Equality & Inclusion Service User Monitoring & Assurance Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Sheffield Hallam University Thesis
Exploring the potential of complexity theory in urban regeneration processes. MOOBELA, Cletus. Available from the Sheffield Hallam University Research Archive (SHURA) at: http://shura.shu.ac.uk/20078/ A Sheffield Hallam University thesis This thesis is protected by copyright which belongs to the author. The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the author. When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given. Please visit http://shura.shu.ac.uk/20078/ and http://shura.shu.ac.uk/information.html for further details about copyright and re-use permissions. Fines are charged at 50p per hour JMUQ06 V-l 0 9 MAR ?R06 tjpnO - -a. t REFERENCE ProQuest Number: 10697385 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest ProQuest 10697385 Published by ProQuest LLC(2017). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC. ProQuest LLC. 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106- 1346 Exploring the Potential of Complexity Theory in Urban Regeneration Processes Cletus Moobela A Thesis Submitted in partial fulfilment of the requirements of Sheffield Hallam University for the Degree of Doctor of Philosophy July 2004 ACKNOWLEDGEMENTS The carrying out and completion of this research project was a stimulating experience for me in an area that I have come to develop an ever-increasing amount of personal interest. -
Exploring Greater Manchester
Exploring Greater Manchester a fieldwork guide Web edition edited by Paul Hindle Original printed edition (1998) edited by Ann Gardiner, Paul Hindle, John McKendrick and Chris Perkins Exploring Greater Manchester 5 5. Urban floodplains and slopes: the human impact on the environment in the built-up area Ian Douglas University of Manchester [email protected] A. The River Mersey STOP 1: Millgate Lane, Didsbury The urban development of Manchester has modified From East Didsbury station and the junction of the A34 runoff to rivers (see Figure 1), producing changes in and A5145, proceed south along Parrs Wood Road and into flood behaviour, which have required expensive remedial Millgate Lane, Stop at the bridge over the floodbasin inlet measures, particularly, the embankment of the Mersey from channel at Grid Reference (GR) 844896 (a car can be turned Stockport to Ashton weir near Urmston. In this embanked round at the playing fields car park further on). Looking reach, runoff from the urban areas includes natural channels, south from here the inlet channel from the banks of the storm drains and overflows from combined sewers. Mersey can be seen. At flood times the gates of the weir on Alternative temporary storages for floodwaters involve the Mersey embankment can be opened to release water into release of waters to floodplain areas as in the Didsbury flood the Didsbury flood basin that lies to the north. Here, and at basin and flood storage of water in Sale and Chorlton water other sites along the Mersey, evidence of multi-purpose use parks. This excursion examines the reach of the Mersey from of the floodplain, for recreation and wildlife conservation as Didsbury to Urmston. -

Buses Serving North Manchester General Hospital
Buses serving North Manchester General Hospital 52 Salford Shopping City, Broughton, Cheetham Hill, NMGH, Harpurhey, Moston, Newton Heath, Failsworth Tesco Bus Stops Daily service, operated by First Greater Manchester A,C, Pendleton Higher Broughton Cheetham Hill NMG Moston Newton Heath Brookdale Failsworth D,E,F Salford Shopping City McDonalds Crescent Road Hospital Ben Brierley Dean Lane Park Tesco Store 27 16 7 12 21 26 32 ______________________________________________________________________________________________________________________________________________ 53 Cheetham Hill, NMGH, Harpurhey, Miles Platting, SportCity, Gorton, Belle Vue, Longsight, Rusholme, Central Manchester Bus Stops Hospitals, Hulme, Old Trafford A,C, Daily service, operated by First Greater Manchester D,E,F Cheetham Hill NMG Harpurhey Sport Gorton Belle Rusholme University Old Trafford Salford Crescent Road Hospital Rochdale Rd City Vue of Manchester Trafford Bar Shopping City 7 7 16 31 35 50 58 68 80 _____________________________________________________________________________________________________________________________________________ 88=> Circulars, Manchester City Centre, Monsall, Moston, White Moss, Blackley, NMGH, Cheetham Hill, Manchester City Centre 89<= Daily service, operated by First Greater Manchester (Evenings, Sundays and Bank Holidays—JPT) Use these buses and change at Crumpsall Metrolink Station or Cheetham Hill, Cheetham Hill Rd (Bus 135) for Bury. Bus Stops Manchester Central Moston White Blackley Bank Crumpsall NMG Cheetham Manchester -
N SA Appendix 3 Details of Baseline Information
Publication Salford Local Plan: Development Management and Allocations Document Sustainability Appraisal Appendix 3 Details of Baseline Information APPENDIX 3 Details of Baseline Information Contents 1. Introduction ........................................................................................................ 2 2 Social .................................................................................................................. 3 2A Population .............................................................................................................. 3 2B Health ..................................................................................................................... 7 2C Crime ................................................................................................................... 10 2D Accessibility .......................................................................................................... 11 2E Housing ................................................................................................................ 15 2F Education ............................................................................................................. 21 3. Economic .......................................................................................................... 25 3A Economic health ................................................................................................... 25 3B Structure of the economy .................................................................................... -

Gm Green City Region Partnership
GM GREEN CITY REGION PARTNERSHIP Date: 12th March 2021 Subject: PERFORMANCE UPDATE – Q4 (Jan-Mar) Report of: Mark Atherton, Director Environment, GMCA PURPOSE OF REPORT The report provides the usual update on progress of the Green City Region Partnership for the fourth quarter of 2020/21. RECOMMENDATIONS: The Partnership is recommended to: Note and comment upon the progress outlined in this report and latest position set out in the dashboards attached at: a. Annex 01 (Environment Performance Overview) and b. Annex 02 (5 Year Environment Plan KPIs). CONTACT OFFICERS: Contact Officer: Mark Atherton, GM Director of Environment [email protected] 1.0 OVERVIEW OF PROGRESS The updates at Annexes 01 (Environment Team Performance Overview) & 02 (5 Year Environment Plan Performance) contain a summary of key achievements during the last quarter across the areas within the 5 Year Environment Plan. There are a number of key successes to be highlighted, set out below: Energy Local Area Energy Planning (LAEP)/LEM - Bury’s LAEP is to be issued by ESC by the end of March 21; Bruntwood and OVO have issued their respective proposals for Non-Domestic and Domestic Value Sharing propositions; OVO have issued their survey for the use of Sonnen batteries and Bruntwood are in contract talks to install trial EV chargers during the month of Mar 21; Daikin and Northward Housing to trial the installation of ASHPs to existing building stock; Carbon Co-op have commenced all user engagement requirements; Bruntwood has appointed Upside Energy to assist in the design development of the market making platform; REGEN have commenced discussions with key partners for the development of the business case ref investment and Cornwall Insight have overseen all regulatory issues and advised accordingly. -

Immigration Timeline
14th Century 18th Century 19th Century 19th Century 19th Century 20th Century 20th Century 20th Century 20th Century 21st Century 1353 1600s 1780 onwards 1821-1831 Mid 1800s 1844 1847 1861 1871-1881 1894 1898 1904 1911 1914-1918 WWI 1920s 1939-45 WWII Post WWII 1940s onwards 1950s and 60s 1970s 1991 1997-99 1999 2003 2003 2005 Flemish weavers Armenian merchants Jewish migrants begin to settle Greek War of Independence Germans, Greeks, Jews, “The Night Asylum of Manchester has Society for Really Deserving Greek Orthodox Church is Boom time, the population Salford Docks opens. Massive B.W. Levy, a Jewish man, Lithuanians, Poles and West 1911 Census: Refugees flee to the UK, eg. Polish Greek community in Refugees enter the UK as during the last War. Hitler’s Armenians from Cyprus, A flow of Greek Cypriots begin Lots of immigration from Caribbean Islands Greek Cypriot refugees arrive There is a substantial Refugees flee DR Congo Kosovan Albanian refugees Iraq Invasion by USA and The City agrees to take “In my culture, if it is raining and someone settle in settle and influence in Manchester and Salford. Many Christian Greeks flee and other communities are been open for about 4 years…In one of and Distressed Foreigners is built in Salford. There is a of Salford increases by success and influx of workers is given the freedom of the Ukrainians establish a club and 1,500 Germans in Manchester and Ukrainian in Manchester and Greater Manchester dictatorship causes an exodus of political and religious Iran, Iraq, Lebanon and Syria to settle following violence in Cyprus, and the Indian subcontinent, mainly settle in after Turkish invasion of Cyprus Jewish population in the in 1997 and 1999 arrive in Greater Manchester. -

Ashley and Morley Clan
The Ashley and Morley Clan Last Updated 2nd Septemberr 2020 ©2019, 2020 Ray Warburton Table of Contents Preface 2 Surnames 3 Descendants of John Warburton First Generation 4 Second Generation 5 Third Generation 7 Fourth Generation 14 Fifth Generation 20 Sixth Generation 34 Seventh Generation 53 Place Index 58 Person Index 69 1 PREFACE This clan documents a clan from Morley in Wilmslow and connects it to a family in Ashley within Bowdon parish that is descended from Josiah (died 1764) and Martha nee Bradbury. Josiah’s origins are uncertain but he is possibly the Josiah son of John who was baptised in Northenden in 1715. The Josiah name, which occurs throughout the clan, suggested that this clan is linked to the Hale Barns clan. However DNA shows it is unrelated, it being linked to the Nottinghamshire clan with a common ancestor who probably lived before 1600 AD. A number of links in the first couple of generations are 'most likely' rather than proven. Future DNA results might help here, though single mismatches might result from a non paternal event rather than signifying an error in the tree. Surnames B Bailey, Banks, Barlow, Barnes, Blease, Blinkhorn, Boon, Boulton, Bradbury, Bradley, Broadhurst, Burton C Cartwright, Cash, Culley D Davenport, Deakin, Dickenson E Eccles, Erlam F Fairhurst, Fallows, Faulkner, Finch, Fisher, Fletcher, Francis G Garner, Goubourn, Greenhalgh, Guest H Hamer, Harvey, Hawkins, Heaton, Henshaw, Hermon, Hobson, Holt, Hooley, Horton, Hulbert, Hyde J Jackson, Johnson, Jones, Joule M MacKay, Mayor, Morris O Oakes P Pearson, Price R Rawlins, Rickelton, Rigby, Robson, Rustage S Sadler, Sargeant, Saunders, Schofield, Sharman, Shaw, Smith, Swindells T Taberner, Telford, Thomason, Thompson, Tipping W Wallace, Warburton, Watkinson, Whitaker, Whittingham, Wilde, Wilkinson, Wilson, Worrall, Wright, Wylde Y Yates 3 Descendants of John Warburton First Generation 1. -
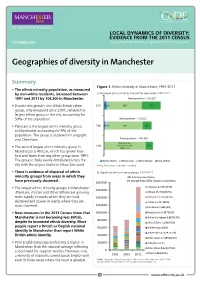
Geographies of Diversity in Manchester
LOCAL DYNAMICS OF DIVERSITY: EVIDENCE FROM THE 2011 CENSUS OCTOBER 2013 Prepared by ESRC Centre on Dynamics of Ethnicity (CoDE) Geographies of diversity in Manchester Summary Figure 1. Ethnic diversity in Manchester, 1991-2011 • The ethnic minority population, as measured by non-white residents, increased between a) Increased ethnic minority share of the population, 1991-2011 1991 and 2011 by 104,300 in Manchester. Total population – 503,127 • Despite this growth, the White British ethnic 2011 5% 2% 59% 33% group, only measured since 2001, remains the largest ethnic group in the city, accounting for 59% of the population. Total population – 422,922 • Pakistani is the largest ethnic minority group 2001 2% 4% 74% 19% in Manchester accounting for 9% of the population. The group is clustered in Longsight and Cheetham. Total population – 432,685 85% (includes 1991 White Other and 15% • The second largest ethnic minority group in White Irish Manchester is African, which has grown four- fold and faster than any other group since 1991. The group is fairly evenly distributed across the White Other White Irish White British Non-White city with the largest cluster in Moss Side ward. Notes: Figures may not add due to rounding. • There is evidence of dispersal of ethnic b) Growth of ethnic minority groups, 1991-2011 minority groups from areas in which they 2011 Census estimates (% change from 2001 shown in brackets): have previously clustered. 180,000 • The largest ethnic minority groups in Manchester Pakistani 42,904 (73%) 160,000 (Pakistani, African and Other White) are growing African 25,718 (254%) more rapidly in wards where they are least 140,000 Chinese 13,539 (142%) clustered and slower in wards where they are Indian 11,417 (80%) 120,000 most clustered. -
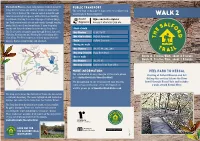
Walk 2 in Between
The Salford Trail is a new, long distance walk of about 50 public transport miles/80 kilometres and entirely within the boundaries The new way to find direct bus services to where you of the City of Salford. The route is varied, going through want to go is Route Explorer. rural areas and green spaces, with a little road walking walk 2 in between. Starting from the cityscape of Salford Quays, tfgm.com/route-explorer the Trail passes beside rivers and canals, through country Access it wherever you are. parks, fields, woods and moss lands. It uses footpaths, tracks and disused railway lines known as ‘loop lines’. Start of walk The Trail circles around to pass through Kersal, Agecroft, Bus Number 8, 26, 34-37 Walkden, Boothstown and Worsley before heading off to Salford Crescent Chat Moss. The Trail returns to Salford Quays from the Bus stop location historic Barton swing bridge and aqueduct. Train Salford Crescent Blackleach During the walk Country Park Bus Number 96, 97, 98, X41, X43 5 3 Clifton Country Park Bus stop location Bury New Road 4 Walkden Roe Green End of walk Route A. 5 miles/8km, about 2.5 hours Kersal Route B. 3 miles/5km, about 1.5 hours 2 Vale Bus Number 92, 93, 95 6 Worsley 7 Littleton Road Post Office Eccles Bus stop location Chat 1 Moss 8 Barton Swing Salford more information peel park to kersal 9 Bridge Quays For information on any changes in the route please Little Starting at Salford Museum and Art Woolden 10 go to visitsalford.info/thesalfordtrail Moss Gallery this section follows the River Irlam For background on the local history that you will Irwell through Kersal Vale and includes come across on the trail or for information on a walk around Kersal Moor. -

'After Housing Costs' Child Poverty Rate from Highest to Lowest
Notes: This spreadsheet ranks wards in Greater Manchester by their 'after housing costs' child poverty rate from highest to lowest. This is done using data published by End Child Poverty in 2019. The data also ranks areas based on the proportion of the population in a ward classified as black and minority ethnic (BAME) in census data. The higher the proportion of people who are BAME in a ward the higher the rank. This data shows that areas with the highest BAME populations in Greater Manchester are often the areas with the highest rates of child poverty. Local Ward GM Child poverty rank GM BAME authority area (after housing costs) rank Oldham Werneth 1 1 Oldham St Mary's 2 6 Oldham Coldhurst 3 3 Manchester Longsight 4 4 Salford Ordsall 5 48 Manchester Cheetham 6 9 Rochdale Central Rochdale 7 10 Manchester Hulme 8 16 Rochdale Milkstone and Deeplish 9 2 Manchester Gorton South 10 17 Rochdale Kingsway 11 23 Salford Broughton 12 47 Bolton Great Lever 13 13 Manchester Rusholme 14 11 Salford Kersal 15 82 Oldham Alexandra 16 25 Oldham Medlock Vale 17 22 Salford Irwell Riverside 18 55 Manchester Crumpsall 19 15 Manchester Ardwick 20 12 Manchester Bradford 21 29 Manchester Miles Platting and Newton Heath 22 52 Tameside St Peter's 23 30 Bolton Rumworth 24 7 Salford Langworthy 25 72 Manchester Gorton North 26 27 Bury Sedgley 27 56 Bolton Harper Green 28 37 Bolton Halliwell 29 20 Manchester Ancoats and Clayton 30 40 Rochdale Smallbridge and Firgrove 31 36 Manchester Levenshulme 32 18 Trafford Clifford 33 8 Manchester Moss Side 34 5 Manchester Fallowfield -

OFFICIAL DIRECTORY. 1927 Whalley Range Bowling Green Co
DIRECTORY. J OFFICIAL DIRECTORY. 1927 Whalley Range Bowling Green Co. Limited, Manchester Wheelers' Club, Demesne Road, Whalley Range. 8 .A..lbert Square, Trea.surer-E. O'Donnell Preaident-Fred Leeming Hon. SecretaT1J-Frerl T. Woolley, Thirlmere, Spring Bridge road Capt.ain-F. C. Lowcock Hon. Secretary-J. Viuson Steward-S. Keuworthy CHESS CLUBS. Cyclists' Touring Club, Manchester Chess Club, 23 Cros3 Street. 6 Bank Street. Pruident-J. Burgess lion. Secr~tary-W. Aruold Lmn~ll Via-President-A. Brodsky Y.M.C.A. Bicycle Club, Hon. Trea~urer-W. Lancaster Hon. &cretary-W. D. Bailey Ro by Schools, Ayto tin Street. Hon. LibrarU.tro-T. Kelly Hon. Secretary-H. Radford The Ladies' Chess Club. FOOTBALL CLUBS. Ttiesday at Pa.rker·s Restaurant, 12 St. Ann's square. Association Football Players Union. Pre1ident-Mrs. Brodsky lion, Sec-Mrs. Oltlharn, 33 Demesne road, A.lcxandra. park 14 St. Petet 's Square. Secretary-Herbert C. Broomfield North Manchester Chess Club, Manchester City Football Club Co. Limited, 50 Church Street, 32~ Hyde Road, .Aid wick, Hon. Secretary -II. L. Overt<Jn, 50 Church st Secretary-H. J. Newbould Y.M.C.A. Chess Club, Manchester Football Club, Roby Schools, .A.ytolln Street. Crown Hotel, Booth. Street. Hon. Secretary-Cffirdon Irwin Club Ground, Upper Chorlton Road, Whalley Range. Elon, Treasurer-F. S. Oppeuheim Hrm. &cretary-W. Parlaue CRICKET CLUBS AND GROUNDS. Manchester & District Cricket Association. Manchester United Football Club Lbnited, Bank Street, Clayton. County Cricket offices, 26 Barton Arcade, Deansgatc, Prc1ident-Ja.mes Horner Secreta1"]J-J. E. Mauguall Hon. Treruurer-E. 0. Swallow .Secretary-T. -

The Tudor Water Mill. By Peter James Corbally in 1543 Sir Robert
The Tudor Water Mill. by Peter James Corbally In 1543 Sir Robert Langley of Agecroft Hall, Lord of the Manor of Prestwich, built a weir across the River Irwell to provide water for a water mill. The weir was to raise the level of the river and pen back water that could be used to work the wheel at the mill. The weir was 20 yards long and 28 inches high above the river level raising the river level by an extra 24 inches. Presumably there was a mill race which led a forceful stream of water to the wheel. The mill and weir cost 300 marks to build and provided a profit of 40 marks per annum. It operated smoothly for four or so years. th Then on 20 June 1548, Thomas Holland, Lord of the Manor of Clifton came with six other men and broke down the end of the weir on the western bank. The water flowed out through the broken weir and the mill ceased operation. Truth to tell the western end of the weir rested on Thomas Holland’s land on the Clifton bank. Sir Robert Langley needed the co-operation of Thomas Holland in order to build the weir. The river must have been surveyed and the best spot for the weir must have rested on the Prestwich bank on the east and the Clifton bank on the west of the river. The two men, Sir Robert Langley and Thomas Holland, made a gentleman’s agreement about the weir five years earlier and Sir Robert, trusting Thomas Holland’s word, had gone ahead and built the project.