Best Practices from D.C. Hospitals and the Health Care Community
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sibley Memorial Hospital Johns Hopkins Medicine
Office of the President 5255 Loughboro Road, N.W. Washington, D.C. 200|6-2695 202-537-4680Telephone 202-537-4683 Fax SIBLEY MEMORIAL HOSPITAL JOHNS HOPKINS MEDICINE kwiktag ~ 090 761 843 October 22, 20:~2 Mr. Amha W. Selassie Director, State Health Planning and Development Agency District of Columbia Department of Health 825 North Capitol Street Washington, DC 20002 Re: Certificate of Need Registration Number :~2-3-10 Dear Mr. Selassie: Enclosed please find Sibley Memorial Hospital’s Certificate of Need (CON) application for the Establishment of Proton Therapy Service - CON 12-3-10. We believe that this facility and equipment are vital to our growth and ability to serve this community as we work to fully integrate our oncology services with Johns Hopkins Medicine. Also included with each of the three CONs is a red binder. Documents contained in these binders include items of a competitive nature and equipment detail which fall under non-disclosure agreements. We request these documents be kept out of the public record. We anticipate that this application will be reviewed in the November 2012 batch review of CON applications. We believe that the application is complete. However, if you or your staff need additional information, please contact Christine Stuppy, Vice President, Business Development and Strategic Planning at 202-537-4472. We look forward to working with you through this process. Sincerely, Richard O. Davis, Ph.D. President GOVERNMENT OF THE DISTRICT OF COLUMBIA Department of Health State Health Planning and Development Agency Certificate of Need Application Checklist Registration Number: As discussed and agreed, the fpllowing questions (as checked)are to be cor~;’~eted on the D.C. -
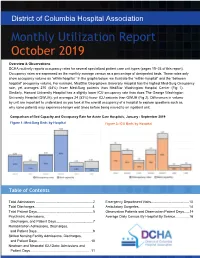
Monthly Utilization Report October 2019
District of Columbia Hospital Association Monthly Utilization Report October 2019 Overview & Observations DCHA routinely reports occupancy rates for several specialized patient care unit types (pages 15–23 of this report). Occupancy rates are expressed as the monthly average census as a percentage of designated beds. These rates only show occupancy volume as “within hospital.” In the graphs below, we illustrate the “within-hospital” and the “between hospital” occupancy volume. For example, MedStar Georgetown University Hospital has the highest Med-Surg Occupancy rate, yet averages 270 (54%) fewer Med-Surg patients than MedStar Washington Hospital Center (Fig 1). Similarly, Howard University Hospital has a slightly lower ICU occupancy rate than does The George Washington University Hospital (GWUH); yet averages 24 (53%) fewer ICU patients than GWUH (Fig 2). Differences in volume by unit are important to understand as you look at the overall occupancy of a hospital to explore questions such as, why some patients may experience longer wait times before being moved to an inpatient unit. Comparison of Bed Capacity and Occupancy Rate for Acute Care Hospitals, January - September 2019 Figure 1: Med-Surg Beds by Hospital Figure 2: ICU Beds by Hospital Table of Contents Total Admissions ............................................................2 Emergency Department Visits........................................13 Total Discharges.............................................................4 Ambulatory Surgeries.....................................................14 -

Capital Region Research (CAPRES)
Capital Region Research (CAPRES) ROLE OF OFFICE CAPRES is part of the Johns Hopkins Institute for Clinical and Translational Research, which is under the leadership of Dr. Daniel Ford, Vice Dean for Clinical Investigation. The Office of Capital Region Research is led by Dr. Mark Sulkowski, Associate Dean for CAPRES and Jackie Lobien, BSN, CCRP‐CP, Director of CAPRES. The Office of Capital Region Research was established: 1. To foster medical discovery within the Johns Hopkins Medicine (JHM) community in the Washington capital region including Sibley Memorial Hospital, Suburban Hospital, and Howard County General Hospital; 2. To nurture research collaborations within the Johns Hopkins University School of Medicine and the Johns Hopkins Health System. 3. Enhance the care and experience of patients by providing opportunities to participate in clinical research at or close to the Johns Hopkins facility in which they receive care. CAPRES provides a dynamic interface for researchers in the Capital Region with several key Johns Hopkins Medicine research entities including the Institutional Review Board (IRB), Office of Research Administration (ORA), and Johns Hopkins Clinical Research Network (JHCRN). At each of the CAPRES institutions, CAPRES serves as a central resource for all areas of research oversight and administration including IRB/compliance, contracting, study budgets, research training, recruitment, clinical operations, marketing and finance. CAPRES has been integral in working with ORA to coordinate agreements and budgets for community physicians in private practice to open research studies within the walls of the community hospitals. CAPRES is responsible for the Research Review Committees (RRC) at Sibley Memorial Hospital, Suburban Hospital, and Howard County General Hospital. -

Service Compassion
11x85_CBR-final_CBR 10/3/18 11:40 AM Page 1 service compassion The Johns Hopkins Health System care Community Benefit Report | FISCAL YEAR 2017 community 11x85_CBR-final_CBR 10/3/18 11:48 AM Page 2 Pennsylvania The Johns Hopkins Table of Contents Hospital Howard County Johns Hopkins 3 Introduction General Bayview Medical Hospital Center 4 Overview – The Johns Delaware Hopkins Health System Baltimore Suburban Hospital Sibley 6 The Johns Hopkins Hospital Memorial Hospital 8 Johns Hopkins Bayview Medical Center Chesapeake Washington D.C. Bay Virginia 10 Howard County General Hospital 12 Suburban Hospital 14 Sibley Memorial Hospital 16 Johns Hopkins All Children’s Hospital 18 Fiscal Year 2017 Community Not shown on map: Johns Hopkins All Children’s Benefit Activities Summary Hospital St. Petersburg, Florida The Johns Hopkins Health System Hospitals 2 11x85_CBR-final_CBR 10/3/18 11:40 AM Page 3 A Continuing Commitment to Our Community Johns Hopkins Medicine is committed to Sibley Memorial Hospital in Washington, At Johns Hopkins, we know that by improving the health and wellness of D.C., and Johns Hopkins All Children’s supporting community institutions – the residents in the neighborhoods we Hospital in St. Petersburg, Florida – we congregations, schools, nonprofit serve. We seek partners who share our have developed meaningful partnerships organizations, and neighborhood values and mission to empower and that enhance our ability to improve the centers – we reach those with the educate our patients, staff, neighbors, health and vitality of our neighbors and greatest needs. We are committed to and communities. As students, the communities we serve. strengthening connections through educators, physicians, and nurses, our increased dialogue and collaboration This report highlights a few of these continuing commitment to patient care to help strengthen our communities. -

Higher Education & Healthcare
WASHINGTON, DC HIGHER EDUCATION & HEALTHCARE Washington, DC’s universities and hospitals are one of the most vital components of its economy. The Educational & Health Services sector is responsible for 17% of DC’s total employment. Since 2010, this sector has grown more than 18%, compared to DC’s total employment growth rate of nearly 6% during the same time period. As both knowledge generators and exporters, the combined impact of DC’s universities creates one of the largest economic DC UNIVERSITIES ARE RANKED IN THE TOP 100 engines in the region. The economic impact of these major DC BY U.S. NEWS & WORLD REPORT: GEORGETOWN universities approaches billion. UNIVERSITY (#21), THE GEORGE WASHINGTON UNIVERSITY (#57), AND AMERICAN UNIVERSITY (#72)4 During the academic year, nearly , students attend 3 college at a Washington, DC college or university. With enrollment and competition increasing, colleges and universities have built more than . million square feet of new DC EDUCATIONAL & HEALTH SERVICES EMPLOYMENT3 dorms and academic centers in DC since , with another . million square feet under construction. 10.5% Colleges, 36.3% Universities, and With major hospitals and numerous expansion plans, DC has Professional Schools experienced a major increase in health care employment. The 6.6% Health Care & Social Assistance sector has experienced an Other educational services increase in employment of from – and is 127,400 Ambulatory Health responsible for nearly percent of all DC employment. (2014 employment) Care Services Employment is expected to continue to grow as several hospitals are undergoing major expansion plans, including Hospitals 22.3% MedStar Georgetown University Hospital’s plan to build a new Nursing and Residential million medical and surgical pavilion. -

Johns Hopkins Medicine Finance Financial Assistance Policies Manual General
Version 8.0 Johns Hopkins Medicine Finance Policy Number PFS035 Financial Assistance Policies Manual Effective Date 10/01/2020 General Approval Date N/A Subject Page 1 of 10 Financial Assistance Supersedes Date 02/01/2020 This document applies to the following Participating Organizations: Howard County General Hospital Johns Hopkins Bayview Medical Center Johns Hopkins Community Physicians Johns Hopkins Surgery Centers Series Johns Hopkins University School of Sibley Memorial Hospital Suburban Hospital The Johns Hopkins Hospital Medicine Keywords: assistance, bill, debt, financial, medical Table of Contents Page Number I. PURPOSE 1 II. POLICY 1 III. PROCEDURES 2 IV. DEFINITIONS 7 V. REFERENCE 9 VI. SPONSOR 9 VII. REVIEW CYCLE 10 VIII. APPROVAL 10 Appendix A: SIBLEY MEMORIAL HOSPITAL (ONLY) FINANCIAL ASSISTANCE PROVISIONS Click Here SPECIFIC TO DC REGULATIONS Appendix B: Financial Assistance Application Click Here I. PURPOSE Johns Hopkins Medicine is committed to providing Financial Assistance to patients who have health care needs and are uninsured, underinsured, ineligible for a government program, or otherwise unable to pay, for Medically Necessary Care based on their individual financial situation. II. POLICY This policy contains the criteria to be used in determining a patient’s eligibility for Financial Assistance and outlines the process and guidelines that shall be used to determine eligibility for Financial Assistance and the completion of the Financial Assistance application process. This policy governs the provision of Financial Assistance for patients who are uninsured, underinsured, ineligible for a government program, or otherwise unable to pay for Medically Necessary Care based on their individual financial situation. Sibley Memorial Hospital is located in the District of Columbia. -

Utilization Indicators Calendar Year 2019
District of Columbia Hospital Association Utilization Indicators Calendar Year 2019 About This Report The charts and tables in this publication are intended to provide aggregate and comparative data on health care facility utilization in the District of Columbia. The source of the data is the District of Columbia Hospital Association’s Monthly Utilization Survey (self-reported by individual facilities). ISSUED | May | 2020 | www.dcha.org District of Columbia Hospital Association 1152 15th Street NW | Suite 900 Washington, D.C. | 20005 dcha.org AMBULATORY SURGERIES 2018 2019 % Change ACUTE TOTAL Children’s National Health System 12,614 13,151 4.3% The George Washington University Hospital 16,280 17,030 4.6% Howard University Hospital 7,386 9,324 26.2% MedStar Georgetown University Hospital 8,071 8,273 2.5% MedStar Washington Hospital Center 10,583 10,631 0.5% Providence Hospital – Ascension 5,586 - -100.0% Sibley Memorial Hospital – Johns Hopkins Medicine 8,657 9,010 4.1% United Medical Center 1,231 1,311 6.5% GRAND TOTAL 70,408 68,730 -2.4% AMBULATORY SURGERIES 72,000 71,353 70,408 70,000 69,941 69,126 69,792 68,823 68,380 68,730 68,000 67,034 66,000 65,103 64,000 62,000 60,000 58,000 56,000 ► YEAR 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 Note: Calculations are based on reported utilization figures for the District of Columbia acute non-federal hospitals. UTILIZATION INDICATORS / PAGE 2 EMERGENCY DEPARTMENT VISITS 2018 2019 % Change There was a statistically ACUTE TOTAL significant decrease in ED visits in 2019. -

Information on Health Care Costs
United States General Accounting Office GAO Report to Congressional Requesters April 1996 DISTRICT OF COLUMBIA Information on Health Care Costs GOA years 1921 - 1996 GAO/AIMD-96-42 United States General Accounting Office GAO Washington, D.C. 20548 Accounting and Information Management Division B-265725 April 22, 1996 The Honorable James T. Walsh Chairman The Honorable Julian C. Dixon Ranking Minority Member The Honorable Rodney P. Frelinghuysen Member Subcommittee on the District of Columbia Committee on Appropriations House of Representatives At your request, we are providing baseline information on the District of Columbia’s health care system to help evaluate the various restructuring proposals the District is considering in light of consistently rising health care expenditures, limited resources, and pending legislative changes. Specifically, you asked us to answer questions concerning the District’s health care budget and the composition of the District’s health care system such as the number of Medicaid recipients and uninsured and distribution of hospitals and clinics. To respond to your questions, we looked at many aspects of health care in the District. In doing so, we also identified several additional issues that we thought would benefit your deliberations. This letter and the accompanying appendixes discuss those issues as well as respond to your specific questions. Recent studies1 on the District’s health care system have concluded that the District’s health care problems are aggravated by social factors, such as high rates of poverty, crime, substance abuse, and unemployment in the city. Such factors, these studies found, in turn contribute to (1) a certain segment of the population that does not seek or obtain preventive health care and is unable to pay for its health care, (2) the inappropriate use of D.C. -

Monday, January 25, 2021 WHERE WE ARE TODAY 2
Monday, January 25, 2021 WHERE WE ARE TODAY 2 January 25, 2021 VACCINE DISTRIBUTION 3 Total doses already Total doses Additional doses delivered already becoming available (as of 1/23/21): administered: this week: 68,750 51,421 9,475 January 25, 2021 VACCINE DISTRIBUTION 4 This week, DC is receiving 8,775 doses of the Pfizer vaccine and 5,600 doses of the Moderna vaccine. Moderna doses breakdown: § 2,975 doses for appointments that were made available through the portal last week § 1,500 doses for appointments that were previously booked § 300 doses to a pharmacy to vaccinate residents of Intermediate Care Facilities § 100 doses to a pharmacy to vaccinate residents of community residential facilities/group homes § 400 doses to Unity Healthcare to vaccinate individuals experiencing homelessness and patients at Unity § 200 doses to United Medical Center for patients that will be booked directly through UMC § 125 doses for pharmacy or provider staff, or to be allocated in the following week’s schedule Pfizer doses breakdown: § 3,900 doses to Children’s for DCPS in-person staff § 1,950 doses to One Medical for public charter school in-person staff § 1,950 doses to Kaiser for MPD and their eligible patients § 975 doses to Sibley/Johns Hopkins for the Senior Housing-DCHA initiative and their patients January 25, 2021 OUTREACH FROM HOSPITALS AND MEDICAL PROVIDERS 5 District hospitals and medical providers have started outreach to schedule their patient population of DC residents 65 years and older. Like the District’s COVID-19 vaccination scheduling portal, hospital appointments are limited. -
The Changing Hospital Sector in Washington, D.C.: Implications for the Poor
THE CHANGING HOSPITAL SECTOR IN Implications for the Poor BARBARA A. ORMOND AND RANDALL R. BOVBJERG The Changing Hospital Sector in Washington, D.C.: Implications for the Poor Barbara A. Ormond Randall R. Bovbjerg THE URBAN INSTITUTE Copyright ©1998. The Urban Institute. All rights reserved. Except for short quotes, no part of this book may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by information storage or retrieval system, without written permission from the Urban Institute Press. Acknowledgments Support for this paper was provided by the Robert Wood Johnson Foundation. The views expressed are those of the authors and should not be attributed to the Urban Institute, its trustees, or its funders. The authors gratefully acknowledge Peggy Sulvetta and John Holahan, who initiated the project and supported it in all phases. We would also like to thank Judith Feder, Joan Lewis, and Virginia Fleming for their helpful guidance and useful comments; Susan Wallin for her timely contributions to the research; Chris Hayes, Brian Bruen, and Suresh Rangarajan for assistance in mapping; Niall Brennan for data analysis; and Matthew Schirmer for research assistance. The research could not have been accomplished without the cooperation of Washington hospital officials, community providers, and health care observers too numerous to mention, and we greatly appreciate their having taken the time to meet with us. Contents Executive Summary . .1 Introduction . .5 Context . .7 Socioeconomic and Demographic Characteristics . .7 Health Status . .7 Health Insurance and Supply of Providers . .9 The Hospitals . .10 Hospital-Specific Utilization . .12 Payer Mix . -

Health & Wellness
WASHINGTON, DC HEALTH & WELLNESS DC is a national center for patient care and medical research, with 16 medical centers and hospitals located within the District. These institutions help make the metro area as a whole a national hub for biomedical research. DC organizations received over $225 million from the National Institutes of Health in 2017, 1 and the District is also home to major federal agencies such as the Department of Health and Human Services (DHHS) and the Food and Drug Administration (FDA). This proximity is critical to organizations and companies striving to influence healthcare policy. In addition, recent policy and technological innovations have helped grow a new health innovation industry. Demand for healthcare data analytics is growing rapidly as electronic health records are increasingly used and advances are made in precision medicine (market expected to top $141 billion by 2026).2 WHY HEALTH COMPANIES CHOOSE DC RESOURCES FOR HEALTH & WELLNESS COMPANIES • Customer base: The concentration of medical centers, hospitals and health research institutions, in addition to a • DC BizCAP programs (Dept. of Insurance, Securities fitness-conscious population, offers business opportunities to and Banking) DC health companies. • Qualified High Technology Company tax incentives • Workforce: DC’s three medical schools and many training (Office of Tax and Revenue) programs for nurses, caregivers, and other specialties provide a steady stream of local talent. DC’s workforce is • Creative and Open Space Modernization tax rebate also tech-savvy with deep legal and data expertise—skills (Office of the Deputy Mayor for Planning and sought by many biotech and health technology companies. Economic Development) • Entrepreneurship: DC is home to many incubators and • Work Opportunity Tax Credit, On the Job Training, co-working spaces that support entrepreneurs, such as and Apprenticeship hiring programs (Dept. -
Utilization Indicators Calendar Year 2010
Utilization Indicators Calendar Year 2010 Issued March 2011 ABOUT THIS REPORT ON UTILIZATION INDICATORS The charts in this publication are intended to provide aggregate and comparative data on the utilization trends of the District of Columbia hospital community for calendar year 2010. The source of the data is the District of Columbia Hospital Association’s (DCHA) Monthly Utilization Survey and Quarterly Bed Capacity and Census Survey (self-reported by individual hospitals). The graphs in this report describe utilization trends in the aggregate for the following District acute care non-federal hospitals: • Children’s National Medical Center • Georgetown University Hospital • Sibley Memorial Hospital • George Washington University • Howard University Hospital • United Medical Center Hospital • Providence Hospital • Washington Hospital Center Operating Bed Capacity 4th 4th Quarter Quarter Five Year Trend: 2006-2010 2006 2010 % Change Acute Care 2,780 2,714 2,766 2,724 Children’s National Medical Center 230 255 10.9% 2,734 George Washington University Hospital 339 341 0.6% Georgetown University Hospital 402 402 0.0% Howard University Hospital 218 291 33.5% Beds Operating Providence Hospital 291 272 -6.5% Sibley Memorial Hospital 264 205 -22.3% United Medical Center 228 184 -19.3% 0 1,000 2,000 3,000 4,000 Washington Hospital Center 808 774 -4.2% 4th Qtr 06 4th Qtr 07 4th Qtr 08 4th Qtr 09 4th Qtr 10 ACUTE TOTAL 2,780 2,724 -2.0% Period Covered Other Specialty National Rehabilitation Hospital 137 187 36.5% Compared to last year, there has been a slight decrease of 42 operating beds, approximately 1.5 Psychiatric Institute of Washington 104 104 0.0% percent, in the District’s acute care non-federal SHW - Capitol Hill 60 60 0.0% hospitals.