Mishap Investigation Board Summary of Extravehicular
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Back to the the Future? 07> Probing the Kuiper Belt
SpaceFlight A British Interplanetary Society publication Volume 62 No.7 July 2020 £5.25 SPACE PLANES: back to the the future? 07> Probing the Kuiper Belt 634089 The man behind the ISS 770038 Remembering Dr Fred Singer 9 CONTENTS Features 16 Multiple stations pledge We look at a critical assessment of the way science is conducted at the International Space Station and finds it wanting. 18 The man behind the ISS 16 The Editor reflects on the life of recently Letter from the Editor deceased Jim Beggs, the NASA Administrator for whom the building of the ISS was his We are particularly pleased this supreme achievement. month to have two features which cover the spectrum of 22 Why don’t we just wing it? astronautical activities. Nick Spall Nick Spall FBIS examines the balance between gives us his critical assessment of winged lifting vehicles and semi-ballistic both winged and blunt-body re-entry vehicles for human space capsules, arguing that the former have been flight and Alan Stern reports on his grossly overlooked. research at the very edge of the 26 Parallels with Apollo 18 connected solar system – the Kuiper Belt. David Baker looks beyond the initial return to the We think of the internet and Moon by astronauts and examines the plan for a how it helps us communicate and sustained presence on the lunar surface. stay in touch, especially in these times of difficulty. But the fact that 28 Probing further in the Kuiper Belt in less than a lifetime we have Alan Stern provides another update on the gone from a tiny bleeping ball in pioneering work of New Horizons. -

Air Leak on Space Station 29 September 2020
Russia reports 'non-standard' air leak on Space Station 29 September 2020 manned space programmes, in a televised comment. He said the ISS always has slight air loss due to the air purifying system. "These leaks are predictable. What's happening now is more than the standard leakage and naturally if it lasts a long time, it will require supplies of extra air to the station," he said. He said the crew were now resting but hoped to find the precise spot and fix the leak on Wednesday. Credit: Pixabay/CC0 Public Domain "That's not for sure," he added, saying there was quite a large area to search. "We have time. The leak exists of course. It's not Russia said Tuesday that astronauts had found an good that it's there, but it's not critical," he said. air leak in its section of the International Space Station, with a senior space official calling the air NASA said that the leak had appeared to grow in loss beyond expected levels. size overnight Monday to Tuesday and the crew were awakened by flight controllers to carry out a The crew on the ISS—Russian cosmonauts Anatoly search. Ivanishin and Ivan Vagner and NASA astronaut Christopher Cassidy—have been searching for the It was later found that a temperature change had air leak since August, first checking the US made the leak seem to grow, while the rate of air segment. escaping was "unchanged," the US space agency said. Russia's space agency, Roscosmos, said in a statement that after analysis and a search for the Previously, astronauts had searched for the source leak "it was established that the spot is located in of the leak in the US segment of the station using the Zvezda (star) service module, which contains an ultrasound detector. -

December 2012 Newsletter
December 2012 Inside This Issue: pg: Sierra Lobo’s Headline News 1 Corporate News 2 USAF AFRL ARES III 15 Wolf Tracks NASA AMES Research Center (ARC) 16 NASA Glenn Research Center (GRC) 18 NASA Johnson Space Center (JSC) 20 NASA Kennedy Space Center (KESC) 21 NASA Kennedy Space Center (KISC) 22 NASA Langley Research Center (LaRC) 23 Michoud Assembly Facility (MAF) 25 Redstone Test Center (RTC) 26 Wright-Patterson AFB (WPAFB) 28 Technology Development and Engineering Center (TDEC) 29 Corporate Safety 32 Environmental Issues in T&E 33 Industry News 34 Welcome to the Pack 38 Industry Trivia 40 Sierra Lobo Wins the Engineering Fabrication Services (EFS) Contract at Johnson Space Center (JSC), Absorbs the Wind Tunnel Support Contract on RDSTS, and is Selected for the NASA Space Launch System Advance Development Program. Sierra Lobo (SLI) Primes EFS Win Sierra Lobo Wins SLS Contract The Cryo-Tracker® sensor is a winner of the The Lyndon B. Johnson Space Center, in SLI announces that NASA, Marshall Space R&D 100 Award, recognizing the top 100 ® best new technologies in the world. The Cryo Houston, Texas, NASA’s lead Center for Flight Center, selected our Cryo-Tracker ® human rated spaceflight hardware design and Mass Gauging System for their Space -Tracker sensor proposed for use as SLS’s production, selected Sierra Lobo to “Prime” Launch System (SLS) Advance Development cryogenic liquid-level sensing system is the its EFS Contract. The primary goals of this Program. This selection is part of NASA’s result of more than 16 years of concept contract are to provide JSC organizations and Research Announcement (NRA) to support exploration, validation, and extensive testing external customers the highest quality, cost the evolutionary development strategy for in laboratory and relevant environments. -
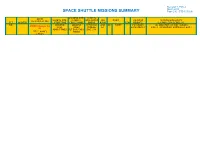
SPACE SHUTTLE MISSIONS SUMMARY Page 210 - STS-127/2JA
Revision T, PCN-4 March 2010 SPACE SHUTTLE MISSIONS SUMMARY Page 210 - STS-127/2JA LANDING SITE/ SSME-TL CREW LAUNCH SITE, RUNWAY, NOM-ABORT SRB ORBIT PAYLOAD MISSION HIGHLIGHTS (6+1 UP/6+1 DN) FLT ORBITER LIFTOFF TIME, CROSSRANGE EMERG RSRM FSW WEIGHTS, (LAUNCH SCRUBS/DELAYS, NO. LANDING LANDING THROTTLE AND INC HA/HP PAYLOADS/ TAL WEATHER, ASCENT I-LOADS, (PCN4 Change Col SITES, TIMES PROFILE ET EXPERIMENTS FIRSTS, SIGNIFICANT ANOMALIES, ETC.) 3) ABORT TIMES FLT DURATION, ENG. S.N. TITLE, NAMES WINDS & EVA'S Revision T, PCN-4 March 2010 SPACE SHUTTLE MISSIONS SUMMARY Page 210 - STS-127/2JA STS- OV-105 CDR: KSC 15 (KSC 104/104/10 BI-138 CARGO: Brief Mission Summary: STS-127 ( 29th (Flight 23) Mark Polansky KSC 39A 71) 9% 51. DIRECT OI- 36253LBS mission to ISS) was a “16 day marathon 127/ 196:22:03:09Z 6 INSERTION 33 ENDEAVO (Flt 3 - STS-98,STS- 212:14:48:07Z RSRM (29) (3) construction mission”. The final pieces of ISS- UR 116) 6:03:10 PM EDT 09:48:07 AM PREDICTED: 106 PAYLOAD the Japanese Kibo Complex including an 2JA P794/R262/V185/M22 (P) CDT 100/104.5/1 POST OMS- CHARGEABLE: Experiment Exposed Facility “Porch” and 8 6:03:10 PM EDT FRIDAY (15) 04.5/ ET-131 2: 24682 LBS the unpressurized Experiment Logistics (A) 123.8x32.3 SEQ OMS PODS 07/31/09 (12 ) 72/104.5 Module were delivered along with spare Wednesday SLWT NM DEPLOYED: FLT # LPO3 -33 PLT equipment intended to keep ISS (15) 35 24266 LBS 127 RPO4 29 Doug Hurley DEORBIT ACTUAL: operational long after Shuttle is retired. -

NASA Assigns STS-127, Expedition 19 Crews 12 February 2008
NASA assigns STS-127, Expedition 19 crews 12 February 2008 The U.S. space agency has assigned the crews for the STS-127 space shuttle mission and the Expedition 19 International Space Station mission. The Endeavour space shuttle's STS-127 mission is to deliver the final components of the Japanese space agency's Kibo laboratory to the space station. Expedition 19 will double the size of the station's resident crew to six people. Mark Polansky will command Endeavour for STS-127, targeted to launch in 2009. Marine Lt. Col. Douglas Hurley will serve as pilot, with astronauts Christopher Cassidy, Thomas Marshburn, David Wolf and Julie Payette, a Canadian Space Agency astronaut, onboard. The mission will deliver U.S. Army Col. Timothy Kopra to the station to join Expedition 18 as a flight engineer and science officer and return Japanese astronaut Koichi Wakata to Earth. Hurley, Cassidy, Marshburn and Kopra will be making their first trips into space. The Japanese module will provide a type of "front porch" for experiments in the exposed space environment. The mission is to include five spacewalks. Expedition 19 will be commanded by cosmonaut and Russian Air Force Col. Gennady Padalka. Copyright 2008 by United Press International APA citation: NASA assigns STS-127, Expedition 19 crews (2008, February 12) retrieved 26 September 2021 from https://phys.org/news/2008-02-nasa-assigns-sts-crews.html This document is subject to copyright. Apart from any fair dealing for the purpose of private study or research, no part may be reproduced without the written permission. The content is provided for information purposes only. -
Appendix Program Managers/Acknowledgments
Flight Information Appendix Program Managers/Acknowledgments Selected Readings Acronyms Contributors’ Biographies Index Image of a Legac y—The Final Re-entry Appendix 517 Flight Information Approx. Orbiter Enterprise STS Flight No. Orbiter Crew Launch Mission Approach and Landing Test Flights and Crew Patch Name Members Date Days 1 Columbia John Young (Cdr) 4/12/1981 2 Robert Crippen (Plt) Captive-Active Flights— High-speed taxi tests that proved the Shuttle Carrier Aircraft, mated to Enterprise, could steer and brake with the Orbiter perched 2 Columbia Joe Engle (Cdr) 11/12/1981 2 on top of the airframe. These fights featured two-man crews. Richard Truly (Plt) Captive-Active Crew Test Mission Flight No. Members Date Length 1 Fred Haise (Cdr) 6/18/1977 55 min 46 s Gordon Fullerton (Plt) 2 Joseph Engle (Cdr) 6/28/1977 62 min 0 s 3 Columbia Jack Lousma (Cdr) 3/22/1982 8 Richard Truly (Plt) Gordon Fullerton (Plt) 3 Fred Haise (Cdr) 7/26/1977 59 min 53 s Gordon Fullerton (Plt) Free Flights— Flights during which Enterprise separated from the Shuttle Carrier Aircraft and landed at the hands of a two-man crew. 4 Columbia Thomas Mattingly (Cdr) 6/27/1982 7 Free Flight No. Crew Test Mission Henry Hartsfield (Plt) Members Date Length 1 Fred Haise (Cdr) 8/12/1977 5 min 21 s Gordon Fullerton (Plt) 5 Columbia Vance Brand (Cdr) 11/11/1982 5 2 Joseph Engle (Cdr) 9/13/1977 5 min 28 s Robert Overmyer (Plt) Richard Truly (Plt) William Lenoir (MS) 3 Fred Haise (Cdr) 9/23/1977 5 min 34 s Joseph Allen (MS) Gordon Fullerton (Plt) 4 Joseph Engle (Cdr) 10/12/1977 2 min 34 s Richard Truly (Plt) 5 Fred Haise (Cdr) 10/26/1977 2 min 1 s 6 Challenger Paul Weitz (Cdr) 4/4/1983 5 Gordon Fullerton (Plt) Karol Bobko (Plt) Story Musgrave (MS) Donald Peterson (MS) The Space Shuttle Numbering System The first nine Space Shuttle flights were numbered in sequence from STS -1 to STS-9. -

2009 Spaceport News Summary
2009 Spaceport News Summary The 2009 Spaceport News used the above banner for the year. The “Spaceport News” portion picked up a bolder look, starting with the July 24, 2009, issue. Introduction The first issue of the Spaceport News was December 13, 1962. The 1963, 1964 and 1965 Spaceport News were issued weekly. The Spaceport News was issued every two weeks, starting July 7, 1966, until the last issue on February 24, 2014. Spaceport Magazine, a monthly issue, superseded the Spaceport News in April 2014, until the final issue, Jan./Feb. 2020. The two 1962 Spaceport News issues and the issues from 1996 until the final Spaceport Magazine issue, are available for viewing at this website. The Spaceport News issues from 1963 through 1995 are currently not available online. In this Summary, black font is original Spaceport News text, blue font is something I added or someone else/some other source provided, and purple font is a hot link. All links were working at the time I completed this Spaceport News Summary. The Spaceport News writer is acknowledged, if noted in the Spaceport News article. Page 1 From The January 9, 2009, Spaceport News On pages 4 and 5, “Scenes Around Kennedy Space Center”. “Space shuttle Endeavour is being lifted away from the Shuttle Carrier Aircraft, or SCA, at Kennedy Space Center’s Shuttle Landing Facility on Dec. 13. The SCA gave the shuttle a piggyback ride from California, where Endeavour landed Nov. 30, ending the STS-126 mission.” On page 7, “747 took on jumbo task 35 years ago”, by Kay Grinter, Reference Librarian. -

Space Reporter's Handbook Mission Supplement
CBS News Space Reporter's Handbook - Mission Supplement Page 1 The CBS News Space Reporter's Handbook Mission Supplement Shuttle Mission STS-127/ISS-2JA: Station Assembly Enters the Home Stretch Written and Produced By William G. Harwood CBS News Space Analyst [email protected] CBS News 6/15/09 Page 2 CBS News Space Reporter's Handbook - Mission Supplement Revision History Editor's Note Mission-specific sections of the Space Reporter's Handbook are posted as flight data becomes available. Readers should check the CBS News "Space Place" web site in the weeks before a launch to download the latest edition: http://www.cbsnews.com/network/news/space/current.html DATE RELEASE NOTES 06/10/09 Initial STS-127 release 06/15/09 Updating to reflect launch delay to 6/17/09 Introduction This document is an outgrowth of my original UPI Space Reporter's Handbook, prepared prior to STS-26 for United Press International and updated for several flights thereafter due to popular demand. The current version is prepared for CBS News. As with the original, the goal here is to provide useful information on U.S. and Russian space flights so reporters and producers will not be forced to rely on government or industry public affairs officers at times when it might be difficult to get timely responses. All of these data are available elsewhere, of course, but not necessarily in one place. The STS-127 version of the CBS News Space Reporter's Handbook was compiled from NASA news releases, JSC flight plans, the Shuttle Flight Data and In-Flight Anomaly List, NASA Public Affairs and the Flight Dynamics office (abort boundaries) at the Johnson Space Center in Houston. -

Reflections 2009 JSC Director
National Aeronautics and Space Administration Lyndon B. Johnson Space Center January | 2010 Reflections 2009 JSC Director year was great for Johnson Space Center, with many Last accomplishments we can all be proud of. You will read about many of them in this special Year in Review issue of Roundup. It highlights our people, our achievements and why JSC is such a great place to work. The Partnership for Public Service and American University’s Institute for the Study of Public Policy Implementation conduct annual surveys that rate the best places to work in the federal government. Based on responses from more than 212,000 federal employees last year, NASA’s workforce continues to score well. The agency is ranked third among large federal agencies as a best place to work. PHOTO The rankings also reveal that NASA scored second among all federal agencies in the categories of effective leadership, teamwork and support for NASA/ diversity, as well as other areas. JSC scored “best in class” in the categories On the cover: of effective leadership and teamwork. None of this is news to any of us here in Houston. We know that we have the The 2009 Year in Review. best workforce in the world, but it is nice to be nationally recognized. As we head into 2010, we can look forward to new challenges and triumphs. We’ll fly out the space shuttle manifest safely. In doing so, we’ll ensure that the International Space Station is fully functional and stocked with spare parts and equipment for the future. On station, we’ll continue to expand science opportunities and document important findings. -

Walking to Olympus: an EVA Chronology, 1997–2011 Volume 2
VOLUME 2 Robert C. Treviño Julie B. Ta MONOGRAPHS AEROSPACE IN HISTORY, 50 NO. AN EVA CHRONOLOGY, 1997–2011 AN CHRONOLOGY, EVA WALKING TO OLYMPUS WALKING WALKING TO OLYMPUS AN EVA CHRONOLOGY, 1997–2011 VOLUME 2 Ta I Treviño NASA SP-2016-4550 WALKING TO OLYMPUS AN EVA CHRONOLOGY, 1997–2011 VOLUME 2 Julie B. Ta Robert C. Treviño MONOGRAPHS IN AEROSPACE HISTORY SERIES #50 APRIL 2016 National Aeronautics and Space Administration NASA History Program Office Public Outreach Division Office of Communications NASA Headquarters Washington, DC 20546 NASA SP-2016-4550 Library of Congress Cataloging-in-Publication Data Ta, Julie B., author. Walking to Olympus: an EVA chronology, 1997–2011 / by Julie B. Ta and Robert C. Treviño. – Second edition. pages cm. – (Monographs in aerospace history series; #50) “April 2016.” Continuation of: Walking to Olympus / David S.F. Portree and Robert C. Treviño. 1997. “NASA SP-2015-4550.” Includes bibliographical references and index. 1. Extravehicular activity (Manned space flight)–History–Chronology. I. Treviño, Robert C., author. II. Title. TL1096.P67 2015 629.45’84–dc23 2015030907 ON THE COVER Astronaut Steve Robinson, anchored to a foot restraint on the International Space Station’s Canadarm2, participates in the STS-114 mission’s third spacewalk. Robinson holds a digital still camera, updated for use on spacewalks, in his left hand. (NASA S114e6651) This publication is available as a free download at http://www.nasa.gov/ebooks. CONTENTS Foreword . v Introduction . .vii The Chronology . 1 1997 1 1998 7 1999 15 2000 21 2001 29 2002 41 2003 55 2004 57 2005 61 2006 67 2007 77 2008 93 2009 107 2010 121 2011 133 Acronyms and Abbreviations . -

+ STS-127 Press Kit (PDF 6.8
CONTENTS Section Page STS-127 MISSION OVERVIEW ................................................................................................ 1 STS-127 TIMELINE OVERVIEW ............................................................................................... 11 MISSION PROFILE................................................................................................................... 15 MISSION OBJECTIVES AND PRIORITIES................................................................................ 17 MISSION PERSONNEL............................................................................................................. 21 STS-127 CREW........................................................................................................................ 23 PAYLOAD OVERVIEW .............................................................................................................. 33 KIBO JAPANESE EXEPRIMENT MODULE EXPOSED FACILITY ................................................................. 33 EXPOSED FACILITY AND EXPERIMENT LOGISTICS MODULE – EXPOSED SECTION................................ 37 INTEGRATED CARGO CARRIER – VERTICAL LIGHT DEPLOY (ICC-VLD) ................................................ 65 RENDEZVOUS & DOCKING....................................................................................................... 69 SPACEWALKS ......................................................................................................................... 73 EXPERIMENTS........................................................................................................................ -

NASA Still Perplexed by Astronaut's Flooded Helmet (Update) 17 July 2013, by Marcia Dunn
NASA still perplexed by astronaut's flooded helmet (Update) 17 July 2013, by Marcia Dunn Luca Parmitano's spacesuit, said NASA spokesman Kelly Humphries. Parmitano, Italy's first and only spacewalker, could not hear or speak by the time he re-entered the space station on Tuesday, 1½ hours after stepping out. He also had difficulty seeing because of the big globs of water in his helmet and elsewhere in his suit. He'd worn the same suit on a spacewalk a week earlier, without mishap. NASA aborted the second spacewalk because of the deluge and later acknowledged it was a serious situation in which Parmitano could have choked or even drowned. He looked all right, although wet, In this image from video made available by NASA, when his crewmates pulled off his helmet, and was astronaut Karen Nyberg assists astronaut Luca Parmitano remove his space suit after the aborted reported to be in fine shape. spacewalk aboard the International Space Station on Tuesday, July 16, 2013. A dangerous water leak in the "Back to normality on the ISS - Cupola is still a helmet of Parmitano, drenched his eyes, nose and fantastic sight, even after a (very short) EVA," mouth, preventing him from hearing or speaking as what Parmitano wrote Wednesday in a tweet. EVA is should have been a routine spacewalk came to an NASA shorthand for spacewalk: extravehicular abrupt end. (AP Photo/NASA) activity. He followed with photos of Italy's Lake Como, the Italian Alps and the Rimini sea resort that he snapped from the station's cupola, or observation deck.