Download Into Their Devices and Log in with a Code, Which Claudia Asked for Because Her Previous Phone Broke Down, and She Had to Get a New One
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Aperitivos Tacos Ensaladas Sincronizadas Burritos
APERITIVOS Guacamole 10 Mashed Avocado & Corn Chips de Mole Nachos 9 Corn Chips w/ Black Beans, Cheese, Guacamole, Pico de Gallo & Sour Cream with Choice of Steak, Chicken or Chorizo 11 Crispy Calamary 12 Jalapeño Aioli, Tamarindo Sauce and Corn Relish Chicken Taquitos 7 3 Pan Fried Taquitos with Lettuce, Queso Blanco & Sour Cream Queso Fundido 11 House Blend Melted Cheese Choice of Chorizo or Wild Mushrooms and Flour Tortillas Ceviche de Veracruz 10 Sea Scallop or Fish, Poached in Fresh Lime Juice - Veracruz Style with Onion, Tomato, Jalapeño, Avocado, Cucumber, Cilantro and Olive Oil Cocktail de Camarones 9 Shrimp Cocktail w/ Cocktail Sauce, Onion, Cilantro and Avocado TACOS SINCRONIZADAS 3 Per Order. Quesadillas Served with Onion & Cilantro. No Mix and Match. Made with 2 Flour Tortillas Monterrey Jack & Blanco Cheese, Lettuce Carne Asada 13 & Pico de Gallo Grilled Skirt Steak Carne Asada Grilled Steak 8 Al Pastor 12 Sautéed Garlic Spinach 7 Achiote Marinated Pork with Grill Pineapple Pollo Grilled Chicken 8 Carnitas 12 de Queso (Plain) Cheese 5 Slow Roast Pork Marinated in Citrus Juices Larger Size of Any Sincronizada Pollo 11 Grilled Chicken Seasoned in Guajillo and Ancho Pepper Add 2.50 Baja 13 Crispy Beer Battered Mahi-Mahi, Mango Habanero Salsa, Cabbage and Cilantro BURRITOS Served in Flour Tortilla w/ Cheese, Red Rice, Black or ENSALADAS Pinto Beans, Pico de Gallo & Sour Cream de Mole Salad 8 Carne Asada Grilled Steak 10 Baby Lettuce, Avocado, Tomato, Onion, Peppers, Pollo Grilled Chicken 9 Cucumber, Pumpkin Seed & Balsamic Vinaigrette. -

Dine-In Menu
PURE Tacos puerco al pastor (gf) pollo (gf) marinated & sauteed pork, chipotle chicken, diced onion, pineapple, onion, chihuahua cheese, cilantro, mexicana salsa TAQUERIA cilantro, chile de arbol salsa 2 tacos 9.29 | 3 tacos 11.29 2 tacos 10.29 | 3 tacos 11.99 house made tortillas *carne asada (gf) appetizers birria (gf) marinated & grilled all-natural steak, braised lamb leg, fundido cheese, diced onion, cilantro, guajillo salsa cilantro, onion, adobo grilled tortilla, 2 tacos 12.49 | 3 tacos 14.29 TOTOPOS & Salsa (v | gf) watercress salad, habanero salsa camarÓn o pescado crisp totopos, house & cremosa salsas 1.99 2 tacos 11.99 | 3 tacos 14.99 fried shrimp or fish, poblano slaw, 7 Salsas coliflor O portobello (v | gf) chipotle mayo, cruda tomatillo salsa guajillo, charred verde, cruda, cashew, cascabel, cumin & turmeric roasted cauliflower 2 tacos 11.29 | 3 tacos 13.99 habanero, roasted chile de arbol 5.99 or cilantro grilled portobello mushroom, pescado a la parrilla (gf) queso con todo pumpkin seed pesto, smoked cashew salsa (gf) citrus-grilled fish, charred pico de gallo, 2 tacos 9.29 | 3 tacos 11.29 queso gringo, tinga chicken, black beans, avocado, cruda tomatillo salsa pico de gallo, fresh jalapeños, guacamole 2 tacos 11.99 | 3 tacos 14.99 roasted chile de arbol salsa, totopos 9.99 sandwiches guacamole y TOTOPOS (v | gf) avocado, onion, jalapeño, cilantro, lime, pico de gallo, totopos 9.29 *torta de carne y chorizo torta cubana all-natural steak, chorizo, ham, avocado, black forest ham, braised pork, Queso Gringo (v) jalapeño, -

Environmental Health Criteria 124 Lindane
Environmental Health Criteria 124 Lindane Please note that the layout and pagination of this web version are not identical with the printed version. Lindane (EHC 124, 1991) INTERNATIONAL PROGRAMME ON CHEMICAL SAFETY ENVIRONMENTAL HEALTH CRITERIA 124 LINDANE This report contains the collective views of an international group of experts and does not necessarily represent the decisions or the stated policy of the United Nations Environment Programme, the International Labour Organisation, or the World Health Organization. Published under the joint sponsorship of the United Nations Environment Programme, the International Labour Organisation, and the World Health Organization First draft prepared by Dr M. Herbst, International Centre for the Study of Lindane, Lyon, France and Dr G.J. Van Esch, Bilthoven, The Netherlands World Health Orgnization Geneva, 1991 The International Programme on Chemical Safety (IPCS) is a joint venture of the United Nations Environment Programme, the International Labour Organisation, and the World Health Organization. The main objective of the IPCS is to carry out and disseminate evaluations of the effects of chemicals on human health and the quality of the environment. Supporting activities include the development of epidemiological, experimental laboratory, and risk-assessment methods that could produce internationally comparable results, and the development of manpower in the field of toxicology. Other activities carried out by the IPCS include the development of know-how for coping with chemical accidents, -
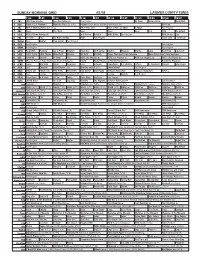
Sunday Morning Grid 4/1/18 Latimes.Com/Tv Times
SUNDAY MORNING GRID 4/1/18 LATIMES.COM/TV TIMES 7 am 7:30 8 am 8:30 9 am 9:30 10 am 10:30 11 am 11:30 12 pm 12:30 2 CBS CBS News Sunday Face the Nation (N) Paid Program JB Show History Astro. Basketball 4 NBC Today in L.A. Weekend Meet the Press (N) (TVG) Hockey Boston Bruins at Philadelphia Flyers. (N) PGA Golf 5 CW KTLA 5 Morning News at 7 (N) Å KTLA News at 9 KTLA 5 News at 10am In Touch Paid Program 7 ABC News This Week News News News Paid NBA Basketball 9 KCAL KCAL 9 News Sunday (N) Joel Osteen Schuller Mike Webb Paid Program REAL-Diego Paid 11 FOX In Touch Paid Fox News Sunday News Paid Program I Love Lucy I Love Lucy 13 MyNet Paid Matter Fred Jordan Paid Program 18 KSCI Paid Program Paid Program 22 KWHY Paid Program Paid Program 24 KVCR Paint With Painting Joy of Paint Wyland’s Paint This Oil Painting Kitchen Mexican Martha Jazzy Real Food Chefs Life 28 KCET 1001 Nights 1001 Nights Mixed Nutz Edisons Biz Kid$ Biz Kid$ Things That Aren’t Here Anymore More Things Aren’t Here Anymore 30 ION Jeremiah Youseff In Touch Paid NCIS: Los Angeles Å NCIS: Los Angeles Å NCIS: Los Angeles Å NCIS: Los Angeles Å 34 KMEX Misa de Pascua: Papa Francisco desde el Vaticano Fútbol Fútbol Mexicano Primera División (N) República Deportiva 40 KTBN James Win Walk Prince Carpenter Jesse In Touch PowerPoint It Is Written Jeffress K. -

Short Rib Cochinita Pibil
Salsas are key to Taco-eating. Try many, own your taco. We make ours fresh, in house from the best ingredients available. (1.5 each or 5 for 5.0) MEXICANA LA MAYA MORITA VERDE FRESCA Tomato, white onion, Pineapple, Chipotle, tomatillos, Serrano chillies, jalepeño, lime, coriander habañero vegetable stock tomatillos, coriander MILD QUITE SPICY QUITE SPICY SPICY BOTANITAS ...................................4 Jicama, celery, carrot crudites. Chilli, lime & salt dressing CHILE DE ARBOL DEL VIC EL DIABLO Toasted arbol chillies Charred habañero Made using a mix of the hottest chillies GUACAMOLE ............................6.5 & garlic oil & lime on the planet (only for massive show-offs) Served with totopos or chicharron VERY SPICY HOT WILD or both ..................................................... 7.5 In Mexico, shellfish and seafood is often eaten raw in ceviches, cocteles or aguachiles, especially on the Pacific Coast and Baja California. 2 pcs per portion OYSTERS ......................... (each) 3 CLAMS ...................................9.5 Mezcal, citrus dressing, worm salt Dorset Giant Cherrystone, pico de TUNA .............................................. 9 or with pickled Jalapeño and lime ....... 3.5 gallo, jalapeño, salsa Valentina (raw) Avocado, chile de arbol, blue corn tostada APACHE ...................................8.5 AGUACHILE .............................10 Flank tartare, lime, spices, salsa Valentina Seabass, lime, serrano chilli (raw) COCHINITA ..............................5.5 Seafood cocktails Slow roast pork shoulder marinated in orange, anchiote and charred garlic, CEVICHE ................................ 11 ACAPULCO ...........................11.5 red onion-habanero escabeche Seabass (raw, marinated in lime juice), Prawns (cooked) pico de gallo, tomato salsa, pico de gallo, spices traditionally served slightly sweet Two per portion. Some of our tacos are quite fiery. We can dial this down All served with fresh tortillas (2-4 people, appetite depending) where possible. -

Diapositiva 1
Semana Lunes Martes Miércoles Jueves Viernes Desayuno Melón Gelatina Papaya Huevo Gelatina Cereal con Conchas Salchicha revuelto Panque leche Leche frita Leche Atole 1 pan bimbo Tortilla Refrigerio Torta Fruta de Verduras Quesadilla Fruta De jamón temporada julianas Brócoli Manzana Palitos de (1) Jícama Enfrijoladas zanahoria Pan telera Pepino ½ plátano con queso ½ Galletas o 1, ½ saladas (2) alegría Ate Comida Sopa de Arroz blanco Crema de Sopa de Sopa de pasta Calabacitas zanahoria pasta verdura Picadillo a la Torta de Pechuga Bistec en Lunetas mexicana atún con frita jitomate Natilla de papa Ensalada de Con chocolate Ensalada zanahoria calabacitas fresca * Flan y chícharos Fruta Agua Melón Semana Lunes Martes Miércoles Jueves Viernes 2 Desayuno Gelatina Manzana Melón Papaya y Pera Rolles de Hot cakes Burritos de plátano con Jugo canela Leche frijol yogurt y Dobladitas Leche Leche granola de pollo Refrigerio Salchichas en Huevo duro Gelatina Tacos de Jícama, salsa verde Con cátsup Ensalada de frijoles zanahoria y con papas Ensalada de atún blandos pepino con Tortilla (1) Lechuga con Pan (1) chile y limón jitomate Palanqueta Comida Arroz Espagueti Sopa de Sopa de Sopa de Caldo de Albóndigas codito verduras pasta pollo con Bocadín Tortitas de Tinga de Milanesa verduras papa pollo con empanizada Bombón Ensalada de tostadas Ensalada de pepinos Arroz con col Manzana leche zanahoria, espinaca Fruta Semana Lunes Martes Miércoles Jueves Viernes 3 Desayuno Leche con Sincronizada Huevo Gelatina Pera cereal con lechuga revuelto Pan con Galletas -

Las Adaptaciones De Obras Del Teatro Español En El Cine Y El Influjo De Éste En Los Dramaturgos - Juan De Mata Moncho Aguirre Indice
Las adaptaciones de obras del teatro español en el cine y el influjo de éste en los dramaturgos - Juan de Mata Moncho Aguirre Indice Síntesis ....................................................................................................... i Abstract .....................................................................................................iv I. Prólogo ................................................................................................... 1 II. Épocas literarias ................................................................................. 14 1. Época Renacentista ......................................................................14 2. Teatro del siglo de oro ................................................................... 24 3. Teatro del siglo XVIII...................................................................... 52 4. Teatro del siglo XIX........................................................................ 58 5. Teatro del siglo XX....................................................................... 123 III. Conclusiones .................................................................................. 618 IV. Bibliografía....................................................................................... 633 V. Archivos documentales................................................................... 694 Las adaptaciones de obras del teatro español en el cine y el influjo de éste en los dramaturgos - Juan de Mata Moncho Aguirre Síntesis Al afrontar las vinculaciones de los dramaturgos -

Human Pharmacology of Ayahuasca: Subjective and Cardiovascular Effects, Monoamine Metabolite Excretion and Pharmacokinetics
TESI DOCTORAL HUMAN PHARMACOLOGY OF AYAHUASCA JORDI RIBA Barcelona, 2003 Director de la Tesi: DR. MANEL JOSEP BARBANOJ RODRÍGUEZ A la Núria, el Marc i l’Emma. No pasaremos en silencio una de las cosas que á nuestro modo de ver llamará la atención... toman un bejuco llamado Ayahuasca (bejuco de muerto ó almas) del cual hacen un lijero cocimiento...esta bebida es narcótica, como debe suponerse, i á pocos momentos empieza a producir los mas raros fenómenos...Yo, por mí, sé decir que cuando he tomado el Ayahuasca he sentido rodeos de cabeza, luego un viaje aéreo en el que recuerdo percibia las prespectivas mas deliciosas, grandes ciudades, elevadas torres, hermosos parques i otros objetos bellísimos; luego me figuraba abandonado en un bosque i acometido de algunas fieras, de las que me defendia; en seguida tenia sensación fuerte de sueño del cual recordaba con dolor i pesadez de cabeza, i algunas veces mal estar general. Manuel Villavicencio Geografía de la República del Ecuador (1858) Das, was den Indianer den “Aya-huasca-Trank” lieben macht, sind, abgesehen von den Traumgesichten, die auf sein persönliches Glück Bezug habenden Bilder, die sein inneres Auge während des narkotischen Zustandes schaut. Louis Lewin Phantastica (1927) Agraïments La present tesi doctoral constitueix la fase final d’una idea nascuda ara fa gairebé nou anys. El fet que aquest treball sobre la farmacologia humana de l’ayahuasca hagi estat una realitat es deu fonamentalment al suport constant del seu director, el Manel Barbanoj. Voldria expressar-li la meva gratitud pel seu recolzament entusiàstic d’aquest projecte, molt allunyat, per la natura del fàrmac objecte d’estudi, dels que fins al moment s’havien dut a terme a l’Àrea d’Investigació Farmacològica de l’Hospital de Sant Pau. -

Tabla Composición De Alimentos REIMPRESIÓN
INSTITUTO DE NUTRICIÓN DE CENTRO AMÉRICA Y PANAMÁ (INCAP) ORGANIZACIÓN PANAMERICANA DE LA SALUD (OPS) INCAP INCAP http://www.incap.int Segunda Edición © Copyright 2006 Guatemala, Centroamérica Tercera reimpresión Febrero 2012 INSTITUTO DE NUTRICIÓN DE CENTRO AMÉRICA Y PANAMÁ (INCAP) ORGANIZACIÓN PANAMERICANA DE LA SALUD (OPS) INCAP Tercera reimpresión, 2012 ME/085.3 2007 INCAP. Tabla de Composición de Alimentos de Centroamérica./INCAP/ Menchú, MT (ed); Méndez, H. (ed). Guatemala: INCAP/OPS, 2007. 2ª. Edición. viii - 128 pp. I.S.B.N. 99922-880-2-7 1. ANÁLISIS DE LOS ALIMENTOS 2. ALIMENTOS 3. VALOR NUTRITIVO Responsables de la producción de esta edición: Revisión y actualización técnica Licda. María Teresa Menchú Lic. Humberto Méndez, INCAP Coordinación de la edición y publicación Licda. Norma Alfaro, INCAP Segunda Edición Segunda reimpresión, 2009. Tercera reimpresión, 2012. Impresión: Serviprensa, S.A. PBX: 2245 8888 Tabla de Composición de Alimentos de Centroamérica Contenido Presentación................................................................................................................... v Introducción ..................................................................................................................vii Parte I. Documentación A. Antecedentes .............................................................................................................3 B. Metodología aplicada .................................................................................................. 4 C. Presentación de la Tabla de Composición -

Around the World in 80 Food Trucks 1 Preview
Lobster mac ‘n’ cheese, BOB’s Lobster 26 Buttermilk-fried-chicken biscuit OCEANIA SOUTH AMERICA Newport bowl with tofu, Califarmication 144 Great balls of fire pork & beef meatballs, sandwiches, Humble Pie 56 Detox açai bowl, Açai Corner 82 Peruvian sacha taco, Hit ‘n Run 110 BEC sandwich, Paperboy 146 contents The Bowler 28 Super cheddar burger, Paneer 58 Carolina smoked pulled pork sandwich, The Cajacha burger, Lima Sabrosa 112 The Viet banh mi, Chicago Lunchbox 148 Goat’s cheese, honey & walnut Turkey burger, Street Chefs 60 Sneaky Pickle 84 Yakisoba bowl, Luca China 114 Blue cheese slaw, Banjo's 150 Introduction 5 toasted sandwich, The Cheese Truck 30 Forest pancake, Belki&Uglevody 62 The Bahh lamb souvlaki, Argentine sandwich, El Vagabundo 116 Old-fashioned peach cake, The Peach Truck 152 Jerusalem spiced chicken, Laffa 32 Greek Street Food 86 Uruguayan flan, Merce Daglio Sweet Truck 118 Alabama tailgaters, Fidel Gastro’s 154 EUROPE Fried chicken, Mother Clucker 34 AFRICA & MIDDLE EAST Mr Chicken burger, Mr Burger 88 Tapioca pancake, Tapí Tapioca 120 Nanner s’more, Meggrolls 156 Spicy Killary lamb samosas, Chicken, chilli & miso gyoza, Rainbo 36 South African mqa, 4Roomed eKasi Culture 64 Tuscan beef ragu, Pasta Face 90 Red velvet cookies, Misunderstood Heron 6 Asparagus, ewe’s cheese, mozzarella & Asian bacon burger, Die Wors Rol 66 The Fonz toastie, Toasta 92 NORTH AMERICA Captain Cookie and the Milk Man 158 San Francisco langoustine roll, hazelnut pizza, Well Kneaded 38 Chicken tikka, Hangry Chef 68 Butter paneer masala, Yo India -

Cenote Menudigital ING Sin Precios
The Mayan solar is a family garden; lives and life cycles That, like a seashell, goes infinitely round And carries the sound of a language that From generation to generation, performs the same role: Lives and life cycles. We bring the garden to the table And so our values emerge And spin infinitely, Like a seashell carrying the sound of a language From generation to generation For lives and life cycles. BREAKFAST | SALTY FLAVOR French style quiche with longaniza of Valladolid, caramelized onions, regional pumpking and fresh local requeson. Chaya (Mayan spinach) green omelette, sour cream, turkey ham and Oaxaca cheese. Hamburger with egg, bacon, smoked cheese, mustard and caramelized onion, served with potatoes and homemade dressing. Croissant with smoked speck, swiss cheese, arugula and cherry tomato, accompanied with chipotle and basil dressing. Vegan Mollete, smashed beans, fresh spinach, tofu aioli and pico de gallo with guacamole. Classic Chilaquiles, red or green sauce with starry egg. Starry egg on homemade bread, avocado, jalapeño chili, provolone cheese and salad from our garden. Classic Motuleños eggs with ham, peas, plantain and cheese from Chiapas. English breakfast, scrambled or starry eggs, bacon or english sausage, served with homemade bread, cooked beans with baked tomato. Huitlacoche Bagel, with smoked salmon, arugula, tomato, cream cheese, accompanied with guacamole and caper dressing. BREAKFAST | SWEET TASTE Dates fruit smoothie bowl with banana and almond milk. Smoothie bowl with hazelnut praline, coconut milk with chocolate brownie. Seasonal mixed fruit plate, jam and honey. Fruit bowl mixed with granola and one of our toppings: greek yogurt, plain yogurt, vegan coconut yogurt or cottage cheese. -

DESAYUNOS PITUFO MOLLETE Tomate Y Aceite
DESAYUNOS PITUFO MOLLETE Tomate y aceite ...........................................................................................................1,20 € ......... 1,80 € Pâté .............................................................................................................................1,50 € ......... 2,25 € Sobrasada ...................................................................................................................1,50 € ......... 2,25 € Mantequilla y mermelada ...........................................................................................1,50 € ......... 2,25 € Jamón cocido ..............................................................................................................1,80 € ......... 2,70 € Queso barra.................................................................................................................1,80 € ......... 2,70 € Atún .............................................................................................................................1,80 € ......... 2,70 € Jamón cocido y queso .................................................................................................2,00 € ......... 3,00 € Jamón serrano ............................................................................................................2,00 € ......... 3,00 € Queso puro oveja ........................................................................................................2,50 € ......... 3,25 € Jamón ibérico ..............................................................................................................2,50