Download File
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Human Resource Development Sector Report
Human Resource Development Sector Report July 2021 Copyright © 2021 Development Monitoring and Evaluation Office (DMEO), NITI Aayog, Government of India All rights reserved. This report or any portion thereof may not be reproduced or used in any manner whatsoever without the express written permission of DMEO, NITI Aayog, Government of India. All information, ideas, views, opinions, estimates, advice, suggestions, recommendations (hereinafter 'content') in this publication should neither be understood as professional advice in any manner nor interpreted as policies, objectives, opinions or suggestions of the Development Monitoring and Evaluation Office (DMEO), NITI Aayog. Readers are advised to use their discretion and seek professional advice before taking any action or decision, based on the contents of this publication. The content in this publication has been obtained or derived from sources believed by DMEO to be reliable but DMEO does not represent this information to be accurate or complete. DMEO does not assume any responsibility and disclaim any liability for any loss, damages, caused due to any reason whatsoever, towards any person (natural or legal) who uses this publication. Analysis by KPMG Advisory services Private Limited Survey Partner Hansa Research Group Private Limited www.dmeo.gov.in www.niti.gov.in 1 Preface The Government of India (GoI) spends close to Rs. 14 lakh crores annually on development activities, through nearly 750 schemes implemented by Union Ministries. To improve the effectiveness and efficiency of public finance, and the quality of service-delivery to citizens, all schemes have been mandated to undergo third party evaluations, to provide an evidentiary foundation for scheme continuation from 2021-22 to 2025-26. -

Maternal Health 8
MATERNAL HEALTH 8 Maternal and child health has remained an integral part of the Family Welfare Programme of India since the time of the First and Second Five-Year Plans (1951-56 and 1956- 61) when the Government of India took steps to strengthen maternal and child health services. As part of the Minimum Needs Programme initiated during the Fifth Five-Year Plan (1974-79), maternal health, child health, and nutrition services were integrated with family planning services. In 1992-93, the Child Survival and Safe Motherhood Programme continued the process of integration by bringing together several key child survival interventions with safe motherhood and family planning activities (Ministry of Health and Family Welfare, 1992). In 1996, safe motherhood and child health services were incorporated into the Reproductive and Child Health Programme (RCH). The National Population Policy adopted by the Government of India in 2000 reiterates the government’s commitment to safe motherhood programmes within the wider context of reproductive health (Ministry of Health and Family Welfare, 2000). Several of the national sociodemographic goals for 2010 specified by the policy pertain to safe motherhood. For 2010, the goals are that 80 percent of all deliveries should take place in institutions, 100 percent of deliveries should be attended by trained personnel, and the maternal mortality ratio should be reduced to a level below 100 per 100,000 live births. To improve the availability of and access to quality health care, especially for those residing in rural areas, the poor, women, and children, the government recently launched the National Rural Health Mission for the 2005-2012 period. -

INDIA YEAR BOOK-2017 Good Luck!
INDIA YEAR BOOK - 2017 INDIA YEAR BOOK-2017 Dear Students, With the focus on the provision of best study material to our students, Rau’s IAS Study Circle is innovatively presenting the voluminous INDIA YEAR BOOK-2017 in a very concise and lucid manner. Through this, efforts have been taken to circulate the best synopsis extracted from the Year Book-2017 for the benefit of the students. The abstract has been designed to present contents of the year book in most user-friendly manner. All the major and important points are given in bold and highlighted. The content is also supported by figures and pictures as per the requirement. The content has been chosen and compiled judiciously so that maximum coverage of all the relevant and significant material is presented within minimum readable pages. The issue titled ‘INDIA YEAR BOOK-2017 will be covering the following topics: 1. Land and the People 16. Health and Family Welfare 2. National Symbols 17. Housing 3. The Polity 18. India and the World 4. Agriculture 19. Industry 5. Culture and Tourism 20. Law and Justice 6. Basic Economic Data 21. Labour, Skill Development and Employment 7. Commerce 22. Mass Communication 8. Communications and Information Technology 23. Planning 9. Defence 24. Rural and Urban Development 10. Education 25. Scietific and Technological Developments 11. Energy 26. Transport 12. Environment 27. Water Resources 13. Finance 28. Welfare 14. Corporate Affairs 29. Youth Affairs and Sports 15. Food and Civil Supplies By providing this, the Study Circle hopes that all the students will be able to make the best use of it as a ready reference material and allay their fears of perusing and cramming the entire year book. -
Sustainable Development Goals and Revised Mapping of Csss and Ministries of Government of India
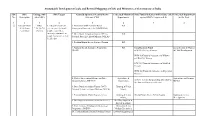
Sustainable Development Goals and Revised Mapping of CSSs and Ministries of Government of India SDG SDG Linkage with SDG Targets Centrally Sponsored /Central Sector Concerned Ministries/ State Funded Schemes (with Scheme code) Concerned Department No. Description other SDGs Schemes (CSS) Departments against SDG's Targets (col. 4) in the State 1 2 3 4 5 6 7 8 ① End poverty in SDGs 1.1 By 2030, eradicate 1. Mahatma Gandhi National Rural RD all its forms 2,3,4,5,6,7,8, extreme poverty for all Employment Guarantee Act (MGNREGA) everywhere 10,11,13 people everywhere, currently measured as 2. Deen Dayal Antyodaya Yojana (DAY) - RD people living on less than National Rural Livelihood Mission (NRLM) $1.25 a day 3. Pradhan Mantri Awaas Yojana - Gramin RD 4. National Social Assistance Programme RD Social Security Fund Social Secuity & Women (NSAP) SSW-03) Old Age Pension & Child Development. WCD-03)Financial Assistance to Widows and Destitute women SSW-04) Financial Assistance to Disabled Persons WCD-02) Financial Assistance to Dependent Children 5. Market Intervention Scheme and Price Agriculture & Agriculture and Farmers Support Scheme (MIS-PSS) Cooperation, AGR-31 Scheme for providing debt relief to Welfare the distressed farmers in the state 6. Deen Dayal Antyodaya Yojana (DAY)- Housing & Urban National Urban Livelihood Mission (NULM) Affairs, 7. Pradhan Mantri Awaas Yojana -Urban Housing & Urban HG-04 Punjab Shehri Awaas Yojana Housing & Urban Affairs, Development 8. Development of Skills (Umbrella Scheme) Skill Development & Entrepreneurship, 9. Prime Minister Employment Generation Micro, Small and Programme (PMEGP) Medium Enterprises, 10. Pradhan Mantri Rojgar Protsahan Yojana Labour & Employment Sustainable Development Goals and Revised Mapping of CSSs and Ministries of Government of India SDG SDG Linkage with SDG Targets Centrally Sponsored /Central Sector Concerned Ministries/ State Funded Schemes (with Scheme code) Concerned Department No. -

Improving Consumer Voices and Accountability in the Swachh Bharat Mission (Gramin) Findings from the Benchmarking Citizen Report Cards in Odisha and Tamil Nadu CRC-2
Improving Consumer Voices and Accountability in the Swachh Bharat Mission (Gramin) Findings from the benchmarking Citizen Report Cards in Odisha and Tamil Nadu CRC-2 Conducted By For Project Supported by June 2017 Public Affairs Foundation (PAF) Implementation of Citizen Report Card (CRC-2) as a part of Improving Consumer Voices and Accountability in Swachh Bharat Mission (Gramin) [SBM(G)] Report of Findings Submitted to Public Affairs Centre (PAC) [For Feedback please contact Meena Nair at [email protected]] June 2017 [page left blank] i Public Affairs Foundation | CRC-2 in Tamil Nadu and Odisha | PAC/BMGF | June 2017 Table of Contents List of Abbreviations ............................................................................................................................ viii Acknowledgments .................................................................................................................................. ix Executive Summary ................................................................................................................................. 1 Introduction ............................................................................................................................................ 6 Report Outline ...................................................................................................................................... 10 Section 2: Methodology ........................................................................................................................ 11 Section -

MIGRATION of NURSING and MIDWIFERY WORKFORCE in the STATE of KERALA This Report Was Prepared by Researchers from Oxford Policy Management (Krishna D
CASE STUDY | INDIA FROM BRAIN DRAIN TO BRAIN GAIN MIGRATION OF NURSING AND MIDWIFERY WORKFORCE IN THE STATE OF KERALA This report was prepared by researchers from Oxford Policy Management (Krishna D. Rao, Aarushi Bhatnagar, Radhika Arora, Swati Srivastava, Udit Ranjan), the Centre for Development Studies, Trivandrum (S. Irudaya Rajan, Sunitha Syam), the Health Systems Research India Initiative (Arun Nair, S.J. Sini Thomas), and the WHO Country Office for India (Tomas Zapata). Please address all correspondence to Krishna D. Rao ([email protected]) and Aarushi Bhatnagar ([email protected]) © WHO, all rights reserved November 2017 Contents Acknowledgements .......................................................3 6. Discussion ....................................... 29 Abbreviations ...............................................................4 6.1 Production, stock and migration of nurses ....... 29 6.1.1 Production ...................................... 29 Executive summary ........................................................5 6.1.2 Stock .............................................. 30 1. Background ........................................ 7 6.1.3 Migration ........................................ 31 6.2 Factors influencing migration patterns ............ 33 1.1 Kerala state ..................................................9 6.2.1 Endogenous push and pull factors ....... 33 1.2 Migration of health workers........................... 10 6.2.2 Exogenous push and pull factors .........34 2. Objectives ....................................... -

Original Research Paper Commerce Modi Model for Community Organization in Indian Society of Urban Rural and Tribal Development
IF : 3.62 | IC Value 70.36 Volume-5, Issue-8, August - 2016 • ISSN No 2277 - 8160 Original Research Paper Commerce Modi Model for Community Organization in Indian Society of Urban Rural and Tribal Development Jagdish Shankar Department of pathology, Rajendra institute of Medical Sciences, Ranchi-834009, Post graduate student, Department of pathology, Sonawane RIMS,Ranchi-834009 Dr. Rahul Associate Professor, Department of pathology, Rajendra institute of Yeshwantrao Medical Sciences, Ranchi-834009 Nikam ABSTRACT This model develop for the community organization or development purpose of urban rural and tribal development in the M.S.W. course very few or rare model use for development of community, So the author tri to use the govt. schemes in field work. Because field work is the soul of M.S.W. social workers use the tools and techniques in the field and take participate in development activities. Teacher’s or field instructor tri people motivate and giving opportunity to facilitated govt. schemes o this purpose social workers give the direction to seek the benefit of govt. schemes. For that purpose social worker must interpret of intermediate with people. KEYWORDS : motivate, opportunity direction, and interpret Introduction – vated cashier is processing your transaction. This type of cashier will: M – Motivate to people (Urban, Rural and Tribal) • Be friendly, creating a pleasant transaction that makes you O – Opportunity to development (Child, youth, women, Old age,) more likely to return • Process your transaction quickly, meaning that the store can D – Direction to your objectives or aims service more customers • Suggest an additional item you would like to purchase, increas- I – Investigation, inquiry, intermediate the govt. -

Q1.What Are the Features of the Government of India's National
12-06-2018 Q1.What are the features of the Government of India’s National Nutrition Strategy announced in September 2017? Does excess emphasis on sanitation help address India’s malnutrition problem? Critically comment. Q2. Despite two key measures – demonetisation and GST, India has made very slow progress towards becoming a formal economy. Discuss the reasons and measures needed to formalise economy. Q3. Critically examine the features of Bharatmala Pariyojana (BMP) initiative and its likely impact on economic growth of India. Q4. Is torture unethical? Justify. Q1.What are the features of the Government of India’s National Nutrition Strategy announced in September 2017? Does excess emphasis on sanitation help address India’s malnutrition problem? Critically comment. The rationale for investing in Nutrition is globally well recognized – both as a critical development imperative, as well as crucial for the fulfillment of human rights- especially of the most vulnerable children, girls and women. It constitutes the foundation for human development, by reducing susceptibility to infections, related morbidity, disability and mortality burden, enhancing cumulative lifelong learning capacities and adult productivity. Nutrition is acknowledged as one of the most effective entry points for human development, poverty reduction and economic development, with high economic returns. The Global Nutrition Report 2015 estimates that for investment in nutrition, there is a benefit cost ratio of 16:1 for 40 low and middle- income countries. Features of National Nutrition Strategy :- www.brainyias.com 12-06-2018 . The Strategy aims to reduce all forms of malnutrition by 2030, with a focus on the most vulnerable and critical age groups. -

2017 STATE of YOUTH VOLUNTEERING in INDIA 2017: State of Youth Volunteering in India
2017 STATE OF YOUTH VOLUNTEERING IN INDIA 2017: State Of Youth Volunteering In India STATE OF YOUTH VOLUNTEERING IN INDIA _________________ 2017 1 2017: State Of Youth Volunteering In India 2 2017: State Of Youth Volunteering In India TABLE OF CONTENTS LIST OF FIGURES LIST OF BOXES LIST OF CASE STUDIES OvervieW 14 1. YOUTH VOLUNTEERISM IN INDIA 22 Evolution of volunteerism in India 23 Defining youth volunteerism in India 26 Manifestations of volunteering by youth in India 29 Discourses around youth volunteering in current times 33 Measuring youth volunteering in India 34 Conclusion 36 2. ECOSYSTEM SURROUNDING YOUTH VOLUNTEERING IN INDIA 38 Government 40 Civil Society 53 Private Sector 62 Conclusion 64 3. YOUTH PERCEPTIONS ON VOLUNTEERING IN INDIA 66 Profile of respondents 67 Nature of volunteering 69 Volunteer motivations 71 Modes of communication about volunteering opportunities 79 Perceived barriers to volunteering and challenges faced 80 Perceptions of impact created on community and self 81 Conclusion 84 4. IMPACT OF YOUTH VOLUNTEERING initiatives IN INDIA 86 Volunteerism and education 87 Health and well-being 90 Gender equality and justice 93 Hunger 96 Water and sanitation 98 Climate change and disaster relief 100 Social entrepreneurship 103 Social inclusion 105 Peace, justice and strong institutions 108 Conclusion 111 5. CONCLUSION: Way FORWARD 114 ACKNOWLEDGMENTS 127 3 2017: State Of Youth Volunteering In India LIST OF FIGURES FIGURE 1: Ecosystem - youth volunteering 40 FIGURE 2: Age group 67 FIGURE 3: Educational qualification -
Lessons from the Swachh Bharat Mission – Driving Behaviour Change at Scale
The making of “Swachh” India Lessons from the Swachh Bharat Mission – driving behaviour change at scale October 2018 KPMG.com/in © 2018 KPMG, an Indian Registered Partnership and a member firm of the KPMG network of independent member firms affiliated with KPMG International Cooperative (“KPMG International”), a Swiss entity. All rights reserved. Foreword The Swachh Bharat Mission (SBM), which is perhaps the largest behaviour change campaign ever, aims to make India a clean nation. There is enough evidence to show that India is on a new trajectory of growth owing to the achievements under the mission. SBM has witnessed a phenomenal increase in rural sanitation coverage from 39 per cent to 90 per cent in the last four years. It is heartening to see the people of our nation stepping beyond their roles as mere beneficiaries of the programme to becoming its leaders. The large majority of citizens in rural India, especially the women, no longer have to suffer the indignity of having to go out into the open to defecate. In fact, women are becoming the primary force in driving the nation in becoming free from open defecation. It marks a sea change in their attitude which has a direct impact on their dignity and quality of life. The World Health Organization (WHO) believes that SBM could prevent about 300,000 deaths due to water borne diseases assuming we achieve 100 per cent coverage by October 2019. The credit for this will go to every Indian who was part of this campaign. I take this opportunity to congratulate the Ministry of Drinking Water and Sanitation and every citizen in the country for catalysing the achievements achieved thus far. -

Impact of an Integrated Nutrition and Health Programme on Neonatal
Impact of an integrated nutrition and health programme on neonatal mortality in rural northern India Abdullah H Baqui,a Emma K Williams,a Amanda M Rosecrans,a Praween K Agrawal,a Saifuddin Ahmed,b Gary L Darmstadt,a Vishwajeet Kumar,a Usha Kiran,c Dharmendra Panwar,c Ramesh C Ahuja,d Vinod K Srivastava,d Robert E Black a & Manthuram Santosham a Objective To assess the impact of the newborn health component of a large-scale community-based integrated nutrition and health programme. Methods Using a quasi-experimental design, we evaluated a programme facilitated by a nongovernmental organization that was implemented by the Indian government within existing infrastructure in two rural districts of Uttar Pradesh, northern India. Mothers who had given birth in the 2 years preceding the surveys were interviewed during the baseline (n = 14 952) and endline (n = 13 826) surveys. The primary outcome measure was reduction of neonatal mortality. Findings In the intervention district, the frequency of home visits by community-based workers increased during both antenatal (from 16% to 56%) and postnatal (from 3% to 39%) periods, as did frequency of maternal and newborn care practices. In the comparison district, no improvement in home visits was observed and the only notable behaviour change was that women had saved money for emergency medical treatment. Neonatal mortality rates remained unchanged in both districts when only an antenatal visit was received. However, neonates who received a postnatal home visit within 28 days of birth had 34% lower neonatal mortality (35.7 deaths per 1000 live births, 95% confidence interval, CI: 29.2–42.1) than those who received no postnatal visit (53.8 deaths per 1000 live births, 95% CI: 48.9–58.8), after adjusting for sociodemographic variables. -

National Guidelines for Smart Cities in India
GCI Thematic Round Table: A Dialogue on Smart Cities, June 29th, 2015 National Guidelines for Smart Cities in India Bharat Punjabi Post Doctoral Fellow, Institute on Municipal Finance and Governance, University of Toronto Visiting Fellow, Global Cities Institute, University of Toronto Email: [email protected] Major Objectives of the Smart Cities Mission • Retrofitting – providing services to those city pockets which are deficient in them • Redevelopment – reconstruction of those city pockets where other interventions are unlikely to bring improvements • City-wide improvements such as Intelligent Transport Solutions, and greenfield smart cities Excerpt from the Guidelines: Brownfield and Green field “ The purpose of the Smart Cities Mission is to drive economic growth and improve the quality of life of people by enabling local area development and harnessing technology, especially technology that leads to Smart outcomes. Area-based development will transform existing areas (retrofit and redevelop), including slums, into better planned ones, thereby improving liveability of the whole City. New areas (greenfield) will be developed around cities in order to accommodate the expanding population in urban areas. Application of Smart Solutions will enable cities to use technology, information and data to improve infrastructure and services ” The core infrastructure elements in a Smart City would include: • Adequate water supply, • Assured electricity supply, • Sanitation, including solid waste management, • Efficient urban mobility and public transport, • Affordable housing • Robust IT connectivity and digitalization, • Good governance, especially e-Governance and citizen participation, • Sustainable environment, • Safety and security of citizens, particularly women, children and the elderly, and • Health and education Finance and Urban Governance: Centre- State co-operation • Rs.