CODE MÉDICAL FIM FIM Medical Code
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
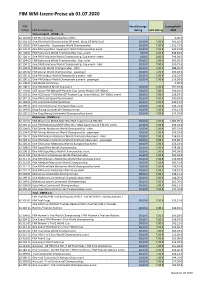
FIM WM-Lizenz-Preise Ab 01.07.2020
FIM WM‐Lizenz‐Preise ab 01.07.2020 FIM Versicherungs‐ Lizenzgebühr Artikel FIM Bezeichnung Betrag AKV‐Betrag 2020 Strassensport ‐ DMSB e.V. 62 101 00 FIM World Championship Grand Prix 0,00 € 62 101 10 One FIM World Championship GP event Moto GP Wild Card 20,00 €7,00 € 491,16 € 62 102 01 FIM Superbike – Supersport World Championship 30,00 €7,00 € 1.521,72 € 62 102 11 One FIM Superbike–Supersport World Championship event 20,00 €7,00 € 540,22 € 62 104 01 FIM Endurance World Championship, Cup – team 0,00 €0,00 € 848,84 € 62 104 11 One FIM Endurance World Championship, Cup event – team 0,00 €0,00 € 299,30 € 62 104 02 FIM Endurance World Championship , Cup ‐ rider 30,00 €7,00 € 565,92 € 62 104 12 One FIM Endurance World Championship, Cup event ‐ rider 20,00 €7,00 € 250,73 € 62 105 01 FIM Sidecar World Championship ‐ rider 30,00 €7,00 € 388,30 € 62 105 02 FIM Sidecar World Championship ‐ passenger 30,00 €7,00 € 290,18 € 62 105 11 One FIM Sidecar World Championship event ‐ rider 20,00 €7,00 € 156,53 € 62 105 12 One FIM Sidecar World Championship event ‐ passenger 20,00 €7,00 € 116,30 € 62 108 01 FIM MotoE World Cup 0,00 € 62 108 11 One FIM MotoE World Cup event 20,00 €7,00 € 201,67 € 62 118 01 CCR Junior FIM (MotoGP Rookies Cup, Junior Moto3, SSP 300cc) 30,00 €7,00 € 290,18 € 62 118 11 One CCR Junior FIM (MotoGP Rookies Cup, Junior Moto3, SSP 300cc) event 20,00 €7,00 € 156,53 € 62 197 11 One FIM Land Speed Record event 20,00 €7,00 € 240,93 € 62 199 01 CCR Continental Championships 30,00 €7,00 € 346,11 € 62 199 11 One CCR Continental Championships event 20,00 €7,00 € 144,76 € 62 199 02 Drag Racing Continental Championships 30,00 €7,00 € 346,11 € 62 199 12 One Drag Racing Continental Championships event 20,00 €7,00 € 144,76 € Motocross ‐ DMSB e.V. -

Ranking 2019 Po Zaliczeniu 182 Dyscyplin
RANKING 2019 PO ZALICZENIU 182 DYSCYPLIN OCENA PKT. ZŁ. SR. BR. SPORTS BEST 1. Rosja 384.5 2370 350 317 336 111 33 2. USA 372.5 2094 327 252 282 107 22 3. Niemcy 284.5 1573 227 208 251 105 17 4. Francja 274.5 1486 216 192 238 99 15 5. Włochy 228.0 1204 158 189 194 96 10 6. Wielka Brytania / Anglia 185.5 915 117 130 187 81 5 7. Chiny 177.5 1109 184 122 129 60 6 8. Japonia 168.5 918 135 135 108 69 8 9. Polska 150.5 800 103 126 136 76 6 10. Hiszpania 146.5 663 84 109 109 75 6 11. Australia 144.5 719 108 98 91 63 3 12. Holandia 138.5 664 100 84 96 57 4 13. Czechy 129.5 727 101 114 95 64 3 14. Szwecja 123.5 576 79 87 86 73 3 15. Ukraina 108.0 577 78 82 101 52 1 16. Kanada 108.0 462 57 68 98 67 2 17. Norwegia 98.5 556 88 66 72 42 5 18. Szwajcaria 98.0 481 66 64 89 59 3 19. Brazylia 95.5 413 56 63 64 56 3 20. Węgry 89.0 440 70 54 52 50 3 21. Korea Płd. 80.0 411 61 53 61 38 3 22. Austria 78.5 393 47 61 83 52 2 23. Finlandia 61.0 247 30 41 51 53 3 24. Nowa Zelandia 60.0 261 39 35 35 34 3 25. Słowenia 54.0 278 43 38 30 29 1 26. -

Fim Track Racing Appendices
FIM TRACK RACING APPENDICES 2020 CHANGES FROM 01.01.2020 GENERAL SECTION 70.1.1 Titles– Flat Track 70.4.2 Age of the Riders – Flat Track 70.5.1 Race Jackets – Clarification 70.8 Practices – Team meetings 70.10.3 Punctuality in starting - Clarification Side car 70.11.1 Calculations of results - Clarification Ice Speedway 70.12.2.1 Hotel accommodation - Clarification Youth Long Track Long Track of Nations FIM SPEEDWAY U21 WORLD CHAMPIONSHIP Races – Classification 72.5.6 Point system FIM TEAM SPEEDWAY U21 WORLD CHAMPIONSHIP 72b.3 Team composition - New 72b.6 Format - New 72b.9 Prize money – New FIM LONG TRACK WORLD CHAMPIONSHIP 73.5 Format – Clarification for QR + Chall. Semis and Final – New Point system - New FIM LONG TRACK of NATIONS 73b.3 Team composition –7 Teams 73b.6 Format – 7 Teams 73b.6.1 Ties - Clarification 73b.9 Re-staging: Clarification FIM ICE SPEEDWAY WORLD CHAMPIONSHIP 74.3.1 Riding number jackets FIM ICE SPEEDWAY of NATIONS 74b.3 Race format – Day 2 YOUTH No semi or final 7C3.2.1 Track Reserve FIM FLAT TRACK WORLD CHAMPIONSHIP All new 04.02.2020 FIM SPEEDWAY U21 WORLD CHAMPIONSHIP 72.5.6 Races – Clarification for classification FIM ICE SPEEDWAY WORLD CHAMPIONSHIP 74.8 Results – Clarification for classification FIM ICE SPEEDWAY of NATIONS 74b.3 Race format – Day 2 – Typing error FIM FLAT TRACK WORLD CHAMPIONSHIP 7E.6 Points system – clarification for classification 07.02.2020 GENERAL SECTION 70.2.4.1 Alcohol ballot and accident report not to be sent to FIM Admin. ISLB 71b.1.3 Priority days FIM ICE SPEEDWAY WORLD CHAMPIONSHIP -

Ranking 2018 Po Zaliczeniu 120 Dyscyplin
RANKING 2018 PO ZALICZENIU 120 DYSCYPLIN OCENA PKT. ZŁ. SR. BR. SPORTS BEST 1. Rosja 238.5 1408 219 172 187 72 16 2. USA 221.5 1140 163 167 154 70 18 3. Niemcy 185.0 943 140 121 140 67 7 4. Francja 144.0 736 101 107 118 66 4 5. Włochy 141.0 701 98 96 115 63 8 6. Polska 113.5 583 76 91 97 50 8 7. Chiny 108.0 693 111 91 67 35 6 8. Czechy 98.5 570 88 76 66 43 7 9. Kanada 92.5 442 61 60 78 45 5 10. Wielka Brytania / Anglia 88.5 412 51 61 86 49 1 11. Japonia 87.5 426 59 68 54 38 3 12. Szwecja 84.5 367 53 53 49 39 3 13. Ukraina 84.0 455 61 65 81 43 1 14. Australia 73.5 351 50 52 47 42 3 15. Norwegia 72.5 451 66 63 60 31 2 16. Korea Płd. 68.0 390 55 59 52 24 3 17. Holandia 68.0 374 50 57 60 28 3 18. Austria 64.5 318 51 34 46 38 4 19. Szwajcaria 61.0 288 41 40 44 33 1 20. Hiszpania 57.5 238 31 34 46 43 1 21. Węgry 53.0 244 35 37 30 27 3 22. Nowa Zelandia 42.5 207 27 35 29 25 2 23. Brazylia 42.0 174 27 20 26 25 4 24. Finlandia 42.0 172 23 23 34 33 1 25. Białoruś 36.0 187 24 31 29 22 26. -

Estructura Y Organización Del Deporte Paralímpico Una Mirada Internacional
EstructuraEstructura yy OrganizaciónOrganización deldel DeporteDeporte ParalímpicoParalímpico UnaUna miradamirada InternacionalInternacional Publicada bajo la dirección de: Joël Gaillard Luz Amelia Hoyos Cuartas Jairo Alejandro Fernández Ortega Estructura y Organización del Deporte Paralímpico Una mirada Internacional Publicada bajo la direccion de: Joël Gaillard Luz Amelia Hoyos Cuartas Jairo Alejandro Fernández Ortega Contenido Página Presentación ....................................................................................................................5 Abstract ...........................................................................................................................7 Presentation .....................................................................................................................9 LATINOAMÉRICA ARGENTINA ..............................................................................................................13 Legislación y estructura del deporte y el deporte paralímpico en Argentina. Débora Di Domizio. BRASIL ........................................................................................................................29 O estado da arte da pessoa com deficiência e o esporte no Brasil. Leonardo José Maturana-Dos-Santos, Elisabeth de Mattos, Silvestre Cirilo dos Santos Neto, Marcelo de Castro Haiachi, Mauro Cesar Gurgel de Alencar Carvalho. COLOMBIA ................................................................................................................73 Legislación y -

Ice Speedway of Nations in Russland
www.dmsb.de DIE WELT DES MOTORSPORTS 2/2019 ICE SPEEDWAY OF NATIONS IN RUSSLAND UMWELT RALLYCROSS DMSJ DMSB RICHTET DAS THEMA NEUE PROMOTOREN-AG VOLLVERSAMMLUNG MIT UMWELT NEU AUS STÄRKT DIE DRX VORSTANDSWAHLEN INHALT | VORSTART Eisspeedway FÖRDERER DES DMSB Beim Eisspeedway of Nations im russischen Togliatti sicherte sich das Fahrer‑Trio der Gastgebernation erwartungsgemäß den Team‑WM‑Titel. Beim großen Showdown bezwang das russische Team die Schweden. Im Feld der sieben angetretenen Teams sicherte sich Österreich den dritten Platz. Die deutsche Mannschaft beendete den Wettkampf als Viertplatzierte. Seite 14 KAPITEL 4 Kurz notiert 8 DMSB | DMSB richtet das Thema Umwelt neu aus 9 Internationale Kommissionen | Die DMSB‑Vertreter in der FIM 10 Internationale Kommissionen | Die DMSB‑Vertreter in der FIM Europe 11 Kartsport | Fabio Rauer startet in der CIK‑FIA Karting Academy Trophy 12 Rallycross | Die DRX startet 2019 neu durch 13 DMSB Academy | Rallye‑Workshop für Sportwarte in den Niederlanden 13 DMSB Academy | Neue Ausbildungsrichtlinien online 13 DMSB Academy | International Stewards Meeting in Frankfurt 13 DMSB Academy | Jetzt anmelden: Seminar Race Resource Management im April 14 Ice Speedway of Nations | Gold für Russland, Deutschland auf Rang vier 16 dmsj | 21. dmsj-Vollversammlung: Jürgen Hieke als dmsj-Vorsitzender wiedergewählt 19 Technik Automobilsport 21 Technik Kartsport 22 Technik Zusammenfassung 2018 IMPRESSUM Vorstart: Die Welt des Motorsports. Offizielles Fotos: ADAC · Thomas Bubel · DMSB · DMSB Organ des DMSB (Deutscher -

Approved Events for Sports Wagering (Last Updated September 23, 2021)1
INDIANA GAMING COMMISSION Greg Small Executive Director EAST TOWER, SUITE 1600 101 W. WASHINGTON STREET TELEPHONE (317) 233-0046 INDIANAPOLIS, IN 46204-3408 FAX (317) 233-0047 www.in.gov/igc Approved Events for Sports Wagering (last updated September 23, 2021)1 1. Aussie Rules Football A. AFL 2. Auto Racing A. Constructors’ Championships B. Formula One C. IndyCar D. MOTO GP E. NASCAR (including Monster Energy Series, Xfinity Series Truck Series) 3. Baseball A. The KBO League B. Minor League Baseball – Triple A C. MLB and MLB Draft D. Nippon Professional Baseball E. NCAA – Division 1 4. Basketball A. Big3 League B. Euro League and Euro Cup C. FIBA Champions League and Qualifiers D. International Basketball Federation (country v. country qualifiers/games/tournaments) E. NBA, NBA Draft, NBA Lottery F. NCAA - Division 1 G. The Basketball Tournament: TBT H. WNBA and WNBA Draft I. First Tier FIBA Leagues (Men/Women) from the following countries: Australia, Brazil, China, France, Germany (including cups), Israel, Italy, Japan, New Zealand, Spain (including cups) and Turkey 5. Bowling A. Pro Bowling Tour 6. Boxing A. Association of Boxing Commissions and Combative Sports B. British Boxing Board of Control C. International Boxing Federation D. August 29, 2021 - Jake Paul v. Tyron Woodley Match, as well as all professional bouts on the undercard E. World Boxing Association F. World Boxing Council G. World Boxing Organization 7. Bull Riding A. Professional Bull Riding, Inc. 1 Added Section 9(D). 8. Competitions A. Nathan’s Famous Hotdog Eating Contest 9. Cricket A. International Cricket Council B. Men’s and Women’s World Cup C. -

Paris Spo Rt
→ Press file 2017 – Paris Convention and Visitors Bureau SPORT PARIS 1 → Press file 2017 – Paris Convention and Visitors Bureau PARIS: A STAGE FOR MAJOR INTERNATIONAL SPORTING EVENTS ‘I love Paris because it is a city that loves sport: it has a passionate public, and a culture and tradition of high-level sport.’ These are the words of Novak Djokovic: a great champion’s tribute to SPORT a great sports city1. For, if Paris is a capital of art, culture, fashion and gastronomy, it is also a leading sporting destination, staging major international championships and events each year. Whatever your favourite sport, you can play it in Paris. Whatever your favourite team, Paris offers you the opportunity to support it, at exciting fixtures in legendary, world-class venues. PARIS Venues and high spots for top-level sport in Paris > For football fans Two renowned venues – the Stade de France and the Parc des Princes – host major league matches. Designed by Jean Nouvel, the Stade de France in northern Paris looks like a huge flying saucer. This is where the French national team plays its most important home matches. The stadium acquired the status of a national monument after France beat Brazil to win the 1998 World Cup. Then there is the Parc des Princes, a huge oval venue in the 16th arrondissement, right in the heart of the city. The home stadium of Paris Saint Germain, where a sizzling atmosphere reigns on match days, it hosts Europe’s top clubs each year during the prestigious Champions League. This historical venue is one of Europe’s most famous stadiums. -

SEE-E Content 2019
JANUARY FOOTBALL TENNIS MOTORSPORT AFC Asian Cup ATP World Tour Dakar Rally 05 Jan - 01 Feb 01 Jan - 24 Nov 06 Jan - 17 Jan Copa Libertadores Australian Open FIA World Rally Championship 22 Jan - 23 Nov 14 Jan - 27 Nov Jan – Nov Bundesliga, Portuguese WTATour League, Italian League, Dutch Jan – Oct League, Czech League, Greek League Davis Cup BADMINTON Aug 2018 – 2019 Jan – Nov BWF World Superseries / Grand Prix Gold English Premier League, Jan – Nov Spanish League, French League Aug 2018 – 2019 CYCLING UCI World Tour HANDBALL 15 Jan - 27 Oct Men’s Handball GOLF World Championships PGATour 09 Jan - 27 Jan 03 Jan - 25 Aug European Tour & LPGA Tour Jan – Nov MARCH APRIL FOOTBALL WINTER TENNIS HORSE Chinese Super League Fed Cup Semi-Finals Mar – Nov SPORTS 20 Apr - 21 Apr RACING World Women’s Curling Grand National Championship 6 Apr BASEBALL 16 Mar - 24 Mar GOLF World Men’s Curling MLB Spring Training ANA Inspiration Championship MOTORSPORT Mar 04 Apr - 07 Apr 30 Mar - 07 Apr World Touring Car Cup MLB Season The Masters Apr – Nov 28 Mar - 29 Sep 11 Apr - 14 Apr ATHLETICS BASKETBALL European Athletics Indoor AMERICAN BASKETBALL Championships NCAA Division Basketball NBA Playoffs 01 Mar - 03 Mar FOOTBALL 19 Mar - 08 Apr NFL Draft Apr – May ITU World Triathlon Series 25 Apr - 27 Apr Mar – Sep MOTORSPORT ATHLETICS MotoGP ICE HOCKEY Boston Marathon Mar – Aug GOLF NHL Playoffs 15 Apr Apr – Jun Formula 1 The Players Championships London Marathon Mar – Nov 12 Mar - 17 Mar 28 Apr 4 MAY TENNIS FOOTBALL ICE HOCKEY French Open IIHF World Championships -

2018 FIM Provisional Calendar
2018 PROVISIONAL CALENDAR CIRCUIT RACING MOTOCROSS TRIAL ENDURO RALLIES TRACK RACING 2018 PROVISIONAL CALENDAR FIM WORLD SUPERBIKE & SUPERSPORT CHAMPIONSHIP IMN START DATE END DATE PLACE COUNTRY 102/01 23/02/2018 25/02/2018 Phillip Island 102/02 23/03/2018 25/03/2018 Chang International Circuit 102/03 13/04/2018 15/04/2018 Motorland 102/04 20/04/2018 22/04/2018 Assen 102/05 11/5/2018 13/05/2018 Imola 102/06 25/05/2018 27/05/2018 Donington Park 102/07 8/6/2018 10/6/2018 Brno 102/08 22/06/2018 24/06/2018 Laguna Seca 102/09 6/7/2018 8/7/2018 Misano World Circuit Marco Simoncelli 102/10 14/09/2018 16/09/2018 Algarve 102/11 28/09/2018 30/09/2018 Magny-Cours 102/12 12/10/2018 14/10/2018 El Villicum 102/13 25/10/2018 27/10/2018 Losail International Circuit WORLD SUPERSPORT 300 IMN START DATE END DATE PLACE COUNTRY 116/01 13/04/2018 15/04/2018 Motorland 116/02 20/04/2018 22/04/2018 Assen 116/03 11/5/2018 13/05/2018 Imola 116/04 25/05/2018 27/05/2018 Donington Park 116/05 8/6/2018 10/6/2018 Brno 116/06 6/7/2018 8/7/2018 Misano World Circuit Marco Simoncelli 116/07 14/09/2018 16/09/2018 Algarve 116/08 28/09/2018 30/09/2018 Magny-Cours GRAND PRIX IMN START DATE END DATE PLACE COUNTRY 101/01 18/03/2018 18/03/2018 Losail International Circuit 101/02 8/4/2018 8/4/2018 Termas de Rio Hondo 101/03 22/04/2018 22/04/2018 Circuit of the Americas 101/04 6/5/2018 6/5/2018 Jerez de la Frontera 101/05 20/05/2018 20/05/2018 Le Mans 101/06 3/6/2018 3/6/2018 Mugello 101/07 17/06/2018 17/06/2018 Catalunya 101/08 1/7/2018 1/7/2018 Assen 101/09 15/07/2018 15/07/2018 -

2018 Coverage
2018 coverage Unrivalled highlights coverage sntv offers more cleared highlights from a wider range of sports than anyone else, offering the greatest breadth of sports coverage worldwide. Videos that inform and engage We provide our clients with the most relevant and engaging videos, either fully customisable or ready to publish directly to your audience. Global and regional sports video news Our dedicated teams fully understand what our clients are looking for, and recognise what content will drive conversations on both an international and regional level. January February March April May soccer soccer american football soccer baseball AFC Champions League Superbowl LII Chinese Super League MLB Season FA Cup Final Jan - Nov Feb Mar - Nov Apr - Oct May Copa Libertadores J.League UEFA Champions Jan - Nov rugby Mar - Dec basketball League Final RBS Six Nations NBA Playoffs May tennis Championship golf Apr - May UEFA Europa League Final ATP World Tour Feb - Mar ANA Inspiration May Jan - Nov Mar - Apr american football UEFA Women’s Champions Australian Open soccer NFL Draft League Final Jan EFL Cup Final baseball Apr May Davis Cup Feb MLB Spring Training Jan - Nov Mar ice hockey tennis Hopman Cup tennis NHL Playoffs French Open Jan Fed Cup motorsport Apr - Jun May - Jun WTA Tour Feb - Nov Jan - Oct Formula One Mar - Nov golf basketball golf golf Moto GP The Masters NBA Finals Apr European Tour Asian Tour Mar - Aug May - Jun Feb - Dec Jan - Nov MXGP Ladies European Tour motorsport golf LPGA Tour Mar - Oct Feb - Dec World Touring Car Players -

IWFA CHRISTMAS Invitational CHAMPIONSHIPS Medalists at the I.W.F.A
PHOTO BY GRADKOWSKI IWFA CHRISTMAS INVITATiONAL CHAMPIONSHIPS Medalists at the I.W.F.A. Christmas Invitational Championships were: (I to r) Ellen Jacobs, Brooklyn College, Silver medal, Ruth White, N.Y.U., Gold medal, Julia Jones, coach of Hunter College, wha donated and presented the awards, and Laura Dingle, Cornell, Bronze medalist. (SEE PAGE 14) VANDERBILT ATHLETIC CLUB HOST 21 Number 3 ;1IJl£;11Clll1 f El1CJ1]Jj OF 1970 NATIONAL CHAMPIONSHIPS Officio I Organ of the Amateur Fencers League of America AIR CONDITIONED FACILITIES IN HEART Of MANHATTAN; Dedicated to the Memory of its First Editor and SITE OF INTERNATIONAL TENNIS TOURNAMENTS Co-Founder JOSE R. DeCAPRILES, 1912-1969. Management By Richard Gradkowski W. L. Osborn, Publisher Rolph M. Goldstein, Editor 5 Great Oak Lone 397 Concord Rd. E. Csaba Gall, Chairman of the Metro politan Division, announces the holding of 'Ieasantville, N.Y. 10570 Yunkers, N. Y. 10710 the U. S. National Chompionships from July 2 .ssoc. Editor: Irwin Bernstein Asst. Editor: Richard Gradkowski to July 11 at the Vanderbilt Athletic Club in Feature Editors: Don Lyons, Mory Gehant Editorial Stoff: Marilyn Masiero. Historian: Alex Solomon New York. The spacious and air conditioned ertising Correspondence: 5 Great Oak Lane, Pleasantville, N. Y. 10510 Vonderbilt Club is located in the Grand Advertising Plates: P. O. Box 144, Terre Haute, Ind. 41808 Central Terminal Building in the heart of Monhattan. Policy Board A. Ruben, Chairman; R. M. Goldstein, W. J. Latzko. The club has unusually complete athletic W. L. 05born, P. Tishman, N. L. Lewis facilities with two large indoor tennis courts, ns for non-members of the AFLA is $3.00 in the.