Current and Future Imaging of the Peripheral Nervous System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

An Improved Technique for Radial Nerve Conduction Studies
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.30.4.332 on 1 August 1967. Downloaded from J. Neurol. Neurosurg. Psychiat., 1967, 30, 332 An improved technique for radial nerve conduction studies ALLAN W. DOWNIE1 AND THOMAS R. SCOTT From the Division of Neurology, Department of Medicine, School of Medicine, University ofNorth Carolina, Chapel Hill, North Carolina, U.S.A. A technique for recording evoked sensory potentials MATERIALS AND METHOD from the radial nerve has already been reported by us (Downie and Scott, 1964). This technique, The apparatus used was a TECA two-channel electro- myograph. The recording electrodes consisted of a pair although reliable, is time consuming and occasion- of chlorided silver discs 1 cm. in diameter, mounted ally difficult and the amplitude of potentials may be 2 5 cm. apart on a plastic base. The active recording as low as 1 to 2 microvolts. The purpose of this electrode was placed over the largest palpable branch communication is to describe a simpler technique by of the radial nerve as it crossed the tendon of the extensor which potentials of greater amplitude can be pollicis longus. The distal recording electrode was placed obtained. In addition, the segment of nerve tested is over the first dorsal interosseous muscle but not neces- Protected by copyright. one which can be readily identified and biopsied if sarily over the nerve, of which the position in this area so desired without causing unpleasant or disturbing cannot be precisely determined (Fig. 1). An experiment sensory loss to the subject. made to assess the importance of the position of this electrode showed no significant difference in latency to The location of a nerve which is to be tested is peak when it was placed in turn on three points along usually determined by stimulating its motor fibres a line between the tendons of the extensor pollicis and finding the stimulus site from which maximal longus and extensor indicis provided the interelectrode muscle contraction is obtained. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -
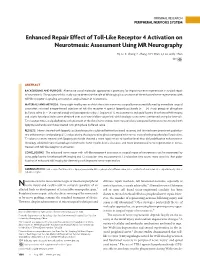
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

A Guide to Transthyretin Amyloidosis
A Guide to Transthyretin Amyloidosis Authored by Teresa Coelho, Bo-Goran Ericzon, Rodney Falk, Donna Grogan, Shu-ichi Ikeda, Mathew Maurer, Violaine Plante-Bordeneuve, Ole Suhr, Pedro Trigo 2016 Edition Edited by Merrill Benson, Mathew Maurer What is amyloidosis? Amyloidosis is a systemic disorder characterized by extra cellular deposition of a protein-derived material, known as amyloid, in multiple organs. Amyloidosis occurs when native or mutant poly- peptides misfold and aggregate as fibrils. The amyloid deposits cause local damage to the cells around which they are deposited leading to a variety of clinical symptoms. There are at least 23 different proteins associated with the amyloidoses. The most well-known type of amyloidosis is associated with a hematological disorder, in which amyloid fibrils are derived from monoclonal immunoglobulin light-chains (AL amyloidosis). This is associated with a clonal plasma cell disorder, closely related to and not uncommonly co-existing with multiple myeloma. Chronic inflammatory conditions such as rheumatoid arthritis or chronic infections such as bronchiectasis are associated with chronically elevated levels of the inflammatory protein, serum amyloid A, which may misfold and cause AA amyloidosis. The hereditary forms of amyloidosis are autosomal dominant diseases characterized by deposition of variant proteins, in dis- tinctive tissues. The most common hereditary form is transthyretin amyloidosis (ATTR) caused by the misfolding of protein monomers derived from the tetrameric protein transthyretin (TTR). Mutations in the gene for TTR frequently re- sult in instability of TTR and subsequent fibril formation. Closely related is wild-type TTR in which the native TTR protein, particu- larly in the elderly, can destabilize and re-aggregate causing non- familial cases of TTR amyloidosis. -

Expert Consensus Recommendations to Improve Diagnosis of ATTR Amyloidosis with Polyneuropathy
Journal of Neurology https://doi.org/10.1007/s00415-019-09688-0 REVIEW Expert consensus recommendations to improve diagnosis of ATTR amyloidosis with polyneuropathy David Adams1 · Yukio Ando2 · João Melo Beirão3 · Teresa Coelho4 · Morie A. Gertz5 · Julian D. Gillmore6 · Philip N. Hawkins6 · Isabelle Lousada7 · Ole B. Suhr8 · Giampaolo Merlini9,10 Received: 10 December 2019 / Revised: 20 December 2019 / Accepted: 23 December 2019 © The Author(s) 2020 Abstract Amyloid transthyretin (ATTR) amyloidosis with polyneuropathy (PN) is a progressive, debilitating, systemic disease wherein transthyretin protein misfolds to form amyloid, which is deposited in the endoneurium. ATTR amyloidosis with PN is the most serious hereditary polyneuropathy of adult onset. It arises from a hereditary mutation in the TTR gene and may involve the heart as well as other organs. It is critical to identify and diagnose the disease earlier because treatments are available to help slow the progression of neuropathy. Early diagnosis is complicated, however, because presentation may vary and family history is not always known. Symptoms may be mistakenly attributed to other diseases such as chronic infammatory demyelinating polyradiculoneuropathy (CIDP), idiopathic axonal polyneuropathy, lumbar spinal stenosis, and, more rarely, diabetic neuropathy and AL amyloidosis. In endemic countries (e.g., Portugal, Japan, Sweden, Brazil), ATTR amyloidosis with PN should be suspected in any patient who has length-dependent small-fber PN with autonomic dysfunction and a family history of ATTR amyloidosis, unexplained weight loss, heart rhythm disorders, vitreous opacities, or renal abnormali- ties. In nonendemic countries, the disease may present as idiopathic rapidly progressive sensory motor axonal neuropathy or atypical CIDP with any of the above symptoms or with bilateral carpal tunnel syndrome, gait disorders, or cardiac hypertro- phy. -
Practical Neurology: Peripheral Neuropathy for the Internist
Practical Neurology: Polyneuropathy for the Non-Neurologist Steven A. Day, MD Providence Neurological Specialties Definitions Foundational Principle: With neurological problems think of LOCALIZATION before SYNDROME Definitions • Neuronopathy – Motor neuronopathy – Sensory neuronopathy • Radiculopathy • Plexopathy • Neuropathy – Mononeuropathy – Polyneuropathy The Netter Collection of Medical Illustrations, Volume 1, Nervous System, 2002 “ROOTS” C4 TRUNKS C5 Dorsal scapular n. C6 TRUNKS C7 Suprascapular n. T1 DIVISIONS Musculocut- aneous n. CCF CORDS 2002 Long thoracic n. TERMINAL NERVES CCF ©2002 Axillary n. Radial n. Median n. Ulnar n. Definitions ‘Neuropathy’ is a diagnosis which specifies the location of pathology, not a symptom Definitions • Axonal = axon loss pathology • Demyelinating = myelin loss pathology Topical Diagnosis in Neurology, 3rd ed. 1998 Topical Diagnosis in Neurology, 3rd ed. 1998 Duss’ Topical Diagnosis in Neurology, 4th ed. 2005 Polyneuropathy Polyneuropathy: Typical Presentation • Insidious onset • Distal (toes, pads of feet) • Gradual progression • Complaints are primarily sensory Polyneuropathy: Key Exam Features • Sensory – Distal gradient of sensory loss • Pin prick or cold • Monofilament • Cotton wisp • Vibration at toes and ankles • Proprioception: toe movements Polyneuropathy: Key Exam Features • Motor – Is there intrinsic foot or hand muscle atrophy? – Weakness pattern • Distal • Proximal and distal • Asymmetric – Able to stand/elevate on toes and heels? Polyneuropathy: Key Exam Features • Reflexes – Distal -

The Usefulness of Proximal Radial Motor Conduction in Acute Compressive Radial Neuropathy
JCN Open Access ORIGINAL ARTICLE pISSN 1738-6586 / eISSN 2005-5013 / J Clin Neurol 2015;11(2):178-182 / http://dx.doi.org/10.3988/jcn.2015.11.2.178 The Usefulness of Proximal Radial Motor Conduction in Acute Compressive Radial Neuropathy Kun Hyun Kima b Background and PurposezzThe objective of this study was to determine diagnostic and Kee-Duk Park a prognostic values of proximal radial motor conduction in acute compressive radial neuropathy. Pil-Wook Chung a MethodszzThirty-nine consecutive cases of acute compressive radial neuropathy with radial Heui-Soo Moon conduction studies–including stimulation at Erb’s point–performed within 14 days from a Yong Bum Kim clinical onset were reviewed. The radial conduction data of 39 control subjects were used as a Won Tae Yoon reference data. b Hyung Jun Park ResultszzThirty-one men and eight women (age, 45.2±12.7 years, mean±SD) were enrolled. Bum Chun Suha All 33 patients in whom clinical follow-up data were available experienced complete recov- ery, with a recovery time of 46.8±34.3 days. Partial conduction block was found frequently a Department of Neurology, Kangbuk Samsung Hospital, (17 patients) on radial conduction studies. The decrease in the compound muscle action po- Sungkyunkwan University tential area between the arm and Erb’s point was an independent predictor for recovery time. School of Medicine, Seoul, Korea zzProximal radial motor conduction appears to be a useful method for the early b Conclusions Department of Neurology, detection and prediction of prognosis of acute compressive radial neuropathy. Mokdong Hospital, Ewha Womans University Key Wordszz radial neuropathy, nerve conduction study, conduction block, diagnosis, School of Medicine, Seoul, Korea prognosis. -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -
Development of a Z-Stack Projection Imaging Protocol for a Nerve Allograft
DEVELOPMENT OF A Z-STACK PROJECTION IMAGING PROTOCOL FOR A NERVE ALLOGRAFT by SELVAANISH SELVAM Submitted in partial fulfillment of the requirements for the degree of Master of Science Dissertation Advisor: Dr. George F. Muschler Department of Biomedical Engineering CASE WESTERN RESERVE UNIVERSITY August 2018 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the thesis of Selvaanish Selvam candidate for the degree of (Master of Science) *. Committee Chair Dr. George F. Muschler Committee Member Dr. Eben Alsberg Committee Member Dr. Robert Kirsch Committee Member Cynthia Boehm Date of Defense May 4th 2018 *we also certify that written approval has been obtained For any proprietary material contained therein 2 Table of Contents List of Tables……………………………………………………………………..4 Figures List……………………………………………………………………….5 Acknowledgments………………………………………………………………..6 List of Abbreviations………………………………………………………….....7 Abstract…………………………………………………………………………...8 Introduction……………………………………………………………………..10 Methods………………………………………………………………………….21 Data and Analysis………………………………………………………………31 Conclusions and Future Directions……………………………………………51 References……………………………………………………………………….53 3 List of Tables Table 1: Overall summary of ratios and retention rates……………………..31 Table 2: Selection Ratio for grafts (3X – 10-minute rinse) ………………….35 Table 3: Selection Ratio for grafts (15-minute soak) ………………………...35 4 List of Figures: Figure 1: 2D 10X DAPI stained image using current techniques…….……….9 Figure 2: Peripheral Nerve Anatomy………………………………………….10 -

Restoration of Neurological Function Following Peripheral Nerve Trauma
International Journal of Molecular Sciences Review Restoration of Neurological Function Following Peripheral Nerve Trauma Damien P. Kuffler 1,* and Christian Foy 2 1 Institute of Neurobiology, Medical Sciences Campus, University of Puerto Rico, 201 Blvd. del Valle, San Juan, PR 00901, USA 2 Section of Orthopedic Surgery, Medical Sciences Campus, University of Puerto Rico, San Juan, PR 00901, USA; [email protected] * Correspondence: dkuffl[email protected] Received: 12 January 2020; Accepted: 3 March 2020; Published: 6 March 2020 Abstract: Following peripheral nerve trauma that damages a length of the nerve, recovery of function is generally limited. This is because no material tested for bridging nerve gaps promotes good axon regeneration across the gap under conditions associated with common nerve traumas. While many materials have been tested, sensory nerve grafts remain the clinical “gold standard” technique. This is despite the significant limitations in the conditions under which they restore function. Thus, they induce reliable and good recovery only for patients < 25 years old, when gaps are <2 cm in length, and when repairs are performed <2–3 months post trauma. Repairs performed when these values are larger result in a precipitous decrease in neurological recovery. Further, when patients have more than one parameter larger than these values, there is normally no functional recovery. Clinically, there has been little progress in developing new techniques that increase the level of functional recovery following peripheral nerve injury. This paper examines the efficacies and limitations of sensory nerve grafts and various other techniques used to induce functional neurological recovery, and how these might be improved to induce more extensive functional recovery. -

Painful Abdominal Wall Nerves
CASE REPORT Reconstructive Treatment of Painful Nerves in the Abdominal Wall Using Processed Nerve Allografts Andrew Bi, BS Eugene Park, MD Summary: Neuromas can be a debilitating cause of pain and often negatively af- Gregory A. Dumanian, MD fect patients’ quality of life. One effective method of treatment involves surgical resection of the painful neuroma and use of a processed nerve allograft to repair the injured nerve segment. Giving the nerve “somewhere to go and something to do” has been shown to effectively alleviate pain in upper and lower extremities. We present the first report of this concept to treat a painful neuroma of the ab- dominal wall that developed following a laparoscopic gastric bypass. The neuroma was excised, and the affected nerve was reconstructed using a processed nerve allograft as an interposition graft, with resolution of pain and gradual return of normal sensation. Patient-reported outcomes were measured using the Patient Reported Outcomes Measurement Information System. Neuroma excision with concurrent interposition grafting using processed nerve allografts may be a promising method of treatment for postsurgical painful neuromas of the trunk. Bi et al. (Plast Reconstr Surg Glob Open 2018;6:e1670; doi: 10.1097/GOX.0000000000001670; Published online 6 March 2018.) INTRODUCTION and unacceptable repeat surgical rates.2 And while wrap- Painful neuromas can form following any surgery when ping the distal point of a painful nerve postneuroma exci- nerves are injured due to cautery or traction. Nerve injury sion