Nerve Injury and Neuropathy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -

Strategies to Improve Nerve Regeneration After Radical Prostatectomy: a Narrative Review
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Institutional Research Information System University of Turin Strategies to improve nerve regeneration after radical prostatectomy: a narrative review Stefano Geuna 1, 2, Luisa Muratori1, 2, Federica Fregnan 1, 2, Matteo Manfredi4 , Riccardo Bertolo 3, 4 , Francesco Porpiglia4. 1 Department of Clinical and Biological Sciences, University of Turin, Orbassano (To), 10043, Italy. 2 Neuroscience Institute Cavalieri Ottolenghi (NICO), Orbassano (To), 10043, Italy. 3 Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, US. 4 Department of Oncology, University of Turin, Orbassano (To), 10043, Italy. Abstract Peripheral nerves are complex organs that spread throughout the entire human body. They are frequently affected by lesions not only as a result of trauma but also following radical tumor resection. In fact, despite the advancement in surgical techniques, such as nerve- sparing robot assisted radical prostatectomy, some degree of nerve injury may occur resulting in erectile dysfunction with significant impairment of the quality of life. The aim of this review is to provide an overview on the mechanisms of the regeneration of injured peripheral nerves and to describe the potential strategies to improve the regeneration process and the functional recovery. Yet, the recent advances in bio- engineering strategies to promote nerve regeneration in the urological field are outlined with a view on the possible future regenerative therapies which might ameliorate the functional outcome after radical prostatectomy. 1 Introduction Radical prostatectomy is the gold standard surgical treatment for organ-confined prostate cancer. The employment of innovative surgical technique such as nerve-sparing robot assisted radical prostatectomy allowed to magnify the anatomical field leading to a three- dimensional perspective obtained through the robotic lenses and a better anatomical knowledge. -
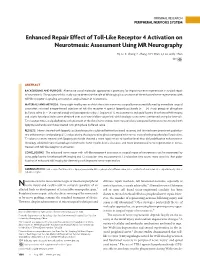
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

Some Aspects of Facial Nerve Paralysis* PART Li
13 Januarie 1973 S.-A. MEDIESE TVDSKRIF 65 Some Aspects of Facial Nerve Paralysis* PART lI. ELECTRICAL TESTS AND THE SUBMAXILLARY SALlYARY TEST M. G. POTGIETER,t M.B. CH.B. UNIV. PRET., M.MED. OTOL. UNIV. CAPE TOWN, Department of Otolaryngology, Groote Schuur Hospital, Observatory, Cape SUMMARY fibres are the first to be affected and when there is re generation, the new fibres conduct slowly.' The submaxillary salivary flow test gives reliable in The maintenance of nerve and muscle excitability de formation as to whether neurapraxia, axono:mesis, or pends greatly upon sodium and potassium cations. States neurotmesis of the facial nerve is present. This can be of polarization and depolarization are dependent on the corroborated by electrical studies. This test can make an shift of sodium and potassium cations across the cell important contribution to the topognosis and prognosis of membranes. With injury to the nerve;" elimination of facial paralysis, especially when elaborate electrical the membrane potential takes place and this causes a lack equipment for nerve excitability tests and electromyo of electrical conduction. A shift of potassium from the graphy is not available. cell takes place. An over-all increase in the potassium content of the injured nerve exists where, for instance, S. Afr. Med. J., 47, 65 (1973). bone fragments cause a foreign body reaction. Hyaluronic acid from an inflammatory response, occurs as a potas sium hyaluronate. Fibroblast and mast-cell activities in ELECTRlCAL TESTS crease and elaborate mucopolysaccharides. This may explain the high potassium values, maintained in the In 1872 Duchenne described the technique of nerve ex injured area of the nerve, inhibiting transmission. -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -
Development of a Z-Stack Projection Imaging Protocol for a Nerve Allograft
DEVELOPMENT OF A Z-STACK PROJECTION IMAGING PROTOCOL FOR A NERVE ALLOGRAFT by SELVAANISH SELVAM Submitted in partial fulfillment of the requirements for the degree of Master of Science Dissertation Advisor: Dr. George F. Muschler Department of Biomedical Engineering CASE WESTERN RESERVE UNIVERSITY August 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis of Selvaanish Selvam candidate for the degree of (Master of Science) *. Committee Chair Dr. George F. Muschler Committee Member Dr. Eben Alsberg Committee Member Dr. Robert Kirsch Committee Member Cynthia Boehm Date of Defense May 4th 2018 *we also certify that written approval has been obtained For any proprietary material contained therein 2 Table of Contents List of Tables……………………………………………………………………..4 Figures List……………………………………………………………………….5 Acknowledgments………………………………………………………………..6 List of Abbreviations………………………………………………………….....7 Abstract…………………………………………………………………………...8 Introduction……………………………………………………………………..10 Methods………………………………………………………………………….21 Data and Analysis………………………………………………………………31 Conclusions and Future Directions……………………………………………51 References……………………………………………………………………….53 3 List of Tables Table 1: Overall summary of ratios and retention rates……………………..31 Table 2: Selection Ratio for grafts (3X – 10-minute rinse) ………………….35 Table 3: Selection Ratio for grafts (15-minute soak) ………………………...35 4 List of Figures: Figure 1: 2D 10X DAPI stained image using current techniques…….……….9 Figure 2: Peripheral Nerve Anatomy………………………………………….10 -

Restoration of Neurological Function Following Peripheral Nerve Trauma
International Journal of Molecular Sciences Review Restoration of Neurological Function Following Peripheral Nerve Trauma Damien P. Kuffler 1,* and Christian Foy 2 1 Institute of Neurobiology, Medical Sciences Campus, University of Puerto Rico, 201 Blvd. del Valle, San Juan, PR 00901, USA 2 Section of Orthopedic Surgery, Medical Sciences Campus, University of Puerto Rico, San Juan, PR 00901, USA; [email protected] * Correspondence: dkuffl[email protected] Received: 12 January 2020; Accepted: 3 March 2020; Published: 6 March 2020 Abstract: Following peripheral nerve trauma that damages a length of the nerve, recovery of function is generally limited. This is because no material tested for bridging nerve gaps promotes good axon regeneration across the gap under conditions associated with common nerve traumas. While many materials have been tested, sensory nerve grafts remain the clinical “gold standard” technique. This is despite the significant limitations in the conditions under which they restore function. Thus, they induce reliable and good recovery only for patients < 25 years old, when gaps are <2 cm in length, and when repairs are performed <2–3 months post trauma. Repairs performed when these values are larger result in a precipitous decrease in neurological recovery. Further, when patients have more than one parameter larger than these values, there is normally no functional recovery. Clinically, there has been little progress in developing new techniques that increase the level of functional recovery following peripheral nerve injury. This paper examines the efficacies and limitations of sensory nerve grafts and various other techniques used to induce functional neurological recovery, and how these might be improved to induce more extensive functional recovery. -

Painful Abdominal Wall Nerves
CASE REPORT Reconstructive Treatment of Painful Nerves in the Abdominal Wall Using Processed Nerve Allografts Andrew Bi, BS Eugene Park, MD Summary: Neuromas can be a debilitating cause of pain and often negatively af- Gregory A. Dumanian, MD fect patients’ quality of life. One effective method of treatment involves surgical resection of the painful neuroma and use of a processed nerve allograft to repair the injured nerve segment. Giving the nerve “somewhere to go and something to do” has been shown to effectively alleviate pain in upper and lower extremities. We present the first report of this concept to treat a painful neuroma of the ab- dominal wall that developed following a laparoscopic gastric bypass. The neuroma was excised, and the affected nerve was reconstructed using a processed nerve allograft as an interposition graft, with resolution of pain and gradual return of normal sensation. Patient-reported outcomes were measured using the Patient Reported Outcomes Measurement Information System. Neuroma excision with concurrent interposition grafting using processed nerve allografts may be a promising method of treatment for postsurgical painful neuromas of the trunk. Bi et al. (Plast Reconstr Surg Glob Open 2018;6:e1670; doi: 10.1097/GOX.0000000000001670; Published online 6 March 2018.) INTRODUCTION and unacceptable repeat surgical rates.2 And while wrap- Painful neuromas can form following any surgery when ping the distal point of a painful nerve postneuroma exci- nerves are injured due to cautery or traction. Nerve injury sion -
Nerve Evaluation Protocol 2014
Nerve Evaluation Protocol 2014 TABLE OF CONTENTS INTRODUCTION .................................................................................................... 1 A REVIEW OF SENSORY NERVE INJURY ................................................................ 3 TERMINOLOGY ...................................................................................................... 5 INFORMED CONSENT ............................................................................................ 6 PREOPERATIVE EVALUATION ................................................................................ 7 TESTS FOR SENSORY NERVE FUNCTION: ........................................................... 12 MATERIALS NEEDED FOR TESTING SENSORY PERCEPTION .............................. 17 TESTING TECHNIQUE .......................................................................................... 20 REFERENCES .......................................................................................................... 23 BIBLIOGRAPHY - CORONECTOMY ..................................................................... 28 SAMPLE SENSORY RECORDING SHEETS ............................................................. 30 A HANDOUT FOR PATIENTS ............................................................................... 33 INTRODUCTION The first edition of this document was produced in the Spring of 1988. Dr. A. F. Steunenberg and Dr. M. Anthony Pogrel collaborated to produce the first edition with input from Mr. Art Curley, Esquire, and with Dr. Charles Alling editing -

Cryoneurolysis and Percutaneous Peripheral Nerve Stimulation To
REVIEW ARTICLE Deborah J. Culley, M.D., Editor ABSTRACT Two regional analgesic modalities currently cleared by the U.S. Food and Drug Administration hold promise to provide postoperative analgesia free of many of the limitations of both opioids and local anesthetic-based techniques. Cryoneurolysis and Cryoneurolysis uses exceptionally low temperature to reversibly ablate a peripheral nerve, resulting in temporary analgesia. Where applicable, it offers Percutaneous Peripheral a unique option given its extended duration of action measured in weeks to months after a single application. Percutaneous peripheral nerve stimula- Nerve Stimulation to Treat tion involves inserting an insulated lead through a needle to lie adjacent to a peripheral nerve. Analgesia is produced by introducing electrical current with Downloaded from http://pubs.asahq.org/anesthesiology/article-pdf/133/5/1127/513611/20201100.0-00028.pdf by guest on 27 September 2021 Acute Pain an external pulse generator. It is a unique regional analgesic in that it does not induce sensory, motor, or proprioception deficits and is cleared for up to A Narrative Review 60 days of use. However, both modalities have limited validation when applied to acute pain, and randomized, controlled trials are required to define both Brian M. Ilfeld, M.D., M.S., John J. Finneran IV, M.D. benefits and risks. (ANESTHESIOLOGY 2020; 133:1127–49) ANESTHESIOLOGY 2020; 133:1127–49 OTENT site-specific analgesia may be provided with at the probe tip results in a corresponding volume expansion Pregional anesthetics -

Intralipid Infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia?
Journal of ISSN: 2581-7310 Inno Volume 1: 1 Health Science and Development J Health Sci Dev 2018 Intralipid Infusion for Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia? Joseph Eldor1* 1Theoretical Medicine Institute, Jerusalem, Israel Abstract Article Information Multiple sclerosis is a demyelinating disease in which the insulating Article Type: Research covers of nerve cells in the brain and spinal cord are damaged. Article Number: JHSD105 Trigeminal neuralgia involves loss of the myelin around the trigeminal Received Date: 05 Febuary, 2018 nerve. Myelin is a phospholipid membrane that wraps around axons to Accepted Date: 23 Febuary, 2018 provide them with insulation. It is produced by Schwann cells in the PNS, Published Date: 26 Febuary, 2018 and by oligodendrocytes in the CNS. *Corresponding author: Dr. Joseph Eldor, Theoretical Medicine Institute, Jerusalem, Israel. Tel: +972-2-5835528; a way for myelin sheath repair in multiple sclerosis and trigeminal Email: csen_international(at)csen.com neuralgia.Intralipid treatment is first suggested in the medical literature as Keywords: Intralipid, Fat Emulsion, Myelin, Multiple Sclerosis, Citation: Joseph Eldor (2018) Intralipid Infusion for Trigeminal Neuralgia, Mitochondria. Myelin Sheath Repair in Multiple Sclerosis and Trigeminal Neuralgia? J Health Sci Dev Vol: 1, Issu: 1 (25-42). Multiple Sclerosis Multiple sclerosis (MS) is a demyelinating disease in which the Copyright: © 2018 Joseph Eldor. This is an open-access insulating covers of nerve cells in the brain and spinal cord are damaged article distributed under the terms of the Creative Commons [1]. This damage disrupts the ability of parts of the nervous system to Attribution License, which permits unrestricted use, communicate, resulting in a range of signs and symptoms, including distribution, and reproduction in any medium, provided the original author and source are credited.