The Making of British Bioethics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Acknowledgements
Acknowledgements The cataloguing of the Manchester Medical Collections was made possible by a grant from the fund for Research Resources for Medical History set up by the Wellcome Trust. We are indebted to the Wellcome Trust for its continuing support for the history of medicine in The University of Manchester. Many colleagues and friends have helped to bring this volume to completion.We are grateful to all the contributors for their patience and forbearance during the long editing process. Dr Dorothy Clayton guided us expertly through the production of the volume and took much of the pain from that process. Many of the papers feature images taken from the JRUL collections and we would like to thank Carol Burrows for help with the selection and production of these illustrations. We are grateful to the following for permission to reproduce images: L'Institut Pasteur, p. 102; Tameside Local Studies and Archives Centre, Central Library, Ashton-under-Lyne, pp. 89, 105; The Royal Society, p. 159; The Medical Illustration Unit, Manchester Royal Infirmary, pp. 170, 172, 177, 178, 180; Anthony Bentley, Scientific Photographer, Faculty of Life Sciences, The University of Manchester, pp. 217, 218, 219 and 220. All other illustrations were taken from the collections held by the John Rylands University Library. John Pickstone Stella Butler 7 Contributors Julie Anderson is a Research Fellow at the Centre for the History of Science,Technology and Medicine and the Wellcome Unit for the History of Medicine at The University of Manchester. Her areas of research include the history of disability and she has published on physical disability and war. -

Public Services Ombudsmen. This Consultation
The Law Commission Consultation Paper No 196 PUBLIC SERVICES OMBUDSMEN A Consultation Paper ii THE LAW COMMISSION – HOW WE CONSULT About the Law Commission The Law Commission was set up by section 1 of the Law Commissions Act 1965 for the purpose of promoting the reform of the law. The Law Commissioners are: The Rt Hon Lord Justice Munby (Chairman), Professor Elizabeth Cooke, Mr David Hertzell, Professor David Ormerod1 and Miss Frances Patterson QC. The Chief Executive is: Mr Mark Ormerod CB. Topic of this consultation This consultation paper deals with the public services ombudsmen. Impact assessment An impact assessment is included in Appendix A. Scope of this consultation The purpose of this consultation is to generate responses to our provisional proposals. Duration of the consultation We invite responses from 2 September 2010 to 3 December 2010. How to respond By email to: [email protected] By post to: Public Law Team, Law Commission, Steel House, 11 Tothill Street, London, SW1H 9LJ Tel: 020-3334-0262 / Fax: 020-3334-0201 If you send your comments by post, it would be helpful if, wherever possible, you could send them to us electronically as well (for example, on CD or by email to the above address, in any commonly used format. After the consultation In the light of the responses we receive, we will decide our final recommendations and we will present them to Parliament. It will be for Parliament to decide whether to approve any changes to the law. Code of Practice We are a signatory to the Government’s Code of Practice on Consultation and carry out our consultations in accordance with the Code criteria (set out on the next page). -

A Guide to the Government for BIA Members
A guide to the Government for BIA members Correct as of 26 June 2020 This is a briefing for BIA members on the Government led by Boris Johnson and key ministerial appointments for our sector after the December 2019 General Election and February 2020 Cabinet reshuffle. Following the Conservative Party’s compelling victory, the Government now holds a majority of 80 seats in the House of Commons. The life sciences sector is high on the Government’s agenda and Boris Johnson has pledged to make the UK “the leading global hub for life sciences after Brexit”. With its strong majority, the Government has the power to enact the policies supportive of the sector in the Conservatives 2019 Manifesto. All in all, this indicates a positive outlook for life sciences during this Government’s tenure. Contents: Ministerial and policy maker positions in the new Government relevant to the life sciences sector .......................................................................................... 2 Ministers and policy maker profiles................................................................................................................................................................................................ 7 Ministerial and policy maker positions in the new Government relevant to the life sciences sector* *Please note that this guide only covers ministers and responsibilities relevant to the life sciences and will be updated as further roles and responsibilities are announced. Department Position Holder Relevant responsibility Holder in -

Download Clinton Email November Release
UNCLASSIFIED U.S. Department of State Case No. F-2014-20439 Doc No. C05772613 Date: 11/30/2015 RELEASE IN FULL CONFIDENTIAL October 9, 2010 For: Hillary From: Sid Re: Yes, some things: 1. Richard Wolff told me that one of the reasons Jones was summarily executed was payback for dumping Mark Lippert (whom he called "Thing Two," from Dr. Seuss' Cat in the Hat), McDonough's sidekick (whom Jones calls "Thing One"). Of course, Jones had to go to Obama himself to dispose of Lippert. The true cause was that Thing One and Thing Two were leaking negative stories about Jones. McDonough, naturally, has assumed Donilon's post. Obladi, oblada, as John Lennon (who would have been 70) might say. 2. Shaun Woodward is in the Labour shadow cabinet in his former position as Secretary of State for Northern Ireland. Gordon Brown's hatchetman, Charlie Whelan, whose job was to undercut Tony, had worked the unions to vote for Ed Miliband rather than Ed Balls (the one closest to Gordon) in order to beat David--the last scene in the revenge tragedy of Gordon v. Tony. Only 19 percent of the union people voted, but were credited with the full one-third of Labour votes for leader selection, so a minority of a minority threw the election by 1.3 percent to Ed. Then Balls, his wife Yvette Cooper (an MP and former cabinet secretary), and other Brownites ran as a slate for shadow cabinet--the first time the shadow cabinet was to be elected by the constituency. That succeeded to electing them all and shutting out Peter Hain, the former deputy PM, as well as Shaun. -

Glover, Jonathan. Humanity: a Moral History of the Twentieth Century
Glover, Jonathan. Humanity: A Moral History of the Twentieth Century. New Haven, Connecticut: Yale University Press: 2000. Jonathan Glover (1941-____ A.D.) directs the Centre of Medical Law and Ethics at King’s College, London. Preface. What lessons in ethics ought one to derive from the violence of the twentieth century? Chapter 1: Never Such Innocence Again. At the end of the twentieth century, one cannot be certain of the existence of a moral law or of moral progress. Intellectual repudiation of moral law and last century’s history argue against them. News tends to anesthetize viewers to events. Everything gets forgotten in the endless news cycle. Glover has not experienced the events of which he writes. He is attempting to get perspective on them. In philosophical ethics, there has been a move from theoretical ethics to applied ethics, putting human concerns squarely in philosophy’s crosshairs. Ethics generally should be more empirical. Enlightenment confidence that rationality would banish war and cruelty proved shallow. Glover looks at human spiritual darkness, in the hope of restraining it in the service of a better future. PART ONE: ETHICS WITHOUT THE MORAL LAW Chapter 2: Nietzsche’s Challenge. Friedrich Nietzsche foresaw the collapse of religious morality in the twentieth century. Nietzsche valued self-creation, and castigated all authorities that might claim to govern or restrain that project. God is dead. Religion is poison and must be swept away. Governments rely on confusions of the masses. A self-created man is noble in the sense that his superior completeness frees him to do whatever he may need in order to self-create. -

Yougov / the Sunday Times Survey Results
YouGov / The Sunday Times Survey Results Sample Size: 1011 Labour Party Members Fieldwork: 7th - 9th September 2010 1st Preference - September 2010 1st Preference - July 2010 September Choice July Choice Gender Age Diane Andy David Ed Diane Andy David Ed David Ed David Ed Total Ed Balls Ed Balls Male Female 18-34 35-54 55+ Abbott Burnham Miliband Miliband Abbott Burnham Miliband Miliband Miliband Miliband Miliband Miliband Weighted Sample 1008 106 86 91 354 287 99 45 65 244 209 431 474 320 340 577 432 331 303 374 Unweighted Sample 1011 102 89 97 344 296 93 45 69 239 221 429 485 310 353 654 357 307 317 387 % %%%%%%%%%%%%%%%%%%% 1st Preference - September 2010 [Excluding Don't know and Wouldn't Vote] David Miliband 38 0001000824 9 79 16 83 0 68 11 36 42 41 39 35 Ed Miliband 31 00001001114 13 11 69 1 62 11 50 31 31 33 28 33 Diane Abbott 11 1000000702 3144164181112131111 Andy Burnham 10 001000029 66 4 6 7 10 10 10 12 7 8 10 11 Ed Balls 9 0100000852 10 5 6 5 12 7 11 10 8 5 13 10 Weighted Sample 846 92 82 84 320 268 84 41 55 214 186 384 427 279 296 493 353 280 258 308 Unweighted Sample 849 90 85 89 308 277 80 41 58 207 199 380 438 268 309 555 294 260 266 323 %%%%%%%%%%%%%%%%%%%% 2nd Preference - September 2010 [Excluding Don't know and Wouldn't Vote] Ed Miliband 30 53 48 34 43 0 42 32 25 33 22 35 27 30 29 29 32 32 33 26 Ed Balls 22 200 2825251936 26 23 21 23 21 24 22 23 21 20 23 23 Andy Burnham 19 14 17 0 21 24 14 18 19 21 18 19 19 19 18 18 20 21 20 16 David Miliband 17 13 20 30 0 35 13 12 24 10 27 13 21 16 20 17 17 15 12 23 Diane Abbott 11 0 15 8 11 16 11 2 7 12 12 9 12 11 11 12 10 12 11 12 Weighted Sample 905 90 74 75 351 285 82 40 56 233 203 431 474 299 319 519 387 303 267 336 Unweighted Sample 914 87 78 84 341 293 79 40 60 228 214 429 485 290 334 592 322 283 280 351 %%%%%%%%%%%%%%%%%%%% Miliband preference - September [Excluding definitely wouldn't vote] David Miliband 48 19 28 41 100 1 25 34 37 86 17 100 0 80 17 47 49 48 46 48 Ed Miliband 52 81 72 59 0 99 75 66 63 14 83 0 100 20 83 53 51 52 54 52 1 © 2010 YouGov plc. -

Particularitiesof Tony Blair' Governments'foreign Policy Decision
Максим Прихненко . Особливості механізму прийняття зовнішньополітичних рішень … 321 Історико -політичні проблеми сучасного світу : Modern Historical and Political Issues: Збірник наукових статей . – Чернівці : Journal in Historical & Political Sciences. – Chernivtsi: Чернівецький національний університет , Chernivtsi National University, 2016. – Т. 33-34. – С. 321-327 2016. – Volume. 33-34. – pp. 321-327 УДК : 32-327(410) © Максим Прихненко 1 Особливості механізму прийняття зовнішньополітичних рішень в урядах Тоні Блера В статті системно проаналізовано модель прийняття зовнішньополітичних рішень , а також ключові фактори , які впливали на формування та впровадження цих рішень у зовнішньополіти- чний курс Великобританії у якості складової частини загальної моделі лідерства Тоні Блера . Ключові слова Модель лідерства , механізм прийняття рішень , блеризм . Particularitiesof Tony Blair’ governments’foreign policy decision-making process The present article is devoted to the problem of particularities of Tony Blair’ governments’ foreign policy decision-making process. The aim of the paper is to analyze the decision-making model formed by Tony Blair as well as to identify key factors which impacted the process of creation and implemen- tation of foreign policy decisions in the framework of Tony Blair’ leadership model. It was concluded that Tony Blair had formed tree level decision-making system. Rolls of the Parliament and the Gov- ernment in the deliberation process were frustrated. On the other hand, special advisers and so called selective committees impacts were strengthened. This institutes played the role of consulting bodies on specific issues of the agenda. Prime Minister and Minister of Foreign Affairs were the driving force of all process. But usually the second one was like the executor of Prime Minister’ decision. -
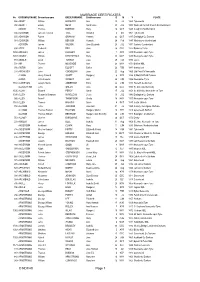
MARRIAGE CERTIFICATES © NDFHS Page 1
MARRIAGE CERTIFICATES No GROOMSURNAME Groomforename BRIDESURNAME Brideforename D M Y PLACE 588 ABBOT William HADAWAY Ann 25 Jul 1869 Tynemouth 935 ABBOTT Edwin NESS Sarah Jane 20 JUL 1882 Wallsend Parrish Church Northumbrland ADAMS Thomas BORTON Mary 16 OCT 1849 Coughton Northampton 556 ADAMSON James Frederick TATE Annabell 6 Oct 1861 Tynemouth 655 ADAMSON Robert GRAHAM Hannah 23 OCT 1847 Darlington Co Durham 581 ADAMSON William BENSON Hannah 24 Feb 1847 Whitehaven Cumberland ADDISON James WILSON Jane Elizabeth 23 JUL 1871 Carlisle, Cumberland 694 ADDY Frederick BELL Jane 26 DEC 1922 Barnsley Yorks 1456 AFFLECK James LUCKLEY Ann 1 APR 1839 Newcastle upon Tyne 1457 AGNEW William KIRKPATRICK Mary 30 MAY 1887 Newcastle upon Tyne 751 AINGER David TURNER Eliza 28 FEB 1870 Essex 704 AIR Thomas MCKENZIE Ann 24 MAY 1871 Belford NBL 936 AISTON John ELLIOTT Esther 26 FEB 1881 Sunderland 244 AITCHISON John COCKBURN Jane 22 Aug 1865 Utd Pres Ch Newcastle ALBION Henry Edward SCOTT Margaret 6 APR 1884 St Mark Millfield Durham ALDER John Cowens WRIGHT Ann 24 JUN 1856 Newcastle /Tyne 1160 ALDERSON Joseph Henry ANDERSON Eliza 22 JUN 1897 Heworth Co Durham ALLABURTON John GREEN Jane 24 DEC 1842 St. Giles ,Durham City 1505 ALLAN Edward PERCY Sarah 17 JUL 1854 St. Nicholas, Newcastle on Tyne 1390 ALLEN Alexander Bowman WANDLESS Jessie 10 JUL 1943 Darlington Co Durham 992 ALLEN Peter F THOMPSON Sheila 18 MAY 1957 Newcastle upon Tyne 1161 ALLEN Thomas HIGGINS Annie 4 OCT 1887 South Shields 158 ALLISON John JACKSON Jane Ann 31 Jul 1859 Colliery, Catchgate, -

Inhuman Wrongs Crimes Against Humanity in Theory, Law, and Politics
Inhuman Wrongs Crimes against Humanity in Theory, Law, and Politics Goya, Third of May 1808 Government 94gl* Professor Cheryl Welch Fall 2016 [email protected] Thursday 2:00-4:00 617.495.5855 CGIS Knafel Building– K108 CGIS K151A Office Hours: by appointment Course Description This course examines the notion of a crime against humanity from the perspectives of moral theory, history, and contemporary international law and politics. After considering some philosophical perspectives on abuses whose wrongness has been termed “morally over- determined,” we turn to nineteenth-century cases of so-called scandals against humanity: slavery and expulsion or extermination of conquered peoples. We then trace the emergence of the concept of crimes against humanity in the twentieth century as a category of international crime at the intersection of human rights and humanitarian law and examine debates over the legalization offenses that “shock the conscience.” Finally, we turn to philosophical and political debates surrounding the prevention and prosecution of some contemporary crimes against humanity. *This course counts as a Government seminar or elective. It also counts toward the secondary concentration in Ethnicity, Migration, and Rights. Welch 94gl - fall 2016 - page 1 of 6 Course Requirements 1. Class participation (30% of grade) • Blog posts: Students are expected to have done the readings and to come to the seminar prepared to discuss them. Before each class (except for the class in which you are presenting), you will be expected to post a short response to the reading. Posts are due on Canvas by 8 am on Thursday morning. First post is due on Thurs., Sept. -

The Parliamentary Ombudsman: Firefighter Or Fire-Watcher?
12 The Parliamentary Ombudsman: Firefi ghter or fi re-watcher? Contents 1. In search of a role 2. The PCA’s offi ce 3. From maladministration to good administration 4. Firefi ghting or fi re-watching? (a) The small claims court (b) Ombudsmen and courts (c) Fire-watching: Inspection and audit 5. Inquisitorial procedure (a) Screening (b) Investigation (c) Report 6. The ‘Big Inquiry’ (a) Grouping complaints: The Child Support Agency (b) Political cases 7. Occupational pensions: Challenging the ombudsman 8. Control by courts? 9. Conclusion: An ombudsman unfettered? 1. In search of a role In Chapter 10, we considered complaints-handling by the administration, set- tling for a ‘bottom-up’ approach. Th is led us to focus on proportionate dispute resolution (PDR) and machinery, such as internal review, by which complaints can be settled before they ripen into disputes. In so doing, we diverged from the ‘top-down’ tradition of administrative law where tribunals are seen as court substitutes. We returned to the classic approach in Chapter 11, looking at the recent reorganisation of the tribunal service and its place in the administrative justice system. We saw how the oral and adversarial tradition of British justice was refl ected in tribunal procedure and considered the importance attached to impartiality and independence, values now protected by ECHR Art. 6(1). We, 529 The Parliamentary Ombudsman: Firefi ghter or fi re-watcher? however, argued that recent reshaping of the tribunal system left unanswered key questions about oral and adversarial proceedings and whether they are always the most appropriate vehicle for resolving disputes with the administra- tion. -

The Patient's View: Doing Medical History from Below Author(S): Roy Porter Source: Theory and Society, Vol
The Patient's View: Doing Medical History from below Author(s): Roy Porter Source: Theory and Society, Vol. 14, No. 2 (Mar., 1985), pp. 175-198 Published by: Springer Stable URL: http://www.jstor.org/stable/657089 . Accessed: 10/04/2013 19:27 Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at . http://www.jstor.org/page/info/about/policies/terms.jsp . JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. Springer is collaborating with JSTOR to digitize, preserve and extend access to Theory and Society. http://www.jstor.org This content downloaded from 131.113.213.135 on Wed, 10 Apr 2013 19:27:23 PM All use subject to JSTOR Terms and Conditions 175 THE PATIENT'S VIEW Doing Medical History from Below ROY PORTER Medicine today is a supremely well-entrenched, prestigious profession, yoked to a body of relatively autonomous, self-directingscience, expertise, and practices. It is hardly surprising, then, that it has tended to produce histories of itself essentially cast in the mold of its own currentimage, stories of successive breakthroughs in medical science, heroic pioneers of surgical techniques, of the supersessionof ignorant folkloric remediesand barefaced charlatanry through the rise of medicine as a liberal, ethical, corporate profession. Even historians and historical sociologists who have taken more skeptical views of medicine's past, perhaps stressing its failures or underlin- ing the self-servingfeatures of professionalization,have neverthelessimplic- itly endorsed the view that the history of healing is par excellence the history of doctors. -

Johnston, Alan
Alan Johnston Personal Details Name Alan Johnston Dates 1928 Place of Birth UK (Manchester) Main work places Aberdeen Principal field of work Clinical genetics Short biography See below Interview Recorded interview made Yes Interviewer Peter Harper Date of Interview 24/09/2008 Edited transcript available See below Personal Scientific Records Significant Record set exists Records catalogued Permanent place of archive Summary of archive Biography Alan Johnston was born 8.1.1928 in Manchester, educated at Manchester Grammar School and studied medicine at Cambridge and UCH qualifying in 1951. He later spent a year at Johns Hopkins Hospital. He became Consultant Physician in the Aberdeen Teaching Hospitals in 1966 and subsequently Clinical Senior Lecturer in medicine and genetics. Fellowship of the three Colleges of Physicians followed. With Eric McKay, he initiated the clinical genetics service for N.E.Scotland. With David Pyke, he played a crucial role in the setting up of the Clinical Genetics Committee of the College of Physicians and was its first Hon. Sec. He also served in various capacities on other committees and working parties concerned in the recognition of the specialty and its training programme, including the Scottish Molecular Genetics Consortium. In addition to lectures to the Royal Colleges, he published around one hundred papers. His outside interests include eldership of the Church of Scotland, active membership of the Christian Medical Fellowship, travel, gardening, archaeology and three grandchildren. INTERVIEW WITH DR ALAN JOHNSTON, 24th SEPTEMBER, 2008 PSH. It’s 24th September 2008 and I’m talking with Dr Alan Johnston from Aberdeen and the recording is being made in London.