Operator Dies After Being Caught Between Bulldozer's Track and Fender
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
DAO Level 3 Certificate in Military Engineering (Armoured) Titan and Trojan Crew Supervision
Qualification Handbook DAO Level 3 Certificate in Military Engineering (Armoured) Titan and Trojan crew supervision QN: 603/3232/3 The Qualification Overall Objective for the Qualifications This handbook relates to the following qualification: DAO Level 3 Certificate in Military Engineering (Armoured) Titan and Trojan crew supervision Pre-entry Requirements Learners are required to have completed the Class ME (Armd) Class 0-2 course, must be fully qualified AFV crewman and hold full category H driving licence Unit Content and Rules of Combination This qualification is made up of a total of 6 mandatory units and no optional units. To be awarded this qualification the candidate must achieve a total of 13 credits as shown in the table below. Unit Unit of assessment Level GLH TQT Credit number value L/617/0309 Supervise Titan Operation and 3 25 30 3 associated Equipment L/617/0312 Supervise Titan Crew 3 16 19 2 R/617/0313 Supervise Trojan Operation and 3 26 30 3 associated Equipment D/617/0315 Supervise Trojan Crew 3 16 19 2 H/617/0316 Supervise Trojan and Titan AFV 3 10 19 2 maintenance tasks K/617/0317 Carry out emergency procedures and 3 7 11 1 communication for Trojan and Titan AFV Totals 100 128 13 Age Restriction This qualification is available to learners aged 18 years and over. Opportunities for Progression This qualification creates a number of opportunities for progression through career development and promotion. Exemption No exemptions have been identified. 2 Credit Transfer Credits from identical RQF units that have already been achieved by the learner may be transferred. -

NSIAD-88-77 Army Disposal
United States General Accounting Office Report to the Chairman, Subcommittee on GAO>; Oversight and Investigations, Committee on Energy and Commerce, House of Representatives September 1988 ARMYDISPOSAL Construction Equipment Prematurely Disposed of in Europe RESTRKTED-Not to be released outside the Gend Accounting Office except on the basis of the specifk 8~4 by the Of&e of CongressionalRelations. United States General Accounting Office GAO Washington, D.C. 20548 National Security and International Affairs Division B-229358 September 20,1988 The Honorable John Dingell Chairman, Subcommittee on Oversight and Investigations Committee on Energy and Commerce House of Representatives Dear Mr. Chairman: The Army, having decided that its fleet of construction vehicles was becoming too costly to keep in repair, directed European units in 1985 to dispose of commercially available combat engineer construction vehi- cles. The Army purchased 850 replacement vehicles for Europe costing about $79 million. The purchase was part of a worldwide replacement program totaling about $470 million through fiscal year 1987. As you requested, we reviewed the Army’s replacement of construction vehicles in Europe. Our objective was to determine the basis for replac- ing these vehicles. We agree with the Army’s goal to replace worn-out vehicles with stan- dardized ones, but question its decision to dispose of usable vehicles without showing that it was cost-effective to do so. Army officials stated that old construction vehicles were difficult to support and that high repair costs made replacing the entire fleet -regardless of condi- tion-cost-effective. We found no analyses to support the Army’s position. -

Construction Sector Technical Education and Skills
TRAINING REGULATIONS Heavy Equipment Operation (Bulldozer) NC II CONSTRUCTION SECTOR TECHNICAL EDUCATION AND SKILLS DEVELOPMENT AUTHOR ITY East Service Road, South Superhighway, Taguig City, Metro Manila BULLDOZER TR HEAVY - EQUIPMENT OPERATION (Bulldozer) Promulgated July 2007 TABLE OF CONTENTS CONSTRUCTION - HEAVY EQUIPMENT SUB - SECTOR HEAVY EQUIPMENT OPERATION (BULLDOZER) NC II SECTION 1 HEAVY EQUIPMENT OPERATION QUALIFICATION SECTION 2 COMPETENCY STANDARDS SECTION 3 TRAINING STANDARDS 3.1 Curriculum Design 3. 2 Training Delivery 3.3 Trainee Entry Requirements 3.4 List of Tools, Equipment and Materials 3.5 Training Facilities 3.6 Trainers' Qualifications SECTION 4 ASSESSMENT AND CERTIFICATION ARRANGEMENT COMPETENCY MAP DEFINITION OF TERMS ACKNOWLEDGEMEN TS TR HEAVY - EQUIPMENT OPERATION (Bulldozer) Promulgated July 2007 TRAINING REGULATIONS FOR HEAVY EQUIPMENT OPERATION - BULLDOZER SECTION 1 HEAVY EQUIPMENT OPERATION - BULLDOZER The HEAVY EQUIPMENT OPERATION (BULLDOZER) NC II qualification consists of competencies that workers must achieve to enable them to perform tasks such as excavating, dozing, ripping, winching, and clearing of earth materials in construction sites or other locations. This qualification is packaged from the competency map of Construction - Heavy Equipment sub - sector as shown in Annex A. The units of competency comprising this qualification include the following: CODE NO. BASIC COMPETENCIES Units of Competency 500311105 Participate in workplace communication 500311106 Work in a team environment 500311107 Practice career professionalism 500311108 Practice occupational health and safety procedures CODE NO. COMMON COMPETENCIES Units of Competency CON931201 Prepare construction materials and tools CON311201 Observe procedures, specifications and manuals of inst ruction CON311202 Interpret technical drawings and plans CON311203 Perform mensurations and calculations CON311204 Maintain tools and equipment CODE NO. -

United Nations Peacekeeping Missions Military Engineers Manual
United Nations Peacekeeping Missions Military Engineer Unit Manual September 2015 0 Preface We are delighted to introduce the United Nations Peacekeeping Missions Military Unit Manual on Engineers—an essential guide for commanders and staff deployed in peacekeeping operations, and an important reference for Member States and the staff at United Nations Headquarters. For several decades, United Nations peacekeeping has evolved significantly in its complexity. The spectrum of multi-dimensional UN peacekeeping includes challenging tasks such as helping to restore state authority, protecting civilians and disarming, demobilizing and reintegrating ex-combatants. In today’s context, peacekeeping Missions are deploying into environments where they can expect to confront asymmetric threats from armed groups over large swaths of territory. Consequently, the capabilities required for successful peacekeeping Missions demand ever-greater improvement. UN peacekeeping operations are rarely limited to one type of activity. While deployed in the context of a political framework supporting a peace agreement, or in the context of creating the conditions for a return to stability, peacekeeping Missions may require military units to perform challenging tasks involving the judicious use of force, particularly in situations where the host state is unable to provide security and maintain public order. To meet these complex peacekeeping challenges, military components often play a pivotal role in providing and maintaining a secure environment. Under these circumstances, the deployment of UN Military Engineers can contribute decisively towards successful achievement of the Mission’s goals by providing the physical wherewithal to exist, sustain and fulfill its mandate. As the UN continues its efforts to broaden the base of Troop Contributing Countries, and in order to ensure the effective interoperability of all UN Military Engineer Units, there is a need to formalize capability standards. -

The Success of the Light Armoured Vehicle
Canadian Military History Volume 20 Issue 3 Article 9 2011 The Success of the Light Armoured Vehicle Ed Storey Canadian Expeditionary Forces Follow this and additional works at: https://scholars.wlu.ca/cmh Recommended Citation Storey, Ed "The Success of the Light Armoured Vehicle." Canadian Military History 20, 3 (2011) This Feature is brought to you for free and open access by Scholars Commons @ Laurier. It has been accepted for inclusion in Canadian Military History by an authorized editor of Scholars Commons @ Laurier. For more information, please contact [email protected]. Storey: Light Armoured Vehicle The Success of the Light Armoured Vehicle Ed Storey s a military vehicle enthusiast make them cost effective and easier AI was quite excited to see the Abstract: In order to understand the to deploy. article by Frank Maas in Canadian purchase of military vehicles, one must The AVGP series of vehicles Military History dealing with the understand the vehicle and where it falls purchased by Canada in 1976 was in the evolution of vehicle procurement. Canadian Light Armoured Vehicle This article, written in response to an a 10.7 ton, 6 wheeled amphibious (LAV) series of vehicles (vol.20, earlier article in Canadian Military vehicle based on the Swiss Mowag no.2 Spring 2011). I was also keenly History by Frank Maas, examines the Piranha I. Canada bought three interested in the article as my Father chronology and motivations behind versions: the Cougar 76 mm Fire was stationed at CFB Petawawa in the Canadian acquisition of wheeled Support Vehicle, the Grizzly armoured fighting vehicles. -
Working Everyday As a Bulldozer and Excavator Owner/Operator Is Tough
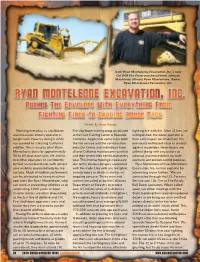
(Left) Ryan Monteleone Excavation, Inc.’s new Cat D6R Fire Dozer purchased from Johnson Machinery. (Above) Ryan Monteleone, Owner, Ryan Monteleone Excavation, Inc. Written By: Brian Hoover Working everyday as a bulldozer Fire’s bulldozer training program located fighting fire with fire. After all fires are and excavator owner/operator is at the Clark Training Center in Riverside, extinguished, the dozer operator is tough work. Now try doing it while California. Applicants come from both then called upon to rehabilitate the surrounded by a blazing California the fire service and the construction previously bulldozed areas to protect wildfire. This is exactly what Ryan industry. Crews and individuals from against mudslides. Here dozers are Monteleone does for approximately all over California must become certified utilized along with excavators to 30 to 60 days each year. He and his and then renew their certification every cleanup and move debris for both two other operators sit confidently year. This intense training is necessary cosmetic and erosion control purposes. behind an enclosed cab, with almost due to the obvious dangers associated Ryan Monteleone of Ryan Monteleone zero visibility, protected only by fire with this trade. Like with any firefighter, Excavation, Inc. further explains his curtains. Much of wildfire confinement serious injury or death is always an interesting niche further, “We are can be attributed to heavy machine ongoing concern. These men and contracted through the U.S. Forestry operators like Ryan Monteleone, who women are called on by the California Service and CAL Fire as Fire Ready can work at preventing wildfires at an Department of Forestry to protect Bull Dozer operators. -
No Slide Title
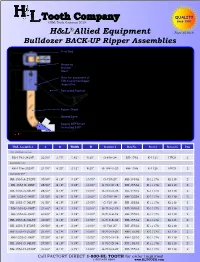
QUALITY ©H&L Tooth Company 2019 since 1931 ® H&L Allied Equipment Flyer 35.2019 Bulldozer BACK-UP Ripper Assemblies Pivot Rod H&L Back-up Rippers are mounted to the back of the bulldozer blade and are designed to rip while the dozer is backing. C Production is increased since the equipment is working full time B in both directions. Tight material, such as hardpan, D.G. and Mounting rock is broken up making production easier with less wear and Bracket tear to the machine. (Box) Rippers operate independently! As the tractor moves forward, Hole for placement of the ripper shanks drag freely behind the dozer blade and when D PIN to position Ripper the tractor moves rearward, each shank will fall into the ripping inoperative position. When shanks needs to be inoperative, simply raise the Retracted Position shank assembly and insert a pin or bolt in the bracket as shown in the drawing detail. H&L replaceable digging Teeth are Uniforged®. Back-up ripper A shanks are designed to install on All-Makes of dozers but were designed specifically for Caterpillar dozers. H&L assemblies Ripper Shank will consist of the mounting bracket (Box), an alloy and hardened steel pivot rod, two cotter pins, ripper shanks, Tooth, Ground Level Flexpin®. The bracket has retract position hole for a pin or bolt. Ripping DEPTH not Mounting instructions: when mounting and welding the to exceed 8.00” bracket to the moldboard of the dozer blade, care should be taken to align it so the shanks will dig in-line with the tracks of the tractor. -

Item 156 Bulldozer Work
156 Item 156 Bulldozer Work 1. DESCRIPTION Excavate, remove, use, or dispose of materials with a bulldozer. Construct, shape, and finish earthwork in conformity with the required lines, grades, and typical cross-sections as shown on the plans, or as directed. 2. EQUIPMENT Use a tractor, crawler, or rubber tired type with a blade attachment at least 8 ft. long. Use a scarifier or ripper with the required tractor when necessary. Use equipment of the type specified on the plans, meeting the following requirements: 2.1. Type A. Manufacturer’s rated net flywheel power of less than 150 horsepower based on SAE standard J1349. 2.2. Type B. Manufacturer’s rated net flywheel power of 150 or greater horsepower based on SAE standard J1349. 3. CONSTRUCTION Perform bulldozer work on the areas as specified on the plans, utilizing equipment as specified above. Rough in with bulldozer work where plans designate “Bulldozer Work” and “Blading,” or “Road Grader Work,” within the same limits. Finish in accordance with specifications for “Blading” or “Road Grader Work.” Compact embankment to ordinary compaction in accordance with Item 132, “Embankment,” unless otherwise shown on the plans. 4. MEASUREMENT This Item will be measured by the actual number of hours of use of the specified type of equipment operated. 5. PAYMENT The work performed in accordance with this Item and measured as provided under “Measurement” will be paid for at the unit price bid for “Bulldozer Work.” This price is full compensation for furnishing and operating equipment, labor, materials, tools, and incidentals. “Sprinkling” and “Rolling” will not be paid for directly but will be subsidiary to this Item. -

Noise Level Analysis of a Bulldozer Used in Constructing a Forest Road in Mediterranean Region of Turkey
African Journal of Agricultural Research Vol. 5(19), pp. 2624-2628, 4 October, 2010 Available online at http://www.academicjournals.org/AJAR ISSN 1991-637X ©2010 Academic Journals Full Length Research Paper Noise level analysis of a bulldozer used in constructing a forest road in Mediterranean region of Turkey Hasan Serin* and Abdullah E. Akay Faculty of Forestry, Kahramanmara Sütçü mam University, 46060 Kahramanmaras, Turkey. Accepted 20 April, 2010 Heavy machinery utilized in forest operations, as one of the working environments with intensive noise disturbance, result detrimental effects on the workers’ health. Particularly, high level noise generated from the road construction machines causes physiologic and psychological health problems on the operators. Among these problems, one of the most important occupational problems is hearing impairment or permanent hearing loss. In this study, the average and peak noise levels generated by a CAT D7G model bulldozer during two working stages (that is, unloaded running stage and road construction stage) of a road construction activity were measured from the operator cabin. The results indicated that the average noise levels for unloaded running stage and road construction stage were 73.87 and 84.11 dBA, respectively. The peak noise levels were measured as 95.90 and 113.40 dBA for unloaded running stage and road construction stage, respectively. Thus, it was found that the mean values of the average noise levels in both working stages were less than the warning limit of 85 dBA. The results also indicated that all of the peak noise levels were over the hazard limit of 90 dBA for both stages. -

Development of Pc210lci-10/Pc200i-10 Machine Control Hydraulic Excavator
Technical Paper Development of PC210LCi-10/PC200i-10 Machine Control Hydraulic Excavator Yuki Shimano Yoshiki Kami Kenichirou Shimokaze In recent years, the efficient construction work thanks to the computerized construction utilizing the ICT technology has been expanded in the market, which contains shortening of a construction period by abolishing the finishing stake which was necessary in the conventional construction work, improvement of execution accuracy, and execution progress management. From this trend, there are growing needs for construction machinery responding to it. When it comes to hydraulic excavators, machines installed with Machine Guidance (MG) have been commercialized including after-market products. However, finishing grading was somewhat dependent on skills of operators monitoring the display. Accordingly, we have developed the machine-controlled hydraulic excavator highly improved in construction efficiency, which enables machine control in a series of operations from rough digging to grading, thanks to the combination of the hydraulic control technology from Komatsu unique components and the GNSS surveying technology. This excavator has released on the computerized-construction-advanced markets of Japan, U.S. and Europe ahead of other competitors. Key Words: PC210LCi-10/PC200i-10, Machine Control Hydraulic Excavator, Automatic Grading Assist, Automatic Stop Control, ICT Construction, Construction Management, GNSS perform work at a construction site without finishing stake 1. Introduction according to the guidance while looking at the guidance monitor. Therefore, final finishing accuracy was largely Construction machinery utilizing GNSS surveying dependent on the skill of operator. technology contributes greatly to the reduction in man-hours We have developed an innovative 20-ton class MC through abolishing of finishing stake. -

Earthmoving Construction Automation with Military Applications: Past, Present and Future
35th International Symposium on Automation and Robotics in Construction (ISARC 2018) Earthmoving Construction Automation with Military Applications: Past, Present and Future Q.P. Haa, L. Yenb, and C. Balaguerc a Faculty of Engineering and IT, University of Technology Sydney, NSW 2007, Australia b Land Vehicles & Systems, Defence Science & Technology Group, SA 5111, Australia c Robotics Lab, Universidad Carlos III de Madrid, Spain E-mail: { [email protected] ; [email protected]; [email protected] } Abstract – Amongst increasing innovations in autonomy of construction plant, in both civilian and frontier engineering sciences, the advancements in military domains, to improve their efficiency, Robotic and Autonomous Systems (RAS) has productivity, quality and reliability [7]. brought about a new horizon in construction Robotic and autonomous systems tailored for the applications. There is evidence of the increasing military call upon the ability to integrate sensors, vision interest in RAS technologies in the civil construction imaging, actuators, end-effector manipulation, computer sector being reflected in construction efforts of many control and human interface for operations in military forces. In particular, Army or ground-based unstructured, difficult and hazardous conditions. Army forces are frequently called upon to conduct construction tasks for enhancing force protection construction tasks as part of military operations, include such earthmoving tasks as filling of protective tasks which could be partially or fully aided by the barriers (HESCO baskets), building dirt bunding employment of RAS technologies. Along with recent structures, as well as anti-tank ditches and trenching. advances in the Internet of Things (IoT) and cyber- For such tasks a variety of heavy construction physical system infrastructure, it is essential to machinery such as excavators, bulldozers, wheel loaders, examine the current maturity, technical feasibility, graders and articulated dump trucks etc. -

Resume PL Word 2.Pages
Hunner Moody 2661 North Goshen Rd, Goshen AL, 36035 334-372-6504 [email protected] Education: 1) Luverne High School • High School Diploma • Graduated 2010 2) Enterprise-Ozark Community College/Alabama Aviation Center • Airframe Technology Certificate • Graduated 2011 • Sheet Metal Experience • Knowledge of sheet metal tools such as: shears, brakes, slip rollers, rivet guns, and counter- sinks. • Experience reading and interpreting electrical diagrams. • Experience using calibrated measuring tools such as: calipers and depth guages. • Experience working with and forming aircraft fuel lines. • Experience assembling and rigging control cables for aircraft control systems. • Experience locating weight and center of gravity for loaded and unloaded aircraft. • Knowledge of aircraft brake systems. • Knowledge of aircraft hydraulic systems. Work Experience: 1) Troy Construction. 03/2020-07/2020 • Operator of heavy machinery such as Excavator, Bulldozer, Backhoe, etc. • Experience using safety equipment such as: safety glasses, gloves, and respirator. • Responsible for keeping all paperwork and documents recorded properly. • Participates in daily Job Safety Assessment meetings. • Participates in monthly company-wide Safety meetings. • Experience maintaining machinery such as: greasing when needed, adding oil or antifreeze, minor repairs, etc. • Experience reading and interpreting Right of Way drawing. • Very common to be away from home for months at a time. 2) Absolute Pipeline Integrity. 11/2018-09/2019 • Operator of heavy machinery such as Excavator, Bulldozer, Backhoe, etc. • Experience using safety equipment such as: safety glasses, gloves, and respirator. • Responsible for keeping all paperwork and documents recorded properly. • Participates in daily Job Safety Assessment meetings. • Participates in monthly company-wide Safety meetings. • Experience maintaining machinery such as: greasing when needed, adding oil or antifreeze, minor repairs, etc.