Mair227 001.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Andrea Doria
Desperate Hours Desperate Hours The Epic Rescue of the Andrea Doria Richard Goldstein John Wiley & Sons, Inc. Copyright © 2001 by Richard Goldstein. All rights reserved Published by John Wiley & Sons, Inc. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning, or otherwise, except as permitted under Section 107 or 108 of the 1976 United States Copyright Act, without either the prior written permission of the Publisher, or authorization through payment of the appropriate per-copy fee to the Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923 (978) 750-8400, fax (978) 750-4744. Requests to the Publisher for permission should be addressed to the Permissions Department, John Wiley & Sons, Inc., 605 Third Avenue, New York, NY 10158-0012 (212) 850-6011, fax (212) 850-6008, e-mail: [email protected]. This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is sold with the understanding that the pub- lisher is not engaged in rendering professional services. If professional advice or other expert assistance is required, the services of a competent professional person should be sought. This title is also available in print as ISBN 0-471-38934-X. Some content that ap- pears in the print version of this book may not be available in this electronic edition. For more information about Wiley products, visit our web site at www.Wiley.com For Nancy -
Chapter 3 Ship Compartmentation and Watertight Integrity
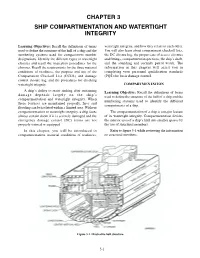
CHAPTER 3 SHIP COMPARTMENTATION AND WATERTIGHT INTEGRITY Learning Objectives: Recall the definitions of terms watertight integrity, and how they relate to each other. used to define the structure of the hull of a ship and the You will also learn about compartment checkoff lists, numbering systems used for compartment number the DC closure log, the proper care of access closures designations. Identify the different types of watertight and fittings, compartment inspections, the ship’s draft, closures and recall the inspection procedures for the and the sounding and security patrol watch. The closures. Recall the requirements for the three material information in this chapter will assist you in conditions of readiness, the purpose and use of the completing your personnel qualification standards Compartment Checkoff List (CCOL) and damage (PQS) for basic damage control. control closure log, and the procedures for checking watertight integrity. COMPARTMENTATION A ship’s ability to resist sinking after sustaining Learning Objective: Recall the definitions of terms damage depends largely on the ship’s used to define the structure of the hull of a ship and the compartmentation and watertight integrity. When numbering systems used to identify the different these features are maintained properly, fires and compartments of a ship. flooding can be isolated within a limited area. Without compartmentation or watertight integrity, a ship faces The compartmentation of a ship is a major feature almost certain doom if it is severely damaged and the of its watertight integrity. Compartmentation divides emergency damage control (DC) teams are not the interior area of a ship’s hull into smaller spaces by properly trained or equipped. -

Pennsylvania
Spring 1991 $1.50 Pennsylvania • The Keystone States Official Boating Magazine Viewpoint Recently we received a letter suggesting that we were being contradictory in Boat Pennsylvania. According to one reader, we suggested that boaters wear personal flota- tion devices, but that the magazine photographs don't always show their use. Obtaining photographs for a magazine can be a difficult proposition. Sometimes we stage situations and take the photographs ourselves. More often, we rely on photographs submitted by contributors. Photos that depict the general boating public often do not show people wearing PFDs simply because the incidence of wearing them is so low. If we were to say that we would only use photos that showed boaters wearing PFDs, we would have a difficult time fmding acceptable photos. Generally, we try to show people wearing PFDs in small boats in situations in which devices should obviously be worn. On large boats, people most often do not wear their PFDs. Should people wear PFDs? Statistics show that wearing a PFD can save your life. Are PFDs needed all the time? Because accidents happen when they are least expected, wearing a PFD all the time is a good idea. Practically, however, as comfortable as the newest PFDs are, they can be excruciating on a hot July day. Many boaters also want to get a little sun. We accept this and our statistics show that the chances of having an accident where a PFD would have been a factor are much lower in the summer months. Ofcourse, circumstances do exist in which wearing a PFD,even on the hottest day, is warranted. -

35 CFR Ch. I (7–1–98 Edition)
§ 109.5 35 CFR Ch. I (7±1±98 Edition) (b) The number of Canal deckhands not less than 100 square inches (645 to be placed on board a transiting ves- square centimeters) in areaÐpreferred sel to assist her crew in handling tow- dimensions are 12 x 9 inches (305 x 229 ing wires in the locks. millimeters)Ðand shall be capable of withstanding a strain of 100,000 pounds § 109.5 Ship's gear to be ready during (43,331 kilograms) on a towing wire transit; test. from any direction. Before beginning transit of the (e) Chocks designated as double Canal, a vessel shall have hawsers, chocks shall have a throat opening of lines and fenders ready for passing not less than 140 square inches (903 through the locks, for warping, towing, square centimeters) in areaÐpreferred or mooring as the case may be; and dimensions are 14 x 10 inches (356 x 254 shall have both anchors ready for let- millimeters)Ðand shall be capable of ting go. The Master shall assure him- withstanding a strain of 140,000 pounds self, by actual test, of the readiness of (64,000 kilograms) on the towing wires his vessel's main engines, steering from any direction. gear, engine room telegraphs, whistle, (f) Use of roller chocks is permissible rudder-angle and engine-revolution in- provided they are not less than 14.94 dicators, and anchors. During the tran- meters (49 feet) above the waterline at sit, at all times while a vessel is under- the vessel's maximum Panama Canal way or moored against the lock walls, draft and provided they are in good her deck winches, capstans, and other condition, meet all of the requirements power equipment for handling lines, as for solid chocks as specified in para- well as her mooring bitts, chocks, graphs (a), (b), (c), and (d) of this sec- cleats, hawse pipes, etc., shall be ready tion, as the case may be, and are so for handling the vessel, to the exclu- fitted that transition from the rollers sion of all other work. -
Record of Assessment Booklet of the OICNW Assessments
RECORD OF ASSESSMENT This record booklet can be used to document your completion of the proficiency assessments for Officer in Charge of the Navigational Watch (OICNW) in order to meet U.S. Coast Guard requirements for: Third Mate and OICNW Mate 1600 GRT and OICNW Mate 500 GRT and OICNW Quality Maritime Training 8601 4th Street N., Suite 209 St. Petersburg, FL 33702 Phone: (727) 209-1811 Toll Free: 1-800-581-5509 www.qualitymaritime.info RECORD OF ASSESSMENT This booklet can be used to document the seventy-nine (79) “Control Sheets” from U.S. Coast Guard CG-543 Policy Letter 11-07, which went into effect on July 1, 2011. The Assessment Control Sheets must be completed to meet U.S. Coast Guard and STCW requirements for an endorsement as Officer in Charge of a Navigation Watch On Vessels of 500 GT or more, which means the following: • Third Mate, Any Gross Tons Near Coastal/Oceans or; • Mate, 1600 GRT Near Coastal/Oceans or; • Mate, 500 GRT Near Coastal/Oceans The assessments of competency may be conducted aboard a seagoing vessel by a mariner who is serving on the vessel upon which the assessments are completed. The assessor must: Hold an STCW endorsement at the management level (STCW Regulation II/2-master or chief mate) valid for service on seagoing vessels of at least 200 GRT/500GT; OR Hold an STCW endorsement as OICNW (2nd Mate, 3rd Mate, or 500/1600 GRT Mate) and have at least one year of experience as OICNW on seagoing vessels of a least 200 GRT/500GT; OR Be serving on a seagoing military vessel of a least 200 GRT/500 GT and is either the Commanding Officer or Executive Officer or is authorized to conduct similar assessments for the U.S. -

1. 5. Name Two Important Rules to Be Followed to Write an Invitation Letter
FY BSC - NAUTICAT SCIENCE SUBJECT: ENGIISH AND COMMUNTCATTON SKtLt-S Q P CODE: 7437OO DATE OF EXAM: 22i{o NOVEMBER 20to 'Q. 1. 1. What does SMCP stands for? ANS: STANDARAD MARINE COMMUNTCATTON pHRASES 2. Who is a pilot? A pilot is someone who's an expert on a port, who ensures and helps the captain to dock the ship safely. Once his work is done; the pilot leaves the ship and goes to another one. 3. Name all the tenses Simple Present tense / simples past tense / simple future tense 4. Name 8 Message markers Ans: a. l.INSTRUCTION b. il. ADVTCE c. lll. WARNING d. IV.INFORMATION V. Question Vl. Answer Vll. Request Vlll. lntention 5. Define "Securite" Ans: lt is a distress safety signal given as a security warning to other ships or to port authorities. 5. Name two important rules to be followed to write an invitation letter 1. Invitation letters always should have a positive and polite tone 2. Always include special instructions which may help the guest when he comes to attend the function. 7. What is the definition of essay? Ans: The word Essay means an Attempt. Your attempt to write in a single prose-piece, using own ideas, impressions, thoughts, feelings or opinion on any given subject 8. What are the 2 important stratagies to be followed for Reaching Comprehension Ans: Skimming and scanning 9. Explain the meaning of Jettison Ans: Throwing overboard of goods in order to lighten the vessel or improve its stability in case of an emergency 10. What is the length of a shackle? 15 fathoms 11. -

Coast Guard Cutter Seamanship Manual
U.S. Department of Homeland Security United States Coast Guard COAST GUARD CUTTER SEAMANSHIP MANUAL COMDTINST M3120.9 November 2020 Commandant US Coast Guard Stop 7324 United States Coast Guard 2703 Martin Luther King Jr. Ave SE Washington, DC 20593-7324 Staff Symbol: (CG-751) Phone: (202) 372-2330 COMDTINST M3120.9 04 NOV 2020 COMMANDANT INSTRUCTION M3120.9 Subj: COAST GUARD CUTTER SEAMANSHIP MANUAL Ref: (a) Risk Management (RM), COMDTINST 3500.3 (series) (b) Rescue and Survival Systems Manual, COMDTINST M10470.10 (series) (c) Cutter Organization Manual, COMDTINST M5400.16 (series) (d) Naval Engineering Manual, COMDTINST M9000.6 (series) (e) Naval Ships' Technical Manual (NSTM), Wire and Fiber Rope and Rigging, Chapter 613 (f) Naval Ships’ Technical Manual (NSTM), Mooring and Towing, Chapter 582 (g) Cutter Anchoring Operations Tactics, Techniques, and Procedures (TTP), CGTTP 3-91.19 (h) Cutter Training and Qualification Manual, COMDTINST M3502.4 (series) (i) Shipboard Side Launch and Recovery Tactics, Techniques, and Procedures (TTP), CGTTP 3-91.25 (series) (j) Shipboard Launch and Recovery: WMSL 418’ Tactics, Techniques, and Procedures (TTP), CGTTP 3-91.7 (series) (k) Naval Ships’ Technical Manual (NSTM), Boats and Small Craft, Chapter 583 (l) Naval Ship’s Technical Manual (NSTM), Cranes, Chapter 589 (m) Cutter Astern Fueling at Sea (AFAS) Tactics, Techniques, and Procedures (TTP), CGTTP 3-91.20 (n) Helicopter Hoisting for Non-Flight Deck Vessels, Tactics, Techniques, and Procedures (TTP), CGTTP 3-91.26 (o) Flight Manual USCG Series -

Story on Page 3 Stoiy on Page 2
mnnmavi AWABDKO nnST PItlU • OCNfRAL EDlTOJITAt EXCtLUNCM • IMI • iNTERNATIONfAL LABOH PRESS OF AMERICA • OFFICIAL ORGAN OF THE SEAFARERS INTERNATIONAL UNION • ATLANTIC AND GULF DISTRICT • AFL-CIO • ^ ! I . 41 ^ I -Story On Page 3 Stoiy On Page 2 ' _ '^-1 I 'r ••T- KintM ^arat% Rican longshoremen ponder big job of moving CAfftiArilir B man to seek VWrjfW# ii2.ton turbine stator rig to nearby power plant after UOffTS jemonwy* higher seniority under SIU the stator was skidded off the Dorothy onto the dock in San Juan. It was put aboard contract's amended hiring rules, Joseph Scaturro, oiler in Baltimore after a rail trip from Pittsburgh. The huge mechanism was moved off (right), files papers as hq. patrolman Frank Bose looks without a hitch. (Story on Pago 7.) on. Changes start Oct. 1. (Story on Page 2). -:t.:: •;' fV..«j-' ' - f Pace Twe SEAFARERS LOG September 14, 1^5t SlU BrOSdSr shrimpers' Fete Seniority Hiring Clause Acknowledging a rise in shipping wd job opportunities for Seafarers, the SIU has won agreement from its contracted employers on a modification of Article 1 of the SIU contract, the seniority hiring ptoviaon.provision. Effective October 1 of'this year, all rated men with Class B seniority can qualify for class A seniority if they began ship Under the original coniract pro were required by the terms of the ping before January 1, 1952 vision, class A seniority was contract clause to accumulate 90 and have been sailing regularly granted to men who started with days seatime a year for eight years since that time. -

Readin' Both Pages
Readin’ Both Pages A membership publication of the Sail, Power & Steam Museum Vol. 1, No. 1 Winter 2008 Rekord ~ A Fascinating Freighter From the Memoirs of Capt. Jim Sharp Life is too short to own an ugly boat! That was my motto and I adhered to it with almost religious devotion. The next boat I was destined to drag into Camden Harbor was one interesting and handsome vessel. Although sailing was still very much my forte, this little ship conveyed the closest thing to worship of a power vessel that this old codger can conjure up. She was called the Record, spelled Rekord in old Norwegian, and was more than attractive in a thousand different ways. Rekord had history, intrigue, humor, challenge, personality and humility, all trunnelled together into one magnificent hull. Museum volunteers and staff were busy throughout the summer season working on many projects aboard Rekord. In this picture, Ben Breda applies fresh white paint to the starboard foredeck rail. Her ad was buried deep among the many listings in the “Yellow Pages” (that’s the scandal sheet of boats for sale shoe ... it was not bad. There was some worming, but noth- in the commercial world). I should never have taken my ing that would be a structural problem. And those worms copy into Fitzpatrick’s Deli to peruse the Boats For Sale would soon die in our cold Maine water. I think I knew I listings over my coffee. It was just a small picture and would buy this boat before even stepping aboard. Then I really fuzzy, but it snapped the hair-trigger on my snooping asked the owner about the engine. -

Service Requirements for Third Mate of Ocean Or Near-Coastal Self-Propelled Vessels
Coast Guard, DHS § 11.407 to 50 percent of the total required serv- (i) A minimum of 6 months service as ice. officer in charge of a deck watch on (3) Service on vessels to which STCW ocean self-propelled vessels. applies, whether inland or coastwise, (ii) Service on ocean self-propelled will be credited on a day-for-day basis. vessels as boatswain, able seaman, or (c) A person holding this endorse- quartermaster while holding a certifi- ment may qualify for an STCW en- cate or MMC endorsement as able sea- dorsement, according to § 11.305 of this man, which may be accepted on a two- part. for-one basis to a maximum allowable substitution of six months (12 months § 11.405 Service requirements for chief of experience equals 6 months of cred- mate of ocean or near-coastal self- propelled vessels of unlimited ton- itable service). nage. (b) Service towards an oceans, near- coastal or STCW endorsement will be (a) The minimum service required to credited as follows: qualify an applicant for an endorse- (1) Service on the Great Lakes will be ment as chief mate of ocean or near- credited on a day-for-day basis up to coastal self-propelled vessels of unlim- 100 percent of the total required serv- ited tonnage is 1 year of service as offi- ice. cer in charge of a navigational watch on ocean self-propelled vessels while (2) Service on inland waters, other holding a license or MMC endorsement than Great Lakes, that are navigable as second mate. waters of the United States, will be (b) Service towards an oceans, near- credited on a day-for-day basis for up coastal, or STCW endorsement will be to 50 percent of the total required serv- credited as follows: ice. -

The MARINER's MIRROR the JOURNAL of ~Ht ~Ocitt~ for ~Autical ~Tstarch
The MARINER'S MIRROR THE JOURNAL OF ~ht ~ocitt~ for ~autical ~tstarch. Antiquities. Bibliography. Folklore. Organisation. Architecture. Biography. History. Technology. Art. Equipment. Laws and Customs. &c., &c. Vol. III., No. 3· March, 1913. CONTENTS FOR MARCH, 1913. PAGE PAGE I. TWO FIFTEENTH CENTURY 4· A SHIP OF HANS BURGKMAIR. FISHING VESSELS. BY R. BY H. H. BRINDLEY • • 8I MORTON NANCE • • . 65 5. DocuMENTS, "THE MARINER's 2. NOTES ON NAVAL NOVELISTS. MIRROUR" (concluded.) CON· BY OLAF HARTELIE •• 7I TRIBUTED BY D. B. SMITH. 8S J. SOME PECULIAR SWEDISH 6. PuBLICATIONS RECEIVED . 86 COAST-DEFENCE VESSELS 7• WORDS AND PHRASES . 87 OF THE PERIOD I]62-I8o8 (concluded.) BY REAR 8. NOTES . • 89 ADMIRAL J. HAGG, ROYAL 9· ANSWERS .. 9I SwEDISH NAVY •• 77 IO. QUERIES .. 94 SOME OLD-TIME SHIP PICTURES. III. TWO FIFTEENTH CENTURY FISHING VESSELS. BY R. MORTON NANCE. WRITING in his Glossaire Nautique, concerning various ancient pictures of ships of unnamed types that had come under his observation, Jal describes one, not illustrated by him, in terms equivalent to these:- "The work of the engraver, Israel van Meicken (end of the 15th century) includes a ship of handsome appearance; of middling tonnage ; decked ; and bearing aft a small castle that has astern two of a species of turret. Her rounded bow has a stem that rises up with a strong curve inboard. Above the hawseholes and to starboard of the stem is placed the bowsprit, at the end 66 SOME OLD·TIME SHIP PICTURES. of which is fixed a staff terminating in an object that we have seen in no other vessel, and that we can liken only to a many rayed monstrance. -

Boston Harbor Auctions
Boston Harbor Auctions NAUTICAL ANTIQUE AND SHIP MODEL AUCTION Saturday - April 20, 2019 NAUTICAL ANTIQUE AND SHIP MODEL AUCTION 1: Samuel Walters Marine Painting USD 4,000 - 6,000 Fine, painting of the clipper ship Mary Moore by Samuel Walters. The vessel is shown under shortened sail, and carries a house flag and British flag. Large canvas. On sight 51 x 33. Overall 58 x 40. 2: Boston built tugboat painting USD 450 - 650 Oil painting of army tug DPC 16. Built by Lawley and Son, Neponset Mass in 1944. She was 86 feet long. Sold in 1946 as Gremlin, later Alice St. Philip and Honcho. Tug is shown in great detail. Rear of canvas states FINISHED 9/22/44. 26 X 19 3: George Lawley Painting USD 300 - 500 Painting originally from the George Lawley and Son shipyard in Boston. This is of the Lawley Built US Navy sub chaser launched at Neponset Mass 1943 and commissioned as USS PC 1087 painted in 1944 by Benjamin Stephenson. Signed lower right STEPHENSON. 31 x 20 4: Tropical naval ship landing painting USD 300 - 500 Original oil by Benjamin T. Stephenson. The reader of canvas reads: USS LCI 691, (center line ramp) titled EARLY MORNING LANDING OPERATION. Painted by Benjamin T. Stephenson 14 Longmeadow Road finished Oct 27, 1944. 31 x 20 5: Landing craft support LCS 1 Painting USD 250 - 450 Original oil painting showing a US Navy World War II LCS-1 landing craft ship underway. Back is marked with artists Benjamin T. Stephenson, 14 Longmeadow Road, Newton Corner, Massachusetts.