Total Maxillectomy and Orbital Exenteration
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MR Imaging of the Orbital Apex
J Korean Radiol Soc 2000;4 :26 9-0 6 1 6 MR Imaging of the Orbital Apex: An a to m y and Pat h o l o g y 1 Ho Kyu Lee, M.D., Chang Jin Kim, M.D.2, Hyosook Ahn, M.D.3, Ji Hoon Shin, M.D., Choong Gon Choi, M.D., Dae Chul Suh, M.D. The apex of the orbit is basically formed by the optic canal, the superior orbital fis- su r e , and their contents. Space-occupying lesions in this area can result in clinical d- eficits caused by compression of the optic nerve or extraocular muscles. Even vas c u l a r changes in the cavernous sinus can produce a direct mass effect and affect the orbit ap e x. When pathologic changes in this region is suspected, contrast-enhanced MR imaging with fat saturation is very useful. According to the anatomic regions from which the lesions arise, they can be classi- fied as belonging to one of five groups; lesions of the optic nerve-sheath complex, of the conal and intraconal spaces, of the extraconal space and bony orbit, of the cav- ernous sinus or diffuse. The characteristic MR findings of various orbital lesions will be described in this paper. Index words : Orbit, diseases Orbit, MR The apex of the orbit is a complex region which con- tains many nerves, vessels, soft tissues, and bony struc- Anatomy of the orbital apex tures such as the superior orbital fissure and the optic canal (1-3), and is likely to be involved in various dis- The orbital apex region consists of the optic nerve- eases (3). -

Branches of the Maxillary Artery of the Domestic
Table 4.2: Branches of the Maxillary Artery of the Domestic Pig, Sus scrofa Artery Origin Course Distribution Departs superficial aspect of MA immediately distal to the caudal auricular. Course is typical, with a conserved branching pattern for major distributing tributaries: the Facial and masseteric regions via Superficial masseteric and transverse facial arteries originate low in the the masseteric and transverse facial MA Temporal Artery course of the STA. The remainder of the vessel is straight and arteries; temporalis muscle; largely unbranching-- most of the smaller rami are anterior auricle. concentrated in the proximal portion of the vessel. The STA terminates in the anterior wall of the auricle. Originates from the lateral surface of the proximal STA posterior to the condylar process. Hooks around mandibular Transverse Facial Parotid gland, caudal border of the STA ramus and parotid gland to distribute across the masseter Artery masseter muscle. muscle. Relative to the TFA of Camelids, the suid TFA has a truncated distribution. From ventral surface of MA, numerous pterygoid branches Pterygoid Branches MA Pterygoideus muscles. supply medial and lateral pterygoideus muscles. Caudal Deep MA Arises from superior surface of MA; gives off masseteric a. Deep surface of temporalis muscle. Temporal Artery Short course deep to zygomatic arch. Contacts the deep Caudal Deep Deep surface of the masseteric Masseteric Artery surface of the masseter between the coronoid and condylar Temporal Artery muscle. processes of the mandible. Artery Origin Course Distribution Compensates for distribution of facial artery. It should be noted that One of the larger tributaries of the MA. Originates in the this vessel does not terminate as sphenopalatine fossa as almost a terminal bifurcation of the mandibular and maxillary labial MA; lateral branch continuing as buccal and medial branch arteries. -

Gross Anatomy
www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY www.BookOfLinks.com Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The authors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the authors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of the information contained in this work. Readers are encouraged to confirm the infor- mation contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. www.BookOfLinks.com THE BIG PICTURE GROSS ANATOMY David A. Morton, PhD Associate Professor Anatomy Director Department of Neurobiology and Anatomy University of Utah School of Medicine Salt Lake City, Utah K. Bo Foreman, PhD, PT Assistant Professor Anatomy Director University of Utah College of Health Salt Lake City, Utah Kurt H. -

Turn-Over Orbital Septal Flap and Levator Recession for Upper-Eyelid
Eye (2013) 27, 1174–1179 & 2013 Macmillan Publishers Limited All rights reserved 0950-222X/13 www.nature.com/eye 1 2 3 1 CLINICAL STUDY Turn-over orbital A Watanabe , PN Shams , N Katori , S Kinoshita and D Selva2 septal flap and levator recession for upper-eyelid retraction secondary to thyroid eye disease Abstract Background A turn-over septal flap has been Keywords: upper-eyelid retraction; orbital reported as a spacer for levator lengthening septal flap; levator recession in a single case report. This study reports the preliminary outcomes of this technique in a series of patients with upper-lid retraction (ULR) associated with thyroid eye disease 1Department of Ophthalmology, Introduction Kyoto Prefectural University of (TED) causing symptomatic exposure Medicine, Kyoto, Japan keratopathy (EK). Achieving a predictable eyelid height and Methods Retrospective, multicenter study contour in the surgical correction of upper- 2 Department of Ophthalmology of 12 eyelids of 10 patients with TED eyelid retraction remains a challenge for and Visual Sciences, South Australian Institute of undergoing a transcutaneous levator- surgeons, as evidenced by the variety of Ophthalmology, Adelaide lengthening technique using the reflected procedures reported.1,2 These techniques are University, Adelaide, South orbital septum (OS) as a spacer. Change in based on weakening or lengthening the Australia, Australia palpebral aperture (PA) and contour, position upper-eyelid retractors and include anterior or 3Department of Oculoplastic of the skin crease (SC), symptoms of EK, and posterior approaches to graded recession and Orbital Surgery, Seirei complications were recorded. or resection of Mu¨ ller’s muscle,3–5 levator Hamamatsu Hospital, Results The average age was 47.5 years. -

The Development of the Human Maxilla, Vomer, and Paraseptal Cartilages
THE DEVELOPMENT OF THE HUMAN MAXILLA, VOMER, AND PARASEPTAL CARTILAGES. By Professor FAWCETT, M.D., University of Bristol. THE usually accepted descriptions of the development of the maxilla of man state that it arises by a number of separate centres-the number varying somewhat with the authority, likewise the situation of these centres. No description of the maxilla can be considered complete unless at the same time notice is taken of the manner of development of the premaxilla, which, of course, forms the anterior segment of the adult bone as usually interpreted. But the consideration of the development of the premaxilla may be left until that of the maxilla has been fully dealt with. Before breaking new ground, it may be well to state what are the usual statements with reference to the ossification of the maxilla. These statements are apparently for the most part based on work done by Callender, Toldt, Rambaud and Renault, and Bland Sutton, so far as concerns human anatomy. More recently Franklin Mall has given his views on the subject in the American Jouarnal of Anatomy, views based on observation of specimens treated by the "clearing" method of Schulze. So far as they go, these statements are in harmony with my own notions, which I have for several years now taught. A very precise account is given in Cunningham's Text-book of Anatomy. The maxilla is there stated to be developed in the connective tissue around the oral cavity of the embryo from centres which are not preceded by cartilage, of uncertain number, as early fusion takes place between them. -

Pocket Atlas of Human Anatomy 4Th Edition
I Pocket Atlas of Human Anatomy 4th edition Feneis, Pocket Atlas of Human Anatomy © 2000 Thieme All rights reserved. Usage subject to terms and conditions of license. III Pocket Atlas of Human Anatomy Based on the International Nomenclature Heinz Feneis Wolfgang Dauber Professor Professor Formerly Institute of Anatomy Institute of Anatomy University of Tübingen University of Tübingen Tübingen, Germany Tübingen, Germany Fourth edition, fully revised 800 illustrations by Gerhard Spitzer Thieme Stuttgart · New York 2000 Feneis, Pocket Atlas of Human Anatomy © 2000 Thieme All rights reserved. Usage subject to terms and conditions of license. IV Library of Congress Cataloging-in-Publication Data is available from the publisher. 1st German edition 1967 2nd Japanese edition 1983 7th German edition 1993 2nd German edition 1970 1st Dutch edition 1984 2nd Dutch edition 1993 1st Italian edition 1970 2nd Swedish edition 1984 2nd Greek edition 1994 3rd German edition 1972 2nd English edition 1985 3rd English edition 1994 1st Polish edition 1973 2nd Polish edition 1986 3rd Spanish edition 1994 4th German edition 1974 1st French edition 1986 3rd Danish edition 1995 1st Spanish edition 1974 2nd Polish edition 1986 1st Russian edition 1996 1st Japanese edition 1974 6th German edition 1988 2nd Czech edition 1996 1st Portuguese edition 1976 2nd Italian edition 1989 3rd Swedish edition 1996 1st English edition 1976 2nd Spanish edition 1989 2nd Turkish edition 1997 1st Danish edition 1977 1st Turkish edition 1990 8th German edition 1998 1st Swedish edition 1979 1st Greek edition 1991 1st Indonesian edition 1998 1st Czech edition 1981 1st Chinese edition 1991 1st Basque edition 1998 5th German edition 1982 1st Icelandic edition 1992 3rd Dutch edtion 1999 2nd Danish edition 1983 3rd Polish edition 1992 4th Spanish edition 2000 This book is an authorized and revised translation of the 8th German edition published and copy- righted 1998 by Georg Thieme Verlag, Stuttgart, Germany. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Download PDF File
Folia Morphol. Vol. 78, No. 2, pp. 331–343 DOI: 10.5603/FM.a2018.0084 O R I G I N A L A R T I C L E Copyright © 2019 Via Medica ISSN 0015–5659 journals.viamedica.pl Morphometric evaluation and surgical implications of the infraorbital groove, canal and foramen on cone-beam computed tomography and a review of literature İ. Bahşi1, M. Orhan1, P. Kervancioğlu1, E.D. Yalçin2 1Department of Anatomy, Faculty of Medicine, Gaziantep University, Gaziantep, Turkey 2Department of Dentomaxillofacial Radiology, Faculty of Dentistry, Gaziantep University, Gaziantep, Turkey [Received: 25 June 2018; Accepted: 8 August 2018] Background: The purpose of this study is to evaluate the anatomy, morphometry, and variations of infraorbital groove (IOG), infraorbital canal (IOC) and infraorbital foramen (IOF) on the cone-beam computed tomography (CBCT) images and to investigate their relations with surrounding structures. Methods: IOG, IOC and IOF were evaluated retrospectively in CBCT images of 75 female (F) and 75 male (M) cases with a range of 18–65 years (F: 37.62 ± ± 13.55, M: 37.53 ± 15.87) by Planmeca Romexis programme. IOG, IOC and IOF were examined bilaterally (300 sides) in the cases. The 13 parameters were measured on these images in axial, sagittal and coronal planes. Results: There was a very weak positive correlation between the age and the angle between IOC and IOG (p = 0.015, r = 0.198), there was a weak positive correlation between the age and skin thickness (p = 0.001, r = 0.281), and there was no correlation between the age and other parameters. -
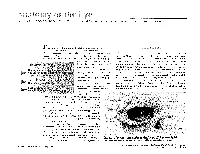
The Orbit Is Composed Anteri
DAVID L. PARVER, MD The University of Texas Southwestern Medical Center, Dallas Theability to successfully assess and treat The Orbit physical ailments requires an understanding of the anatomy involved in the injury or The eye itself lies within a protective shell trauma. When dealing with injuries and called the bony orbits. These bony cavities are trauma associated with the eye, it is neces- located on each side of the root of the nose. sary to have a work- Each orbit is structured like a pear with the ing knowledge of optic nerve, the nerve that carries visual im- basic ocular anatomy pulses from the retina to the brain, represent- so that an accurate ing the stem of the orbtt (Duke-Elder, 1976). Understa eye also diagnosis can be Seven bones make up the bony orbit: frontal, achieved and treat- zygomatic, maxillary, ethmoidal, sphenoid, ment can be imple- lacrimal, and palatine (Figures 1 and 2). in a bony " mented. The roof of the orbit is composed anteri- . .. The upcoming ar- orly of the orbital plate of the frontal bone ticles in this special and posteriorly by the lesser wing of the sphe- Each portion of the 01 I noid bone. The lateral wall is separated from .r. theme section the nervc an eye will deal specifically 2 with recognizing ocular illness, disease, and injuries, and will also address the incidence of sports related eye injuries and trauma. This paper covers the ba- sics of eye anatomy, focusing on the eye globe and its surrounding struc- tures. Once one gains an understand- ing of the normal anatomy of the eye, it will be easier to recognize trauma, injury, or illness. -

Eyelash Inversion in Epiblepharon: Is It Caused by Redundant Skin?
ORIGINAL RESEARCH Eyelash inversion in epiblepharon: Is it caused by redundant skin? Hirohiko Kakizaki1 Purpose: To evaluate the effect of redundant lower eyelid skin on the eyelash direction in Igal Leibovitch2 epiblepharon. Yasuhiro Takahashi3 Materials and methods: Asian patients with epiblepharon participated in this study. The Dinesh Selva4 lower eyelid skin was pulled downward in the upright position with the extent just to detach from eyelash roots, and the direction of the eyelashes was examined. These evaluations were 1Department of Ophthalmology, Aichi Medical University, Nagakute, repeated before surgery while the patients were lying supine under general anesthesia. Aichi 480-1195, Japan; 2Division of Results: The study included 41 lower eyelids of 25 patients (17 females, 8 males, average age; Oculoplastic and Orbital Surgery, 5.6 years, 16 cases bilateral, 9 unilateral). In the upright position, without downward traction Department of Ophthalmology, Tel-Aviv Medical Center, of the skin, the eyelashes were vertically positioned and touching the cornea. The redundant Tel-Aviv University, Tel-Aviv, Israel; skin touched only the eyelash roots and had minimal contribution to eyelash inversion. With 3 Department of Ophthalmology downward skin traction, there was no signifi cant change in the eyelash direction. In the spine and Visual Sciences, Osaka City University Graduate School position, the eyelashes were touching the cornea, and there was marked redundant skin that was of Medicine, Osaka 545-8585, Japan; pushing the eyelashes inward. With downward skin traction, there was no signifi cant change. 4 South Australian Institute Conclusions: The direction of lower eyelashes in patients with epiblepharon was less infl uenced of Ophthalmology and Discipline For personal use only. -

Trigeminal Nerve, Mandibular Division Basic Anatomy and a Bit More
The palate and the faucial isthmus He who guards his mouth and his tongue keeps himself from calamity. Proverbs 21:23 Ph.D., Dr. David Lendvai Parts of the oral cavity Parts of the oral cavity 1. Vestibule of the oral cavity Borders: - lips and cheek (bucca) - dental arches 2. Oral cavity proper Borders: - roof: hard and soft palate - floor: oral diaphragm (mylohoid m.) - antero-laterally: dental arches - posteriorly: isthmus of the fauces Etrance of the oral cavity - Philtrum - Upper & lower lip - Angulus - Rubor labii - Nasolabial groove (Facial palsy) Sobotta Szentágothai - Réthelyi Aspectus anterior 1 zygomatic process 2 frontal process 2 4 alveolar process 1 4 Faller (left) lateral aspect 1 zygomatic process 2 frontal process 3 orbital surface 4 alveolar process 2 3 Sobotta 1 4 Faller (right) Medial aspect Sobotta Superior aspect Sobotta Inferior aspect Sobotta http://www.almanahmedical.eu Sobotta Florian Dental – Dr. S. Kovách Fehér Fehér Szél Szél http://www.hc-bios.com Structures of the hard palate - incisive papilla - palatine rugae - palatine raphe - torus Hard and soft palate Muscles of the soft palate - Levator veli palatini m. - Tensor veli palatini m. - Palatoglossus m. - Palatopharyngeus m. - M. uvulae Muscles of the soft palate Muscles of the soft palate Structures of the hard and soft palate - mucous membrane - palatine glands - bone / muscles Histology of the hard palate Mucoperiosteum Histology of the soft palate NASAL SURFACE - pseudostratified ciliated columnar epithelium - lamina propria - mucous glands - striated -

Original Article Anatomic Study of the Lacrimal Fossa and Lacrimal Pathway
Original Article Anatomic study of the lacrimal fossa and lacrimal pathway for bypass surgery with autogenous tissue grafting Hai Tao, Zhi‑zhong Ma1, Hai‑Yang Wu, Peng Wang, Cui Han Purpose: To study the microsurgical anatomy of the lacrimal drainage system and to provide anatomical Access this article online evidence for transnasal endoscopic lacrimal drainage system bypass surgery by autogenous tissue grafting. Website: Materials and Methods: A total of 20 Chinese adult cadaveric heads in 10% formaldehyde, comprising www.ijo.in 40 lacrimal ducts were used. The middle third section of the specimens were examined for the following DOI: features: the thickness of the lacrimal fossa at the anterior lacrimal crest, vertical middle line, and posterior 10.4103/0301-4738.121137 lacrimal crest; the cross section of the upper opening, middle part, and lower opening of the nasolacrimal PMID: canal; the horizontal, 30° oblique, and 45° oblique distances from the lacrimal caruncle to the nasal cavity; ***** the distance from the lacrimal caruncle to the upper opening of the nasolacrimal duct; and the included Quick Response Code: angle between the lacrimal caruncle–nasolacrimal duct upper opening junction and Aeby’s plane. Results: The middle third of the anterior lacrimal crest was significantly thicker than the vertical middle line and the posterior lacrimal crest (P > 0.05). The horizontal distance, 30° oblique distance, and 45° oblique distance from the lacrimal caruncle to the nasal cavity exhibited no significant differences (P > 0.05). The included angle between the lacrimal caruncle and the lateral wall middle point of the superior opening line of the nasolacrimal duct and Aeby’s plane was average (49.9° ± 1.8°).