A Systematic Approach to a Painful Wrist
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4Th SESSION 1
2019 IWIW Meeting Abstracts, Las Vegas, Wed. Sept. 4th SESSION 1: Carpal Ligament 1 Stable Central Column Theory of Carpal Mechanics Michael Sandow FRACS Wakefield Orthopaedic Clinic Adelaide, Australia Background: The carpus is a complicated and functionally challenged mechanical system and advancements in the understanding have been compromised by the recognition that there is no standard carpal mechanical system and no typical wrist. This paper cover component of a larger project that seeks to develop a kinetic model of wrist mechanics to allow reverse analysis of the specific biomechanical controls or rule of a specific patient's carpus, and then use those to create a forward mathematical model to reproduce the unique individual's anatomical motion based on the extracted rules. Objectives and Methods: Based on previous observations, the carpus essentially moves with only 2 degrees of freedom - pitch (flexion / extension) and yaw (radial deviation / ulnar deviation), while largely preventing roll (pronation / supination). The object of this paper is therefore to present the background and justification to support the rules based motion (RBM) concept states that the motion of a mechanical system, such as the wrist, is the net interplay of 4 rules - morphology, constraint, interaction and load. The Stable Central Column Theory (SCCT) of wrist mechanics applies the concept of RBM to the carpus, and by using a reverse engineering computational analysis model, identified a consistent pattern of isometric constraints, creating a "Two-Gear Four-Bar" linkage. This study assessed the motion of the carpus using a 3D dynamic visualization model, and the hypothesis was that the pattern and direction of motion of the proximal row, and the distal row with respect the immediately cephalad carpal bones or radius would be very similar in all directions of wrist motion. -

Table 9-10 Ligaments of the Wrist and Their Function
Function and Movement of the Hand 283 Table 9-10 Ligaments of the Wrist and Their Function Extrinsic Ligaments Function Palmar radiocarpal Volarly stabilizes radius to carpal bones; limits excessive wrist extension Dorsal radiocarpal Dorsally stabilizes radius to carpal bones; limits excessive wrist flexion Ulnar collateral Provides lateral stability of ulnar side of wrist between ulna and carpals Radial collateral Provides lateral stability of radial side of wrist between radius and carpals Ulnocarpal complex and articular Stabilizes and helps glide the ulnar side of wrist; stabilizes distal disk (or triangular fibrocartilage radioulnar joint complex) Intrinsic Ligaments Palmar midcarpal Forms and stabilizes the proximal and distal rows of carpal bones Dorsal midcarpal Forms and stabilizes the proximal and distal rows of carpal bones Interosseous Intervenes between each carpal bone contained within its proximal or distal row Accessory Ligament Transverse carpal Stabilizes carpal arch and contents of the carpal tunnel Adapted from Hertling, D., & Kessler, R. (2006). Management of common musculoskeletal disorders: Physical therapy principles and methods. Philadelphia, PA: Lippincott, Williams & Wilkins.; Oatis, C. A. (2004). Kinesiology: The mechanics and pathomechanics of human movement. Philadelphia, PA: Lippincott, Williams & Wilkins.; Weiss, S., & Falkenstein, N. (2005). Hand rehabilitation: A quick reference guide and review. St. Louis, MO: Mosby Elsevier. The radial and ulnar collateral ligaments provide lateral and medial support, respectively, to the wrist joint. The ulnocarpal complex is more likely to be referred to as the triangular fibro- cartilage complex (TFCC) and includes the articular disk of the wrist. The TFCC is the major stabilizer of the distal radioulnar joint (DRUJ) and can tear after direct compressive force such as a fall on an outstretched hand. -

Isolated Trapezoid Fractures a Case Report with Compilation of the Literature
Bulletin of the NYU Hospital for Joint Diseases 2008;66(1):57-60 57 Isolated Trapezoid Fractures A Case Report with Compilation of the Literature Konrad I. Gruson, M.D., Kevin M. Kaplan, M.D., and Nader Paksima, D.O., M.P.H. Abstract as an axial load5,6 or bending stress7 transmitted indirectly Isolated fractures of the trapezoid bone have been rarely to the trapezoid through the second metacarpal. We present reported in the literature, the mechanism of injury being a case of an acute, isolated trapezoid fracture that resulted an axial or bending load transmitted through the second from direct trauma to the distal carpus and that was treated metacarpal. We report a case of an isolated, nondisplaced nonoperatively. Additionally, strategies for diagnosis and trapezoid fracture that was sustained by direct trauma treatment, as well as a synthesis of the published results and subsequently treated successfully in a short-arm cast. for both isolated and concomitant trapezoid fractures, are Diagnostic and treatment strategies for isolated fractures presented. of the trapezoid bone are reviewed as well as the results of operative and nonoperative treatment. Case Report A 25-year-old right-hand dominant male presented to the ractures of the carpus most commonly involve the emergency room (ER) complaining of isolated right-wrist scaphoid,1 with typical physical examination findings pain and swelling of 1 day’s duration. The patient stated Fof “snuffbox” tenderness. This presentation is fre- that a heavy metal door at work had closed onto the back quently the result of the patient falling onto an outstretched of his wrist causing an immediate onset of swelling and hand. -

Carpals and Tarsals of Mule Deer, Black Bear and Human: an Osteology Guide for the Archaeologist
Western Washington University Western CEDAR WWU Graduate School Collection WWU Graduate and Undergraduate Scholarship 2009 Carpals and tarsals of mule deer, black bear and human: an osteology guide for the archaeologist Tamela S. Smart Western Washington University Follow this and additional works at: https://cedar.wwu.edu/wwuet Part of the Anthropology Commons Recommended Citation Smart, Tamela S., "Carpals and tarsals of mule deer, black bear and human: an osteology guide for the archaeologist" (2009). WWU Graduate School Collection. 19. https://cedar.wwu.edu/wwuet/19 This Masters Thesis is brought to you for free and open access by the WWU Graduate and Undergraduate Scholarship at Western CEDAR. It has been accepted for inclusion in WWU Graduate School Collection by an authorized administrator of Western CEDAR. For more information, please contact [email protected]. MASTER'S THESIS In presenting this thesis in partial fulfillment of the requirements for a master's degree at Western Washington University, I grant to Western Washington University the non-exclusive royalty-free right to archive, reproduce, distribute, and display the thesis in any and all forms, including electronic format, via any digital library mechanisms maintained by WWu. I represent and warrant this is my original work, and does not infringe or violate any rights of others. I warrant that I have obtained written permissions from the owner of any third party copyrighted material included in these files. I acknowledge that I retain ownership rights to the copyright of this work, including but not limited to the right to use all or part of this work in future works, such as articles or books. -

REVIEW ARTICLE Osteoarthritis of the Wrist
REVIEW ARTICLE Osteoarthritis of the Wrist Krista E. Weiss, Craig M. Rodner, MD From Harvard College, Cambridge, MA and Department of Orthopaedic Surgery, University of Connecticut Health Center, Farmington, CT. Osteoarthritis of the wrist is one of the most common conditions encountered by hand surgeons. It may result from a nonunited or malunited fracture of the scaphoid or distal radius; disruption of the intercarpal, radiocarpal, radioulnar, or ulnocarpal ligaments; avascular necrosis of the carpus; or a developmental abnormality. Whatever the cause, subsequent abnormal joint loading produces a spectrum of symptoms, from mild swelling to considerable pain and limitations of motion as the involved joints degenerate. A meticulous clinical and radiographic evaluation is required so that the pain-generating articulation(s) can be identi- fied and eliminated. This article reviews common causes of wrist osteoarthritis and their surgical treatment alternatives. (J Hand Surg 2007;32A:725–746. Copyright © 2007 by the American Society for Surgery of the Hand.) Key words: Wrist, osteoarthritis, arthrodesis, carpectomy, SLAC. here are several different causes, both idio- of events is analogous to SLAC wrist and has pathic and traumatic, of wrist osteoarthritis. been termed scaphoid nonunion advanced collapse Untreated cases of idiopathic carpal avascular (SNAC). Wrist osteoarthritis can also occur second- T 1 2 necrosis, as in Kienböck’s or Preiser’s disease, may ary to an intra-articular fracture of the distal radius or result in radiocarpal arthritis. Congenital wrist abnor- ulna or from an extra-articular fracture resulting in malities, such as Madelung’s deformity,3,4 can lead malunion and abnormal joint loading. -
Carpus Volume: 7 to 10 Ml for Each Joint Degree of Difficulty: 1/3 Dorsal Approach
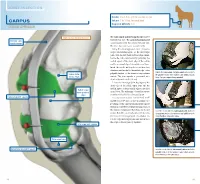
JOINT INJECTION needle: 1 to 1.5 in. (2.5 to 3.8 cm), 20 ga Carpus volume: 7 to 10 ml for each joint Degree of difficulty: 1/3 Dorsal approach right carpus, dorsomedial view The radiocarpal and intercarpal joints can be extensor carpi entered with ease. The carpometacarpal joint radialis tendon communicates with the intercarpal joint and, therefore, does not require separate entry. Using the dorsal approach, enter the radio- carpal (antebrachiocarpal) or the intercarpal joints with the limb held and the carpus flexed. Locate the radiocarpal joint by palpating the medial aspect of the distal edge of the radius and the proximal edge of the radial carpal bone. Insert the needle midway between these two structures and medial to the medial edge of the palpate the radiocarpal and intercarpal joints medial to palpable tendon of the extensor carpi radialis radius (distal the palpable tendon of the extensor carpi radialis muscle. medial edge) muscle. The joint capsule is penetrated at a Note: The right carpus is being palpated. depth of about 0.5 inch (1.3 cm). Locate the intercarpal joint by palpating the distal edge of the radial carpal bone and the medial aspect of the proximal edge of the third radial carpal bone (proximal carpal bone. The technique of needle insertion edge) is similar to that for the radiocarpal joint. radiocarpal joint capsule It is important to point out that Ford et al47 and Moyer et al48 showed that the palmar out- pouchings of the carpometacarpal joint capsule extend into the fibers of the proximal portion of the suspensory ligament. -

Readingsample
Color Atlas of Human Anatomy Vol. 1: Locomotor System Bearbeitet von Werner Platzer 6. durchges. Auflage 2008. Buch. ca. 480 S. ISBN 978 3 13 533306 9 Zu Inhaltsverzeichnis schnell und portofrei erhältlich bei Die Online-Fachbuchhandlung beck-shop.de ist spezialisiert auf Fachbücher, insbesondere Recht, Steuern und Wirtschaft. Im Sortiment finden Sie alle Medien (Bücher, Zeitschriften, CDs, eBooks, etc.) aller Verlage. Ergänzt wird das Programm durch Services wie Neuerscheinungsdienst oder Zusammenstellungen von Büchern zu Sonderpreisen. Der Shop führt mehr als 8 Millionen Produkte. 130 Upper Limb: Bones, Ligaments, Joints Radiocarpal and Midcarpal Joints Ligaments in the Region of the Wrist (A–E) (A–E) Four groups of ligaments can be distin- The radiocarpal or wrist joint is an ellip- guished: soid joint formed on one side by the radius (1) and the articular disk (2) and on the Ligaments which unite the forearm bones with other by the proximal row of carpal bones.Not the carpal bones (violet). These include the all the carpal bones of the proximal row are ulnar collateral ligament (8), the radial col- in continual contact with the socket- lateral ligament (9), the palmar radiocarpal shaped articular facet of the radius and the ligament (10), the dorsal radiocarpal liga- disk. The triquetrum (3), only makes close ment (11), and the palmar ulnocarpal liga- contact with the disk during ulnar abduc- ment (12). tion and loses contact on radial abduction. Ligaments which unite the carpal bones with The capsule of the wrist joint is lax, dorsally one another,orintercarpal ligaments (red). These comprise the radiate carpal ligament Upper Limb relatively thin, and is reinforced by numer- ous ligaments. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Bones and Joints of the Upper Limb: Forearm and Hand
Unit 4: Bones and joints of the upper limb: forearm and hand Chapter 6 (Upper limb) GENERAL OBJECTIVES: - recognize, name and correctly orient forearm and hand bones - understand movements in elbow, wrist and hand joints SPECIFIC OBJECTIVES: Bones of the forearm and hand Identify the bony features on each part of the following bones: RADIUS - Upper End - Shaft - Lower End ULNA - Upper End - Shaft - Lower End Deduce (from the shape of the articular surfaces) the movements at (i) the elbow joint and (ii) the radioulnar joints. Indicate the bony attachments of the major ligaments which help to maintain the stability of these joints (while allowing their mobility). Identify the following bones CARPALS - Proximal Row - Distal Row METACARPALS PHALANGES Identify the attachments of the Flexor Retinaculum and define the "Carpal Tunnel". Deduce (from the shape of the articular surfaces) the movements at (i) the wrist joint (ii) the carpometacarpal joint of the thumb (iii) metacarpophalangeal joints (iv) interphalangeal joints Indicate the bony attachments of the major ligaments which help to maintain the stability of these joints (while allowing their mobility). Joints of the forearm and hand Elbow Joint Articular Surfaces (Humeroulnar & Humeroradial) Fibrous Capsule & Joint Cavity Synovial Membrane Collateral Ligaments ( Medial & Lateral) Special Structures: Olecranon Bursa Other Bursae, Pads of Fat Movements at the Elbow Joint: Flexion/Extension Stability Carrying Angle Radioulnar Joints Proximal Radioulnar Joint Annular Ligament Distal Radioulnar -
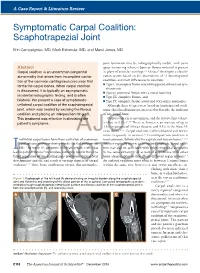
Symptomatic Carpal Coalition: Scaphotrapezial Joint
A Case Report & Literature Review E. Campaigniac et al Symptomatic Carpal Coalition: Scaphotrapezial Joint Erin Campaigniac, MD, Mark Eskander, MD, and Marci Jones, MD joint formation may be radiographically visible, with joint Abstract space narrowing wherein bone or fibrous material is present Carpal coalition is an uncommon congenital in place of articular cartilage.2,4 Minaar8 developed a classifi- abnormality that arises from incomplete cavita- cation system based on his observations of 12 lunotriquetral tion of the common cartilaginous precursor that coalitions and their differences in coalition: ◾ Type I, incomplete fusion resembling pseudarthrosis or syn- forms the carpal bones. When carpal coalition chondrosis is discovered, it is typically an asymptomatic ◾ Type II, proximal fusion with a distal notching incidental radiographic finding, and is often ◾ Type III, complete fusion, and bilateral. We present a case of symptomatic ◾ Type IV, complete fusion associated with other anomalies. unilateral carpal coalition of the scaphotrapezial Although these 4 types were based on lunotriquetral coali- joint, which was treated by excising the fibrous tions, this classification system is used to describe the coalition coalition and placing an interposition fat graft. of any carpal bone. This treatment was effective in alleviating the Carpal coalition is uncommon, and the reported prevalence 2,5,6,9 patient’s symptoms. is close to 0.1%. There is, however, an increase of up to 1.5% in patients of African descent, and 9.5% in the West Af- rican -

Carpal Fractures
CURRENT CONCEPTS Carpal Fractures Nina Suh, MD, Eugene T. Ek, MBBS, PhD, Scott W. Wolfe, MD CME INFORMATION AND DISCLOSURES The Review Section of JHS will contain at least 3 clinically relevant articles selected by the Provider Information can be found at http://www.assh.org/Pages/ContactUs.aspx. editor to be offered for CME in each issue. For CME credit, the participant must read the Technical Requirements for the Online Examination can be found at http://jhandsurg. articles in print or online and correctly answer all related questions through an online org/cme/home. examination. The questions on the test are designed to make the reader think and will occasionally require the reader to go back and scrutinize the article for details. Privacy Policy can be found at http://www.assh.org/pages/ASSHPrivacyPolicy.aspx. The JHS CME Activity fee of $30.00 includes the exam questions/answers only and does not ASSH Disclosure Policy: As a provider accredited by the ACCME, the ASSH must ensure fi include access to the JHS articles referenced. balance, independence, objectivity, and scienti c rigor in all its activities. Disclosures for this Article Statement of Need: This CME activity was developed by the JHS review section editors and review article authors as a convenient education tool to help increase or affirm Editors reader’s knowledge. The overall goal of the activity is for participants to evaluate the Ghazi M. Rayan, MD, has no relevant conflicts of interest to disclose. appropriateness of clinical data and apply it to their practice and the provision of patient Authors care. -

Hand Surgery: a Guide for Medical Students
Hand Surgery: A Guide for Medical Students Trevor Carroll and Margaret Jain MD Table of Contents Trigger Finger 3 Carpal Tunnel Syndrome 13 Basal Joint Arthritis 23 Ganglion Cyst 36 Scaphoid Fracture 43 Cubital Tunnel Syndrome 54 Low Ulnar Nerve Injury 64 Trigger Finger (stenosing tenosynovitis) • Anatomy and Mechanism of Injury • Risk Factors • Symptoms • Physical Exam • Classification • Treatments Trigger Finger: Anatomy and MOI (Thompson and Netter, p191) • The flexor tendons run within the synovial tendinous sheath in the finger • During flexion, the tendons contract, running underneath the pulley system • Overtime, the flexor tendons and/or the A1 pulley can get inflamed during finger flexion. • Occassionally, the flexor tendons and/or the A1 pulley abnormally thicken. This decreases the normal space between these structures necessary for the tendon to smoothly glide • In more severe cases, patients can have their fingers momentarily or permanently locked in flexion usually at the PIP joint (Trigger Finger‐OrthoInfo ) Trigger Finger: Risk Factors • Age: 40‐60 • Female > Male • Repetitive tasks may be related – Computers, machinery • Gout • Rheumatoid arthritis • Diabetes (poor prognostic sign) • Carpal tunnel syndrome (often concurrently) Trigger Finger: Subjective • C/O focal distal palm pain • Pain can radiate proximally in the palm and distally in finger • C/O finger locking, clicking, sticking—often worse during sleep or in the early morning • Sometimes “snapping” during flexion • Can improve throughout the day Trigger Finger: