Paralysis & Restoring Function Justin M. Brown, M.D. Contents 1. Introduction 2. The Anatomy of a Damaged Nerve 3. Assessing Nerve Damage 4. Understanding Brachial Plexus Anatomy 5. Diagnosing Brachial Plexus Injuries - Nerve Conduction & Diagnostic Studies - Diagnostic Testing 6. Understanding Your Treatment Options - Reconstructive Neurosurgery ● Nerve Grafting ● Tendon Transfer ● Muscle Transplant ● Nerve Transfer 7. Why Nerve Transfers are so Successful in Reversing Many Forms of Paralysis - Nerve Transfer as MVP (Most Valuable Player) 8. Post Operative Rehabilitation - Physical and Occupational Therapy 9. But What About …? - Stem Cell Therapy - Robotic Arm 10. Brachial Plexus Patient Stories - Meet Kyle - Meet Diana and Josh 11. Are You a Candidate for Nerve Reconstruction? 12. Tips to Help You Prepare for Your Initial Consult 13. Conclusion 14. About Dr. Brown 15. Contact The Paralysis Center 1 1. Introduction If you are a patient who has suffered injury to your brachial plexus, we are battling against time. Please do not wait to see what kind of function may or may not return following your injury, no matter what you may have been told. More than any other nerve injury, repairing a brachial plexus injury is the most complex and the most time-sensitive of any peripheral nerve injury. We have the greatest chance of restoring maximum function to your arm and hand the faster you can be seen by a Brachial Plexus Specialist - ideally within the first six months following your injury. If this is you, please book a consult immediately with a Brachial Plexus specialist. In 2017, in partnership with Massachusetts General Hospital, Harvard Medical School, and the Spaulding Rehabilitation Hospital, we founded the Paralysis Center - a world-class patient treatment and medical research center for all forms of paralysis.