Comprehensive Test Menu | August 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Genes in Eyecare Geneseyedoc 3 W.M
Genes in Eyecare geneseyedoc 3 W.M. Lyle and T.D. Williams 15 Mar 04 This information has been gathered from several sources; however, the principal source is V. A. McKusick’s Mendelian Inheritance in Man on CD-ROM. Baltimore, Johns Hopkins University Press, 1998. Other sources include McKusick’s, Mendelian Inheritance in Man. Catalogs of Human Genes and Genetic Disorders. Baltimore. Johns Hopkins University Press 1998 (12th edition). http://www.ncbi.nlm.nih.gov/Omim See also S.P.Daiger, L.S. Sullivan, and B.J.F. Rossiter Ret Net http://www.sph.uth.tmc.edu/Retnet disease.htm/. Also E.I. Traboulsi’s, Genetic Diseases of the Eye, New York, Oxford University Press, 1998. And Genetics in Primary Eyecare and Clinical Medicine by M.R. Seashore and R.S.Wappner, Appleton and Lange 1996. M. Ridley’s book Genome published in 2000 by Perennial provides additional information. Ridley estimates that we have 60,000 to 80,000 genes. See also R.M. Henig’s book The Monk in the Garden: The Lost and Found Genius of Gregor Mendel, published by Houghton Mifflin in 2001 which tells about the Father of Genetics. The 3rd edition of F. H. Roy’s book Ocular Syndromes and Systemic Diseases published by Lippincott Williams & Wilkins in 2002 facilitates differential diagnosis. Additional information is provided in D. Pavan-Langston’s Manual of Ocular Diagnosis and Therapy (5th edition) published by Lippincott Williams & Wilkins in 2002. M.A. Foote wrote Basic Human Genetics for Medical Writers in the AMWA Journal 2002;17:7-17. A compilation such as this might suggest that one gene = one disease. -

WES Gene Package Multiple Congenital Anomalie.Xlsx
Whole Exome Sequencing Gene package Multiple congenital anomalie, version 5, 1‐2‐2018 Technical information DNA was enriched using Agilent SureSelect Clinical Research Exome V2 capture and paired‐end sequenced on the Illumina platform (outsourced). The aim is to obtain 8.1 Giga base pairs per exome with a mapped fraction of 0.99. The average coverage of the exome is ~50x. Duplicate reads are excluded. Data are demultiplexed with bcl2fastq Conversion Software from Illumina. Reads are mapped to the genome using the BWA‐MEM algorithm (reference: http://bio‐bwa.sourceforge.net/). Variant detection is performed by the Genome Analysis Toolkit HaplotypeCaller (reference: http://www.broadinstitute.org/gatk/). The detected variants are filtered and annotated with Cartagenia software and classified with Alamut Visual. It is not excluded that pathogenic mutations are being missed using this technology. At this moment, there is not enough information about the sensitivity of this technique with respect to the detection of deletions and duplications of more than 5 nucleotides and of somatic mosaic mutations (all types of sequence changes). HGNC approved Phenotype description including OMIM phenotype ID(s) OMIM median depth % covered % covered % covered gene symbol gene ID >10x >20x >30x A4GALT [Blood group, P1Pk system, P(2) phenotype], 111400 607922 101 100 100 99 [Blood group, P1Pk system, p phenotype], 111400 NOR polyagglutination syndrome, 111400 AAAS Achalasia‐addisonianism‐alacrimia syndrome, 231550 605378 73 100 100 100 AAGAB Keratoderma, palmoplantar, -

Coexpression of ATP-Binding Cassette Proteins ABCG5 and ABCG8 Permits Their Transport to the Apical Surface
Coexpression of ATP-binding cassette proteins ABCG5 and ABCG8 permits their transport to the apical surface Gregory A. Graf, … , Jonathan C. Cohen, Helen H. Hobbs J Clin Invest. 2002;110(5):659-669. https://doi.org/10.1172/JCI16000. Article Cardiology Mutations in either ATP-binding cassette (ABC) G5 or ABCG8 cause sitosterolemia, an autosomal recessive disorder of sterol trafficking. To determine the site of action of ABCG5 and ABCG8, we expressed recombinant, epitope-tagged mouse ABCG5 and ABCG8 in cultured cells. Both ABCG5 and ABCG8 underwent N-linked glycosylation. When either protein was expressed individually in cells, the N-linked sugars remained sensitive to Endoglycosidase H (Endo H). When ABCG5 and ABCG8 were coexpressed, the attached sugars were Endo H–resistant and neuraminidase-sensitive, indicating that the proteins were transported to the trans-Golgi complex. The mature, glycosylated forms of ABCG5 and ABCG8 coimmunoprecipitated, consistent with heterodimerization of these two proteins. The Endo H–sensitive forms of ABCG5 and ABCG8 were confined to the endoplasmic reticulum (ER), whereas the mature forms were present in non-ER fractions in cultured hepatocytes. Immunoelectron microscopy revealed ABCG5 and ABCG8 on the plasma membrane of these cells. In polarized WIF-B cells, recombinant ABCG5 localized to the apical (canalicular) membrane when coexpressed with ABCG8, but not when expressed alone. To our knowledge this is the first direct demonstration that trafficking of an ABC half-transporter to the cell surface requires the presence of its dimerization partner. Find the latest version: https://jci.me/16000/pdf Coexpression of ATP-binding cassette See the related Commentary beginning on page 605. -

'Sitosterolemia—10 Years Observation in Two Sisters'
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2019 Sitosterolemia—10 years observation in two sisters Veit, Lara ; Allegri Machado, Gabriella ; Bürer, Céline ; Speer, Oliver ; Häberle, Johannes Abstract: Familial hypercholesterolemia due to heterozygous low‐density lipoprotein‐receptor mutations is a common inborn errors of metabolism. Secondary hypercholesterolemia due to a defect in phytosterol metabolism is far less common and may escape diagnosis during the work‐up of patients with dyslipi- demias. Here we report on two sisters with the rare, autosomal recessive condition, sitosterolemia. This disease is caused by mutations in a defective adenosine triphosphate‐binding cassette sterol excretion transporter, leading to highly elevated plant sterol concentrations in tissues and to a wide range of symp- toms. After a delayed diagnosis, treatment with a diet low in plant lipids plus ezetimibe to block the absorption of sterols corrected most of the clinical and biochemical signs of the disease. We followed the two patients for over 10 years and report their initial presentation and long‐term response to treatment. DOI: https://doi.org/10.1002/jmd2.12038 Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-182906 Journal Article Accepted Version Originally published at: Veit, Lara; Allegri Machado, Gabriella; Bürer, Céline; Speer, Oliver; Häberle, Johannes (2019). Sitosterolemia— 10 years observation in -

Clinical Utility Gene Card For: Sitosterolaemia
European Journal of Human Genetics (2017) 25, doi:10.1038/ejhg.2016.187 & 2017 Macmillan Publishers Limited, part of Springer Nature. All rights reserved 1018-4813/17 www.nature.com/ejhg CLINICAL UTILITY GENE CARD Clinical utility gene card for: Sitosterolaemia Amanda J Hooper1,2,3, Damon A Bell1,2, Robert A Hegele4 and John R Burnett*,1,2 European Journal of Human Genetics (2017) 25, doi:10.1038/ejhg.2016.187; published online 28 December 2016 1. DISEASE CHARACTERISTICS Japanese and Indian patients with sitosterolaemia (20% of known cases), 1.1 Name of the disease (synonyms) it is mainly owing to ABCG5 mutations.4 On the basis of allele Sitosterolaemia (phytosterolaemia; Mediterranean stomatocytosis/ frequencies of loss-of-function variants (frameshift, nonsense and macrothrombocytopenia). splicing only; not missense) in the ExAC database, sitosterolaemia has a global prevalence of at least 1 in 2.6 million for ABCG5 and 1 in 1.2 OMIM# of the disease 360 000 for ABCG8; the most common loss-of-function variant 210250. appears to be ABCG8 c.1083G4A (p.(Trp361Ter)) (Exome Aggrega- tion Consortium; http://exac.broadinstitute.org/) 1.3 Name of the analysed genes or DNA/chromosome segments ABCG5 ABCG8 , . 1.9 Diagnostic setting 1.4 OMIM# of the gene(s) 605459, 605460. Yes No. A. (Differential) diagnostics ⊠ □ 1.5 Mutational spectrum B. Predictive testing □ ⊠ □ ⊠ The sitosterolaemia genes ABCG5 (NM_022436.2) and ABCG8 C. Risk assessment in relatives □ ⊠ (NM_022437.2) lie ‘head to head’ on chromosome 2.1–3 They each D. Prenatal contain 13 exons and encode a half-transporter (sterolin-1 and sterolin-2, respectively), with the C-terminus only containing 6 of Comment: Use of genetic testing is essentially limited to confirmatory 3 the usual 12 transmembrane domains of the other ABC transporters. -

Sitosterolemia: Twenty Years of Discovery of the Function of ABCG5ABCG8
University of Kentucky UKnowledge Pharmaceutical Sciences Faculty Publications Pharmaceutical Sciences 3-5-2021 Sitosterolemia: Twenty Years of Discovery of the Function of ABCG5ABCG8 Kori Williams University of Kentucky, [email protected] Allison Segard University of Kentucky, [email protected] Gregory A. Graf University of Kentucky, [email protected] Right click to open a feedback form in a new tab to let us know how this document benefits ou.y Follow this and additional works at: https://uknowledge.uky.edu/ps_facpub Part of the Medical Molecular Biology Commons, and the Pharmacy and Pharmaceutical Sciences Commons Sitosterolemia: Twenty Years of Discovery of the Function of ABCG5ABCG8 Digital Object Identifier (DOI) https://doi.org/10.3390/ijms22052641 Notes/Citation Information Published in International Journal of Molecular Sciences, v. 22, issue 5, 2641. © 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/). This review is available at UKnowledge: https://uknowledge.uky.edu/ps_facpub/159 International Journal of Molecular Sciences Review Sitosterolemia: Twenty Years of Discovery of the Function of ABCG5 ABCG8 Kori Williams 1, Allison Segard 1 and Gregory A. Graf 1,2,3,* 1 Department of Pharmaceutical Sciences, College of Pharmacy, University of Kentucky, Lexington, KY 40536, USA; [email protected] (K.W.); [email protected] (A.S.) 2 Saha Cardiovascular Research Center, Lexington, KY 40536, USA 3 Barnstable Brown Diabetes and Obesity Center, Lexington, KY 40536, USA * Correspondence: [email protected]; Tel.: +1-859-797-2463 Abstract: Sitosterolemia is a lipid disorder characterized by the accumulation of dietary xenosterols in plasma and tissues caused by mutations in either ABCG5 or ABCG8. -

Cholesterol and Saturated Fat Intake Determine the Effect Of
article September 2006 ⅐ Vol. 8 ⅐ No. 9 Cholesterol and saturated fat intake determine the effect of polymorphisms at ABCG5/ABCG8 genes on lipid levels in children Enrique Viturro, PhD1, Manuel de Oya, PhD, MD1, Miguel A. Lasuncio´n, PhD2, Lydia Gorgojo, PhD, MD3, Jose´ M. Martı´n Moreno, PhD, MD3, Mercedes Benavente, PhD1, Beatriz Cano, PhD1, and Carmen Garces, PhD1 Purpose: Analysis of mutations in genes of the cholesterol metabolic pathway has not completely explained the interindividual variability of blood cholesterol concentrations attributed to gene–nutrient interactions. Thus, we analyzed polymorphisms in the ABCG5 and ABCG8 genes, involved in the regulation of intestinal cholesterol absorption, with special interest in a potential interaction with diet to determine lipid levels. Methods: The polymorphisms ABCG5 C1950G (Gln604Glu) and ABCG8 C1895T (Ala640Val) were determined by polymerase chain reaction and restriction analysis in 1227 healthy school children, aged 6 to 8 years. Results: No significant differences were found in blood lipid levels between subjects with different genotypes of the two analyzed polymorphisms. However, important differences appeared when separating subjects by their different lipid intake. The presence of the ABCG8 C1895T and ABCG5 C1950G polymorphisms was associated with different plasma total cholesterol, low-density lipoprotein cholesterol complex, and apolipoprotein B levels only in low-cholesterol consumers (significantly for the C1895T polymorphism), and among children within the lower tertile of saturated fat intake (significantly for the C1950G polymorphism). Conclusion: Polymorphisms at the half-transporter ABCG5 and ABCG8 genes affect blood cholesterol concentrations in prepubertal children by influencing dietary respon- siveness. This highly significant gene–nutrient interaction could explain the great individual differences in the plasma lipid response to cholesterol and fat intake. -

Blueprint Genetics Comprehensive Hematology and Hereditary Cancer
Comprehensive Hematology and Hereditary Cancer Panel Test code: HE1401 Is a 348 gene panel that includes assessment of non-coding variants. Is ideal for patients with a clinical suspicion of hematological disorder with genetic predisposition to malignancies. This panel is designed to detect heritable germline mutations and should not be used for the detection of somatic mutations in tumor tissue. Is not recommended for patients suspected to have anemia due to alpha-thalassemia (HBA1 or HBA2). These genes are highly homologous reducing mutation detection rate due to challenges in variant call and difficult to detect mutation profile (deletions and gene-fusions within the homologous genes tandem in the human genome). Is not recommended for patients with a suspicion of severe Hemophilia A if the common inversions are not excluded by previous testing. An intron 22 inversion of the F8 gene is identified in 43%-45% individuals with severe hemophilia A and intron 1 inversion in 2%-5% (GeneReviews NBK1404; PMID:8275087, 8490618, 29296726, 27292088, 22282501, 11756167). This test does not detect reliably these inversions. Is not recommended for patients suspected to have anemia due to alpha-thalassemia (HBA1 or HBA2). These genes are highly homologous reducing mutation detection rate due to challenges in variant call and difficult to detect mutation profile (deletions and gene-fusions within the homologous genes tandem in the human genome). About Comprehensive Hematology and Hereditary Cancer Inherited hematological diseases are a group of blood disorders with variable clinical presentation. Many of them predispose to malignancies and for example patients with inherited bone marrow failure syndromes (Fanconi anemia) have a high risk of developing cancer, either leukemia or solid tumors. -

Download CGT Exome V2.0
CGT Exome version 2. -

Predisposing Factors for Adrenal Insufficiency
The new england journal of medicine review article CURRENT CONCEPTS Predisposing Factors for Adrenal Insufficiency Stefan R. Bornstein, M.D. From the Department of Medicine, Tech- drenal insufficiency — the clinical manifestation of deficient nical University of Dresden, Dresden, Ger- production or action of glucocorticoids — is a life-threatening disorder that many. Address reprint requests to Dr. Bornstein at the Department of Medicine, may result from either primary adrenal failure or secondary adrenal disease Technical University of Dresden, Fetscher- A 1,2 due to impairment of the hypothalamic–pituitary axis. This article focuses on pro- str. 74, 01307 Dresden, Germany, or at viding the practicing clinician with new insights into predisposing factors for adre- [email protected]. nal insufficiency. When and during what situations should a clinician suspect ad- N Engl J Med 2009;360:2328-39. renal insufficiency? What genetic disorders, infections, and medications should be Copyright © 2009 Massachusetts Medical Society. considered? What are the current views on the underlying mechanisms? The cardinal clinical symptoms of adrenocortical insufficiency, as first described by Thomas Addison in 1855,3 include weakness, fatigue, anorexia, and abdominal pain, with orthostatic hypotension, salt craving, and characteristic hyperpigmenta- tion of the skin occurring with primary adrenal failure. The acute syndrome con- stitutes a medical emergency since it may result in a severe hypotensive crisis and clouded sensorium, together with pain in the muscles, joints, or abdomen and fever.1,2 In the diagnostic workup for the disorder, the capacity of the adrenal cortex to respond to corticotropin is tested with the use of the standard short corticotropin test, which measures the serum cortisol level before and 30 or 60 minutes after an intravenous or intramuscular injection of 250 μg of corticotropin.4 An increase in the serum cortisol level to peak concentrations above 500 nmol per liter (18 μg per deciliter) indicates a normal response. -
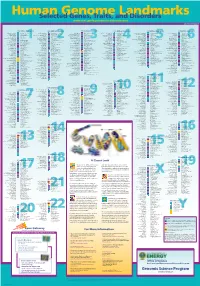
Genomeposter2009.Pdf
Fold HumanSelected Genome Genes, Traits, and Landmarks Disorders www.ornl.gov/hgmis/posters/chromosome genomics.energy. -

Β-Sitosterolemia and Xanthomatosis: a NEWLY DESCRIBED LIPID STORAGE DISEASE in TWO SISTERS
β-Sitosterolemia and Xanthomatosis: A NEWLY DESCRIBED LIPID STORAGE DISEASE IN TWO SISTERS Ashim K. Bhattacharyya, William E. Connor J Clin Invest. 1974;53(4):1033-1043. https://doi.org/10.1172/JCI107640. Although the usual diet may contain 150-250 mg of plant sterols, chiefly β-sitosterol, only trace amounts of these sterols have heretofore been found in human or animal blood and tissues. We now report elevated plant sterol levels in the blood and tissues of two sisters with extensive tendon xanthomas but normal plasma cholesterol levels. Besides β- sitosterolemia and xanthomatosis, no other physical, mental, or biochemical abnormalities were detected. Repeatedly, the plasmas of the two sisters have contained 27.1 and 17.7 mg/100 ml of β-sitosterol, 9.7 and 8.2 mg/100 ml of campesterol, and 0.5 and 0.5 mg/100 ml of stigmasterol, respectively. These plant sterols constituted 15.6 and 11.3% of the total plasma sterols. Some 60% of the plasma β-sitosterol and campesterol was esterified; the measurable stigmasterol was entirely unesterified. The transport of the plasma β-sitosterol and campesterol was largely in low density lipoproteins (76 and 83%, respectively). High density lipoproteins carried the remainder. Plant sterols were barely detectable in the very low density lipoprotein fraction. Only trace amounts of stigmasterol could be detected in the low density and high density lipoprotein fractions. The plant sterol content of the red blood cells averaged 12-13 mg/100 ml packed cells or about 13% of the total sterols. Two tendon xanthoma biopsies with the usual high concentration of cholesterol had 36.7 and 4.0 mg of plant […] Find the latest version: https://jci.me/107640/pdf i-Sitosterolemia and Xanthomatosis A NEWLY DESCRIBED LIPID STORAGE DISEASE IN TWO SISTERS ASHM K.