Shelly Lwu Jan. 23, 2009 Spinal Cord
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Distance Learning Program Anatomy of the Human Brain/Sheep Brain Dissection
Distance Learning Program Anatomy of the Human Brain/Sheep Brain Dissection This guide is for middle and high school students participating in AIMS Anatomy of the Human Brain and Sheep Brain Dissections. Programs will be presented by an AIMS Anatomy Specialist. In this activity students will become more familiar with the anatomical structures of the human brain by observing, studying, and examining human specimens. The primary focus is on the anatomy, function, and pathology. Those students participating in Sheep Brain Dissections will have the opportunity to dissect and compare anatomical structures. At the end of this document, you will find anatomical diagrams, vocabulary review, and pre/post tests for your students. The following topics will be covered: 1. The neurons and supporting cells of the nervous system 2. Organization of the nervous system (the central and peripheral nervous systems) 4. Protective coverings of the brain 5. Brain Anatomy, including cerebral hemispheres, cerebellum and brain stem 6. Spinal Cord Anatomy 7. Cranial and spinal nerves Objectives: The student will be able to: 1. Define the selected terms associated with the human brain and spinal cord; 2. Identify the protective structures of the brain; 3. Identify the four lobes of the brain; 4. Explain the correlation between brain surface area, structure and brain function. 5. Discuss common neurological disorders and treatments. 6. Describe the effects of drug and alcohol on the brain. 7. Correctly label a diagram of the human brain National Science Education -

Split Spinal Cord Malformations in Children
Split spinal cord malformations in children Yusuf Ersahin, M.D., Saffet Mutluer, M.D., Sevgül Kocaman, R.N., and Eren Demirtas, M.D. Division of Pediatric Neurosurgery, Department of Neurosurgery, and Department of Pathology, Ege University Faculty of Medicine, Izmir, Turkey The authors reviewed and analyzed information on 74 patients with split spinal cord malformations (SSCMs) treated between January 1, 1980 and December 31, 1996 at their institution with the aim of defining and classifying the malformations according to the method of Pang, et al. Computerized tomography myelography was superior to other radiological tools in defining the type of SSCM. There were 46 girls (62%) and 28 boys (38%) ranging in age from less than 1 day to 12 years (mean 33.08 months). The mean age (43.2 months) of the patients who exhibited neurological deficits and orthopedic deformities was significantly older than those (8.2 months) without deficits (p = 0.003). Fifty-two patients had a single Type I and 18 patients a single Type II SSCM; four patients had composite SSCMs. Sixty-two patients had at least one associated spinal lesion that could lead to spinal cord tethering. After surgery, the majority of the patients remained stable and clinical improvement was observed in 18 patients. The classification of SSCMs proposed by Pang, et al., will eliminate the current chaos in terminology. In all SSCMs, either a rigid or a fibrous septum was found to transfix the spinal cord. There was at least one unrelated lesion that caused tethering of the spinal cord in 85% of the patients. -

The Strain Rates in the Brain, Brainstem, Dura, and Skull Under Dynamic Loadings
Mathematical and Computational Applications Article The Strain Rates in the Brain, Brainstem, Dura, and Skull under Dynamic Loadings Mohammad Hosseini-Farid 1,2,* , MaryamSadat Amiri-Tehrani-Zadeh 3, Mohammadreza Ramzanpour 1, Mariusz Ziejewski 1 and Ghodrat Karami 1 1 Department of Mechanical Engineering, North Dakota State University, Fargo, ND 58104, USA; [email protected] (M.R.); [email protected] (M.Z.); [email protected] (G.K.) 2 Department of Orthopedic Surgery, Mayo Clinic, Rochester, MN 55905, USA 3 Department of Computer Science, North Dakota State University, Fargo, ND 58104, USA; [email protected] * Correspondence: [email protected]; Tel.: +1-7012315859 Received: 7 March 2020; Accepted: 5 April 2020; Published: 7 April 2020 Abstract: Knowing the precise material properties of intracranial head organs is crucial for studying the biomechanics of head injury. It has been shown that these biological tissues are significantly rate-dependent; hence, their material properties should be determined with respect to the range of deformation rate they experience. In this paper, a validated finite element human head model is used to investigate the biomechanics of the head in impact and blast, leading to traumatic brain injuries (TBI). We simulate the head under various directions and velocities of impacts, as well as helmeted and unhelmeted head under blast shock waves. It is demonstrated that the strain rates for the brain 1 are in the range of 36 to 241 s− , approximately 1.9 and 0.86 times the resulting head acceleration under impacts and blast scenarios, respectively. The skull was found to experience a rate in the range 1 of 14 to 182 s− , approximately 0.7 and 0.43 times the head acceleration corresponding to impact and blast cases. -

Deconstructing Spinal Interneurons, One Cell Type at a Time Mariano Ignacio Gabitto
Deconstructing spinal interneurons, one cell type at a time Mariano Ignacio Gabitto Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy under the Executive Committee of the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2016 © 2016 Mariano Ignacio Gabitto All rights reserved ABSTRACT Deconstructing spinal interneurons, one cell type at a time Mariano Ignacio Gabitto Abstract Documenting the extent of cellular diversity is a critical step in defining the functional organization of the nervous system. In this context, we sought to develop statistical methods capable of revealing underlying cellular diversity given incomplete data sampling - a common problem in biological systems, where complete descriptions of cellular characteristics are rarely available. We devised a sparse Bayesian framework that infers cell type diversity from partial or incomplete transcription factor expression data. This framework appropriately handles estimation uncertainty, can incorporate multiple cellular characteristics, and can be used to optimize experimental design. We applied this framework to characterize a cardinal inhibitory population in the spinal cord. Animals generate movement by engaging spinal circuits that direct precise sequences of muscle contraction, but the identity and organizational logic of local interneurons that lie at the core of these circuits remain unresolved. By using our Sparse Bayesian approach, we showed that V1 interneurons, a major inhibitory population that controls motor output, fractionate into diverse subsets on the basis of the expression of nineteen transcription factors. Transcriptionally defined subsets exhibit highly structured spatial distributions with mediolateral and dorsoventral positional biases. These distinctions in settling position are largely predictive of patterns of input from sensory and motor neurons, arguing that settling position is a determinant of inhibitory microcircuit organization. -
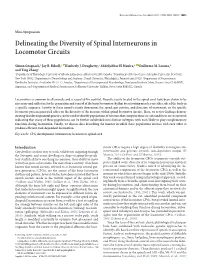
Delineating the Diversity of Spinal Interneurons in Locomotor Circuits
The Journal of Neuroscience, November 8, 2017 • 37(45):10835–10841 • 10835 Mini-Symposium Delineating the Diversity of Spinal Interneurons in Locomotor Circuits Simon Gosgnach,1 Jay B. Bikoff,2 XKimberly J. Dougherty,3 Abdeljabbar El Manira,4 XGuillermo M. Lanuza,5 and Ying Zhang6 1Department of Physiology, University of Alberta, Edmonton, Alberta T6G 2H7, Canada, 2Department of Neuroscience, Columbia University, New York, New York 10032, 3Department of Neurobiology and Anatomy, Drexel University, Philadelphia, Pennsylvania 19129, 4Department of Neuroscience, Karolinska Institutet, Stockholm SE-171 77, Sweden, 5Department of Developmental Neurobiology, Fundacion Instituto Leloir, Buenos Aires C1405BWE, Argentina, and 6Department of Medical Neuroscience, Dalhousie University. Halifax, Nova Scotia B3H 4R2, Canada Locomotion is common to all animals and is essential for survival. Neural circuits located in the spinal cord have been shown to be necessary and sufficient for the generation and control of the basic locomotor rhythm by activating muscles on either side of the body in a specific sequence. Activity in these neural circuits determines the speed, gait pattern, and direction of movement, so the specific locomotor pattern generated relies on the diversity of the neurons within spinal locomotor circuits. Here, we review findings demon- strating that developmental genetics can be used to identify populations of neurons that comprise these circuits and focus on recent work indicating that many of these populations can be further subdivided -
The Spinal Cord Is a Nerve Column That Passes Downward from Brain Into the Vertebral Canal
The spinal cord is a nerve column that passes downward from brain into the vertebral canal. Recall that it is part of the CNS. Spinal nerves extend to/from the spinal cord and are part of the PNS. Length = about 17 inches Start = foramen magnum End = tapers to point (conus medullaris) st nd and terminates 1 –2 lumbar (L1-L2) vertebra Contains 31 segments à gives rise to 31 pairs of spinal nerves Note cervical and lumbar enlargements. cauda equina (“horse’s tail”) –collection of spinal nerves at inferior end of vertebral column (nerves coming off end of spinal cord) Meninges- cushion and protected by same 3 layers as brain. Extend past end of cord into vertebral canal à spinal tap because no cord A cross-section of the spinal cord resembles a butterfly with its wings outspread (gray matter) surrounded by white matter. GRAY MATTER or “butterfly” = bundles of cell bodies Posterior (dorsal) horns=association or interneurons (incoming somatosensory information) Lateral horns=autonomic neurons Anterior (ventral) horns=cell bodies of motor neurons Central canal-found within gray matter and filled with CSF White Matter: 3 Regions: Posterior (dorsal) white column or funiculi – contains only ASCENDING tracts à sensory only Lateral white column or funiculi – both ascending and descending tracts à sensory and motor Anterior (ventral) white column or funiculi – both ascending and descending tracts à sensory and motor All nerve tracts made of mylinated axons with same destination and function Associated Structures: Dorsal Roots = made -

Acute Cauda Equina Syndrome Following Orthopedic Procedures As a Result of Epidural Anesthesia Lisa B
OPEN ACCESS Editor: Nancy E. Epstein, MD SNI: Spine For entire Editorial Board visit : Winthrop Hospital, Mineola, http://www.surgicalneurologyint.com NY, USA Case Report Acute cauda equina syndrome following orthopedic procedures as a result of epidural anesthesia Lisa B. E. Shields1, Vasudeva G. Iyer2, Yi Ping Zhang1, Christopher B. Shields1,3 1Norton Neuroscience Institute, Norton Healthcare, 2Neurodiagnostic Center of Louisville, 3Department of Neurological Surgery, University of Louisville School of Medicine, Louisville, Kentucky, USA E‑mail: Lisa B. E. Shields ‑ [email protected]; Vasudeva G. Iyer ‑ [email protected]; Yi Ping Zhang ‑ [email protected]; *Christopher B. Shields ‑ [email protected] *Corresponding author Received: 29 December 17 Accepted: 15 January 18 Published: 10 April 18 Abstract Background: Cauda equina syndrome (CES) is a rare complication of spinal or epidural anesthesia. It is attributed to direct mechanical injury to the spinal roots of the cauda equina that may result in saddle anesthesia and paraplegia with bowel and bladder dysfunction. Case Description: The first patient underwent a hip replacement and received 5 mL of 1% lidocaine epidural anesthesia. Postoperatively, when the patient developed an acute CES, the lumbar magnetic resonance imaging (MRI) scan demonstrated clumping/posterior displacement of nerve roots of the cauda equina consistent with adhesive arachnoiditis attributed to the patient’s previous L4‑L5 lumbar decompression/ fusion. The second patient underwent spinal anesthesia (injection of 10 mg of isobaric Access this article online bupivacaine for an epidural block) for a total knee replacement. When the patient Website: www.surgicalneurologyint.com developed an acute CES following surgery, the lumbar MRI scan showed an abnormal DOI: T2 signal in the conus and lower thoracic spinal cord over 4.3 cm. -

A Cauda Equina Syndrome in a Patient Treated with Oral Anticoagulants
Paraplegia 32 (1994) 277-280 © 1994 International Medical Society of Paraplegia A cauda equina syndrome in a patient treated with oral anticoagulants. Case report l l l 2 l J Willems MD, A Anne MD, P Herregods MD, R Klaes MD, R Chappel MD 1 Department of Physical Medicine and Rehabilitation, 2 Department of Neurosurgery, A.z. Middelheim, Lindendreef 1, B-2020 Antwerp, Belgium. The authors report a patient who was on oral anticoagulants because of mitral valve disease and who developed paraplegia from subarachnoid bleeding involv ing the cauda equina. The differential diagnosis, investigations and treatment of the cauda equina syndrome are described. Keywords: cauda equina syndrome; anticoagulants; subarachnoid haemorrhage; mitral valve disease. Case report A 32 year old woman from Chile presented with a complete paraplegia. She claimed that the paraplegia had developed progressively over 8 months. Initially she had paraesthesiae in her feet, followed by progressive paresis of both legs, beginning distally, over a period of 3 months. Two months after the onset of illness she complained of bladder incontinence. There was no history of trauma or low back pain. Clinical examination in our hospital revealed a flaccid paraplegia at L1 level, and loss of sensation from the groins to the feet, including saddle anaesthesia. The knee and ankle jerks were absent. The anal sphincter was atonic. She had an indwelling urethral catheter, and she was faecally incontinent. Myelography and a CT scan were carried out, and a space-occupying lesion at the level of T12-L4 (Figs 1, 2) was defined. Surgical ex ploration was done to determine the cause. -

Spinal Cord Organization
Lecture 4 Spinal Cord Organization The spinal cord . Afferent tract • connects with spinal nerves, through afferent BRAIN neuron & efferent axons in spinal roots; reflex receptor interneuron • communicates with the brain, by means of cell ascending and descending pathways that body form tracts in spinal white matter; and white matter muscle • gives rise to spinal reflexes, pre-determined gray matter Efferent neuron by interneuronal circuits. Spinal Cord Section Gross anatomy of the spinal cord: The spinal cord is a cylinder of CNS. The spinal cord exhibits subtle cervical and lumbar (lumbosacral) enlargements produced by extra neurons in segments that innervate limbs. The region of spinal cord caudal to the lumbar enlargement is conus medullaris. Caudal to this, a terminal filament of (nonfunctional) glial tissue extends into the tail. terminal filament lumbar enlargement conus medullaris cervical enlargement A spinal cord segment = a portion of spinal cord that spinal ganglion gives rise to a pair (right & left) of spinal nerves. Each spinal dorsal nerve is attached to the spinal cord by means of dorsal and spinal ventral roots composed of rootlets. Spinal segments, spinal root (rootlets) nerve roots, and spinal nerves are all identified numerically by th region, e.g., 6 cervical (C6) spinal segment. ventral Sacral and caudal spinal roots (surrounding the conus root medullaris and terminal filament and streaming caudally to (rootlets) reach corresponding intervertebral foramina) collectively constitute the cauda equina. Both the spinal cord (CNS) and spinal roots (PNS) are enveloped by meninges within the vertebral canal. Spinal nerves (which are formed in intervertebral foramina) are covered by connective tissue (epineurium, perineurium, & endoneurium) rather than meninges. -
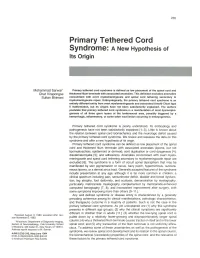
Primary Tethered Cord Syndrome: a New Hypothesis of Its Origin
235 Primary Tethered Cord Syndrome: A New Hypothesis of Its Origin Mohammad Sarwar' Primary tethered cord syndrome is defined as low placement of the spinal cord and Chat Virapongse thickened filum terminale with associated anomalies. This definition excludes anomalies Sultan Bhimani concomitant with overt myelomeningocele and spinal cord tethering secondary to myelomeningocele repair. Embryologically, the primary tethered cord syndrome is an entirely different entity from overt myelomeningocele and associated Arnold-Chiari type II malformation, but its origins have not been satisfactorily explained. The authors postulate that primary tethered cord syndrome is a manifestation of local dysmorpho genesis of all three germ layers at the lumbosacral area, possibly triggered by a hemorrhagic, inflammatory, or some other local lesion occurring in embryogenesis. Primary tethered cord syndrome is poorly understood. Its embryology and pathogenesis have not been satisfactorily explained [1-3]. Little is known about the relation between spinal cord biomechanics and the neurologic deficit caused by the primary tethered cord syndrome. We review and reassess the data on this syndrome and offer a new hypothesis of its origin. Primary tethered cord syndrome can be defined as low placement of the spinal cord and thickened filum terminale with associated anomalies (lipoma, but not lipomyeloschisis; epidermoid or dermoid; cord duplication or cord dysgenesis [4 J; diastematomyelia [5]; and adhesions). Anomalies concomitant with overt myelo meningocele and spinal cord tethering secondary to myelomeningocele repair are excluded [6]. The syndrome is a form of occult spinal dysraphism that may be manifested by skin pigmentation or nevus, hairy patch, hypertrichosis, subcuta neous lipoma, or a dermal sinus tract. -

Review of Spinal Cord Basics of Neuroanatomy Brain Meninges
Review of Spinal Cord with Basics of Neuroanatomy Brain Meninges Prof. D.H. Pauža Parts of Nervous System Review of Spinal Cord with Basics of Neuroanatomy Brain Meninges Prof. D.H. Pauža Neurons and Neuroglia Neuron Human brain contains per 1011-12 (trillions) neurons Body (soma) Perikaryon Nissl substance or Tigroid Dendrites Axon Myelin Terminals Synapses Neuronal types Unipolar, pseudounipolar, bipolar, multipolar Afferent (sensory, centripetal) Efferent (motor, centrifugal, effector) Associate (interneurons) Synapse Presynaptic membrane Postsynaptic membrane, receptors Synaptic cleft Synaptic vesicles, neuromediator Mitochondria In human brain – neurons 1011 (100 trillions) Synapses – 1015 (quadrillions) Neuromediators •Acetylcholine •Noradrenaline •Serotonin •GABA •Endorphin •Encephalin •P substance •Neuronal nitric oxide Adrenergic nerve ending. There are many 50-nm-diameter vesicles (arrow) with dark, electron-dense cores containing norepinephrine. x40,000. Cell Types of Neuroglia Astrocytes - Oligodendrocytes – Ependimocytes - Microglia Astrocytes – a part of hemoencephalic barrier Oligodendrocytes Ependimocytes and microglial cells Microglia represent the endogenous brain defense and immune system, which is responsible for CNS protection against various types of pathogenic factors. After invading the CNS, microglial precursors disseminate relatively homogeneously throughout the neural tissue and acquire a specific phenotype, which clearly distinguish them from their precursors, the blood-derived monocytes. The ´resting´ microglia -

Occult Intrasacral Meningocoele
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.4.493 on 1 August 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 493496 Occult intrasacral meningocoele ROMA A. JOSEPH AND THOMAS McKENZIE From the Neurosurgical Department, General Hospital, San Fernando, Trinidad, W.L SUMMARY A case is reported of the rare lesion occult intrasacral meningocoele in a 27-year-old woman who developed symptoms for the first time shortly after the birth of her fourth child. The terminology of the condition is discussed and its pathogenesis, mode of presentation, and treatment reviewed. The term 'occult intrasacral meningocoele' first used was unable to walk. She was treated conservatively and by Enderle (1932) describes the condition of ab- six weeks later she considered herself to be 'back to normal dilatation of the meninges within the confines normal'. At no time did she have bladder or bowel dis- workers turbance. Before this event she had no history of pain in of the sacral spinal canal. Various have her back or leg nor had she any symptoms suggestive of pointed out that this term is not strictly accurate in motor, sensory, or sphincter dysfunction. Her preg- guest. Protected by copyright. that a meningocoele implies a hernial protrusion of nancies and deliveries had all been normal. the meninges through a defect in the skull or verte- bral column. Thus, Howieson, Norrell, and Wilson EXAMINATION Physical examination showed hypotonia (1968) prefer to speak of 'expansion of the subarach- and loss of position sense in the left foot, impairment of noid space in the lumbosacral region'.