Selective Androgen Receptor Modulators: Current Knowledge and Clinical Applications
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
WADA Technical Letter – TL07 ANDARINE
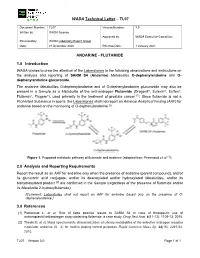
WADA Technical Letter – TL07 Document Number: TL07 Version Number: 3.0 Written by: WADA Science Approved by: WADA Executive Committee Reviewed by: WADA Laboratory Expert Group Date: 21 December 2020 Effective Date: 1 January 2021 ANDARINE - FLUTAMIDE 1.0 Introduction WADA wishes to draw the attention of the Laboratories to the following observations and instructions on the analysis and reporting of SARM S4 (Andarine) Metabolites O-dephenylandarine and O- dephenylandarine glucuronide. The andarine Metabolites O-dephenylandarine and of O-dephenylandarine glucuronide may also be present in a Sample as a Metabolite of the anti-androgen Flutamide (Drogenil®, Eulexin®, Euflex®, Flutamin®, Flugere®), used primarily in the treatment of prostate cancer [1]. Since flutamide is not a Prohibited Substance in sports, the Laboratories shall not report an Adverse Analytical Finding (AAF) for andarine based on the monitoring of O-dephenylandarine [2]. Figure 1. Proposed metabolic pathway of flutamide and andarine (adapted from Perrenoud et al. [1]). 2.0 Analysis and Reporting Requirements Report the result as an AAF for andarine only when the presence of andarine (parent compound), and/or its glucuronic acid conjugate, and/or its deacetylated and/or hydroxylated Metabolites, and/or its bishydroxylated product [2] are confirmed in the Sample (regardless of the presence of flutamide and/or its Metabolite 2-hydroxyflutamide); [Comment: Laboratories shall not report an AAF for andarine based only on the presence of O- dephenylandarine.] 3.0 References [1] Perrenoud L. et al. Risk of false positive results to SARM S4 in case of therapeutic use of antineoplastic/antiandrogen drug containing flutamide: a case study. -

The 2021 List of Pharmacological Classes of Doping Agents and Doping Methods
BGBl. III - Ausgegeben am 8. Jänner 2021 - Nr. 1 1 von 23 The 2021 list of pharmacological classes of doping agents and doping methods www.ris.bka.gv.at BGBl. III - Ausgegeben am 8. Jänner 2021 - Nr. 1 2 von 23 www.ris.bka.gv.at BGBl. III - Ausgegeben am 8. Jänner 2021 - Nr. 1 3 von 23 THE 2021 PROHIBITED LIST WORLD ANTI-DOPING CODE DATE OF ENTRY INTO FORCE 1 January 2021 Introduction The Prohibited List is a mandatory International Standard as part of the World Anti-Doping Program. The List is updated annually following an extensive consultation process facilitated by WADA. The effective date of the List is 1 January 2021. The official text of the Prohibited List shall be maintained by WADA and shall be published in English and French. In the event of any conflict between the English and French versions, the English version shall prevail. Below are some terms used in this List of Prohibited Substances and Prohibited Methods. Prohibited In-Competition Subject to a different period having been approved by WADA for a given sport, the In- Competition period shall in principle be the period commencing just before midnight (at 11:59 p.m.) on the day before a Competition in which the Athlete is scheduled to participate until the end of the Competition and the Sample collection process. Prohibited at all times This means that the substance or method is prohibited In- and Out-of-Competition as defined in the Code. Specified and non-Specified As per Article 4.2.2 of the World Anti-Doping Code, “for purposes of the application of Article 10, all Prohibited Substances shall be Specified Substances except as identified on the Prohibited List. -

Androgen Receptor: a Complex Therapeutic Target for Breast Cancer
cancers Review Androgen Receptor: A Complex Therapeutic Target for Breast Cancer Ramesh Narayanan 1 and James T. Dalton 2,* 1 Department of Medicine, University of Tennessee Health Science Center, Memphis, TN 38103, USA; [email protected] 2 College of Pharmacy, University of Michigan, Ann Arbor, MI 48109, USA * Correspondence: [email protected] Academic Editor: Emmanuel S. Antonarakis Received: 28 September 2016; Accepted: 23 November 2016; Published: 2 December 2016 Abstract: Molecular and histopathological profiling have classified breast cancer into multiple sub-types empowering precision treatment. Although estrogen receptor (ER) and human epidermal growth factor receptor (HER2) are the mainstay therapeutic targets in breast cancer, the androgen receptor (AR) is evolving as a molecular target for cancers that have developed resistance to conventional treatments. The high expression of AR in breast cancer and recent discovery and development of new nonsteroidal drugs targeting the AR provide a strong rationale for exploring it again as a therapeutic target in this disease. Ironically, both nonsteroidal agonists and antagonists for the AR are undergoing clinical trials, making AR a complicated target to understand in breast cancer. This review provides a detailed account of AR’s therapeutic role in breast cancer. Keywords: androgen receptor; breast cancer; selective androgen receptor modulator (SARM); estrogen receptor; triple-negative breast cancer (TNBC) 1. Introduction Over 240,000 women will develop breast cancer and ~40,000 will die from the disease in the United States in 2016 [1]. Globally, about 1.7 million women were diagnosed with breast cancer in 2012, emphasizing the urgent need for effective and safe therapeutic approaches [2]. -

Prnu-BICALUTAMIDE
PRODUCT MONOGRAPH PrNU-BICALUTAMIDE Bicalutamide Tablets, 50 mg Non-Steroidal Antiandrogen NU-PHARM INC. DATE OF PREPARATION: 50 Mural Street, Units 1 & 2 October 16, 2009 Richmond Hill, Ontario L4B 1E4 Control#: 133521 Page 1 of 27 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION....................................................... 3 SUMMARY PRODUCT INFORMATION ............................................................................. 3 INDICATIONS AND CLINICAL USE ................................................................................... 3 CONTRAINDICATIONS ........................................................................................................ 3 WARNINGS AND PRECAUTIONS....................................................................................... 4 ADVERSE REACTIONS......................................................................................................... 5 DRUG INTERACTIONS ......................................................................................................... 9 DOSAGE AND ADMINISTRATION ................................................................................... 10 OVERDOSAGE...................................................................................................................... 10 ACTION AND CLINICAL PHARMACOLOGY.................................................................. 10 STORAGE AND STABILITY............................................................................................... 11 DOSAGE FORMS, COMPOSITION AND PACKAGING -

Selective Androgen Receptor Modulators: the Future of Androgen Therapy?
148 Review Article Selective androgen receptor modulators: the future of androgen therapy? Andrew R. Christiansen1, Larry I. Lipshultz2,3, James M. Hotaling4, Alexander W. Pastuszak4 1University of Utah School of Medicine, Salt Lake City, UT, USA; 2Scott Department of Urology; 3Center for Reproductive Medicine, Baylor College of Medicine, Houston, TX, USA; 4Division of Urology, Department of Surgery, University of Utah School of Medicine, Salt Lake City, UT, USA Contributions: (I) Conception and design: AR Christiansen; (II) Administrative support: AW Pastuszak; (III) Provision of study material or patients: AR Christiansen; (IV) Collection and assembly of data: AR Christiansen; (V) Data analysis and interpretation: AR Christiansen; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Alexander W. Pastuszak, MD, PhD. Assistant Professor, Division of Urology, Department of Surgery, University of Utah School of Medicine, Salt Lake City, UT, USA. Email: [email protected]. Abstract: Selective androgen receptor modulators (SARMs) are small molecule drugs that function as either androgen receptor (AR) agonists or antagonists. Variability in AR regulatory proteins in target tissues permits SARMs to selectively elicit anabolic benefits while eschewing the pitfalls of traditional androgen therapy. SARMs have few side effects and excellent oral and transdermal bioavailability and may, therefore, represent viable alternatives to current androgen therapies. SARMs have been studied as possible therapies for many conditions, including osteoporosis, Alzheimer’s disease, breast cancer, stress urinary incontinence (SUI), prostate cancer (PCa), benign prostatic hyperplasia (BPH), male contraception, hypogonadism, Duchenne muscular dystrophy (DMD), and sarcopenia/muscle wasting/cancer cachexia. While there are no indications for SARMs currently approved by the Food and Drug Administration (FDA), many potential applications are still being explored, and results are promising. -

Context-Specific Efficacy of Apalutamide Therapy in Preclinical
cancers Article Context-Specific Efficacy of Apalutamide Therapy in Preclinical Models of Pten-Deficient Prostate Cancer Marco A. De Velasco 1,2,* , Yurie Kura 1,2, Naomi Ando 1, Noriko Sako 1, Eri Banno 1, Kazutoshi Fujita 1, Masahiro Nozawa 1, Kazuhiro Yoshimura 1 , Kazuko Sakai 2, Kazuhiro Yoshikawa 3, Kazuto Nishio 2 and Hirotsugu Uemura 1,* 1 Department of Urology Kindai, University Faculty of Medicine, Osaka-Sayama 589-8511, Japan; [email protected] (Y.K.); [email protected] (N.A.); [email protected] (N.S.); [email protected] (E.B.); [email protected] (K.F.); [email protected] (M.N.); [email protected] (K.Y.) 2 Department of Genome Biology, Kindai University Faculty of Medicine, Osaka-Sayama 589-8511, Japan; [email protected] (K.S.); [email protected] (K.N.) 3 Research Creation Support Center, Aichi Medical University, Nagakute 480-1195, Japan; [email protected] * Correspondence: [email protected] (M.A.D.V.); [email protected] (H.U.) Simple Summary: Next-generation antiandrogens have transformed the therapeutic landscape for castration-resistant prostate cancer. Their utility in other indications, such as high-risk castration- sensitive cancers and as combination therapy, are being investigated. Our aim was to profile the in vivo antitumor activity of apalutamide in phenotypically distinct mouse models of Pten-deficient castration-naïve and castration-resistant prostate cancer, using both early- and late-stage disease Citation: De Velasco, M.A.; Kura, Y.; models, and to profile the molecular responses. -

Cancer Palliative Care and Anabolic Therapies
Cancer Palliative Care and Anabolic Therapies Aminah Jatoi, M.D. Professor of Oncology Mayo Clinic, Rochester, Minnesota USA • 2 Androgens • Creatine • Comments von Haehling S, et al, 2017 Oxandrolone: androgen that causes less virilization oxandrolone RANDOMIZE megestrol acetate #1: Oxandrolone (Lesser, et al, ASCO abstract 9513; 2008) • N=155 patients receiving chemotherapy • oxandrolone (10 mg twice a day x 12 weeks) versus megestrol acetate (800 mg/day x 12 weeks) • oxandrolone led to – a non-statistically significant increase in lean body mass (bioelectrical impedance) at 12 weeks (2.67 versus 0.82 pounds with megestrol acetate, p = 0.12), but – a decrease in overall weight as compared with megestrol acetate (-3.3 versus +5.8 pounds, respectively). • more oxandrolone patients dropped out prior to completing 12 weeks (63% versus 39 %). #2: Oxandrolone (von Roenn, et al, ASCO, 2003) • N=131 • Single arm • 81% of patients gained/maintained weight • Safe (PRIMARY ENDPOINT): 19% edema; 18% dyspnea; mild liver function test abnormalities #3: Oxandrolone: placebo controlled trial • results unknown SUMMARY OF OXANDROLONE: • Multiple studies (not yet peer-reviewed) • Hints of augmentation of lean tissue • High drop out in the phase 3 oxandrolone arm raises concern Enobosarm: selective androgen receptor modulator (less virilizing) ENOBOSARM RANDOMIZE* PLACEBO *All patients had non-small cell lung cancer, and chemotherapy was given concomittantly. percentage of subjects at day 84 with stair climb power change >=10% from their baseline value percentage of subjects at day 84 with lean body mass change >=0% from their baseline value SUMMARY OF ENOBOSARM: • Leads to incremental lean body mass, but functionality not demonstrated • Pivotal registration trial (not yet peer- reviewed (but FDA-reviewed….)) • 2 Androgens • Creatine • Comments Creatine: an amino acid derivative This study was funded by R21CA098477 and the Alliance for Clinical Trials NCORP grant. -

Sarms in Dietary Supplements and Other Products
SARMs in Dietary Supplements and Other Products Selective androgen receptor modulators, or SARMs, are syn- damage.” They’re also prohibited for use in sport. For exam- thetic drugs designed to mimic the effects of testosterone. Al- ple, a 2017 FDA Safety Alert describes andarine and ostarine though these drugs are still in the research and testing stages as “unapproved drugs and anabolic steroid-like substances.” of development, and they are classified as drugs, yet most are In addition, some experimental drugs that are not SARMs are readily available online both as ingredients in dietary supple- being marketed as or along with SARMs, but they are equally ment products and as chemicals available for “research only.” illegal in dietary supplements and prohibited for sport. As a Some websites marketing SARMs for “research use” include result, the most common of these are also included on the next descriptions with language clearly targeting use for bodybuild- page. In addition, there are dietary supplements marketed as ing. However, according to FDA “Body-building products that contain selective androgen receptor modulators, or SARMs, SARMs that do not contain any of the drugs listed here. The have not been approved by the FDA and are associated with following list will help you recognize these drugs, which often serious safety concerns, including potential to increase the risk go by various names, as well as currently available products of heart attack or stroke and life threatening reactions like liver that contain them. SARMs • LGD-3033 -

UFC PROHIBITED LIST Effective June 1, 2021 the UFC PROHIBITED LIST
UFC PROHIBITED LIST Effective June 1, 2021 THE UFC PROHIBITED LIST UFC PROHIBITED LIST Effective June 1, 2021 PART 1. Except as provided otherwise in PART 2 below, the UFC Prohibited List shall incorporate the most current Prohibited List published by WADA, as well as any WADA Technical Documents establishing decision limits or reporting levels, and, unless otherwise modified by the UFC Prohibited List or the UFC Anti-Doping Policy, Prohibited Substances, Prohibited Methods, Specified or Non-Specified Substances and Specified or Non-Specified Methods shall be as identified as such on the WADA Prohibited List or WADA Technical Documents. PART 2. Notwithstanding the WADA Prohibited List and any otherwise applicable WADA Technical Documents, the following modifications shall be in full force and effect: 1. Decision Concentration Levels. Adverse Analytical Findings reported at a concentration below the following Decision Concentration Levels shall be managed by USADA as Atypical Findings. • Cannabinoids: natural or synthetic delta-9-tetrahydrocannabinol (THC) or Cannabimimetics (e.g., “Spice,” JWH-018, JWH-073, HU-210): any level • Clomiphene: 0.1 ng/mL1 • Dehydrochloromethyltestosterone (DHCMT) long-term metabolite (M3): 0.1 ng/mL • Selective Androgen Receptor Modulators (SARMs): 0.1 ng/mL2 • GW-1516 (GW-501516) metabolites: 0.1 ng/mL • Epitrenbolone (Trenbolone metabolite): 0.2 ng/mL 2. SARMs/GW-1516: Adverse Analytical Findings reported at a concentration at or above the applicable Decision Concentration Level but under 1 ng/mL shall be managed by USADA as Specified Substances. 3. Higenamine: Higenamine shall be a Prohibited Substance under the UFC Anti-Doping Policy only In-Competition (and not Out-of- Competition). -

WO 2018/111890 Al 21 June 2018 (21.06.2018) W !P O PCT
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2018/111890 Al 21 June 2018 (21.06.2018) W !P O PCT (51) International Patent Classification: EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, LV, C07K 16/28 (2006.01) A61K 31/4166 (2006.01) MC, MK, MT, NL, NO, PL, PT, RO, RS, SE, SI, SK, SM, 59/595 (2006.01) TR), OAPI (BF, BJ, CF, CG, CI, CM, GA, GN, GQ, GW, KM, ML, MR, NE, SN, TD, TG). (21) International Application Number: PCT/US20 17/065841 Declarations under Rule 4.17: (22) International Filing Date: — as to applicant's entitlement to apply for and be granted a 12 December 2017 (12.12.2017) patent (Rule 4.1 7(H)) — as to the applicant's entitlement to claim the priority of the (25) Filing Language: English earlier application (Rule 4.17(Hi)) (26) Publication Langi English — of inventorship (Rule 4.1 7(iv)) (30) Priority Data: Published: 62/433,158 12 December 2016 (12.12.2016) US — with international search report (Art. 21(3)) — with sequence listing part of description (Rule 5.2(a)) (71) Applicant (for all designated States except AL, AT, BE, BG, CH, CN, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IN, IS, IT, LT, LU, LV, MC, MK, MT, NL, NO, PL, P T RO, RS, SE, SI, SK, SM, TR): GENENTECH, INC. [US/US]; 1 DNA Way, South San Francisco, CA 94080-4990 (US). -

Part I Biopharmaceuticals
1 Part I Biopharmaceuticals Translational Medicine: Molecular Pharmacology and Drug Discovery First Edition. Edited by Robert A. Meyers. © 2018 Wiley-VCH Verlag GmbH & Co. KGaA. Published 2018 by Wiley-VCH Verlag GmbH & Co. KGaA. 3 1 Analogs and Antagonists of Male Sex Hormones Robert W. Brueggemeier The Ohio State University, Division of Medicinal Chemistry and Pharmacognosy, College of Pharmacy, Columbus, Ohio 43210, USA 1Introduction6 2 Historical 6 3 Endogenous Male Sex Hormones 7 3.1 Occurrence and Physiological Roles 7 3.2 Biosynthesis 8 3.3 Absorption and Distribution 12 3.4 Metabolism 13 3.4.1 Reductive Metabolism 14 3.4.2 Oxidative Metabolism 17 3.5 Mechanism of Action 19 4 Synthetic Androgens 24 4.1 Current Drugs on the Market 24 4.2 Therapeutic Uses and Bioassays 25 4.3 Structure–Activity Relationships for Steroidal Androgens 26 4.3.1 Early Modifications 26 4.3.2 Methylated Derivatives 26 4.3.3 Ester Derivatives 27 4.3.4 Halo Derivatives 27 4.3.5 Other Androgen Derivatives 28 4.3.6 Summary of Structure–Activity Relationships of Steroidal Androgens 28 4.4 Nonsteroidal Androgens, Selective Androgen Receptor Modulators (SARMs) 30 4.5 Absorption, Distribution, and Metabolism 31 4.6 Toxicities 32 Translational Medicine: Molecular Pharmacology and Drug Discovery First Edition. Edited by Robert A. Meyers. © 2018 Wiley-VCH Verlag GmbH & Co. KGaA. Published 2018 by Wiley-VCH Verlag GmbH & Co. KGaA. 4 Analogs and Antagonists of Male Sex Hormones 5 Anabolic Agents 32 5.1 Current Drugs on the Market 32 5.2 Therapeutic Uses and Bioassays -

CAS Number Index
2334 CAS Number Index CAS # Page Name CAS # Page Name CAS # Page Name 50-00-0 905 Formaldehyde 56-81-5 967 Glycerol 61-90-5 1135 Leucine 50-02-2 596 Dexamethasone 56-85-9 963 Glutamine 62-44-2 1640 Phenacetin 50-06-6 1654 Phenobarbital 57-00-1 514 Creatine 62-46-4 1166 α-Lipoic acid 50-11-3 1288 Metharbital 57-22-7 2229 Vincristine 62-53-3 131 Aniline 50-12-4 1245 Mephenytoin 57-24-9 1950 Strychnine 62-73-7 626 Dichlorvos 50-23-7 1017 Hydrocortisone 57-27-2 1428 Morphine 63-05-8 127 Androstenedione 50-24-8 1739 Prednisolone 57-41-0 1672 Phenytoin 63-25-2 335 Carbaryl 50-29-3 569 DDT 57-42-1 1239 Meperidine 63-75-2 142 Arecoline 50-33-9 1666 Phenylbutazone 57-43-2 108 Amobarbital 64-04-0 1648 Phenethylamine 50-34-0 1770 Propantheline bromide 57-44-3 191 Barbital 64-13-1 1308 p-Methoxyamphetamine 50-35-1 2054 Thalidomide 57-47-6 1683 Physostigmine 64-17-5 784 Ethanol 50-36-2 497 Cocaine 57-53-4 1249 Meprobamate 64-18-6 909 Formic acid 50-37-3 1197 Lysergic acid diethylamide 57-55-6 1782 Propylene glycol 64-77-7 2104 Tolbutamide 50-44-2 1253 6-Mercaptopurine 57-66-9 1751 Probenecid 64-86-8 506 Colchicine 50-47-5 589 Desipramine 57-74-9 398 Chlordane 65-23-6 1802 Pyridoxine 50-48-6 103 Amitriptyline 57-92-1 1947 Streptomycin 65-29-2 931 Gallamine 50-49-7 1053 Imipramine 57-94-3 2179 Tubocurarine chloride 65-45-2 1888 Salicylamide 50-52-2 2071 Thioridazine 57-96-5 1966 Sulfinpyrazone 65-49-6 98 p-Aminosalicylic acid 50-53-3 426 Chlorpromazine 58-00-4 138 Apomorphine 66-76-2 632 Dicumarol 50-55-5 1841 Reserpine 58-05-9 1136 Leucovorin 66-79-5