How to Administer Intramuscular and Subcutaneous Vaccine Injections Administration by the Intramuscular (IM) Route
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Intravenous Therapy Procedure Manual
INTRAVENOUS THERAPY PROCEDURE MANUAL - 1 - LETTER OF ACCEPTANCE __________________________________________ hereby approves (Facility) the attached Reference Manual as of _____________________. (Date) The Intravenous Therapy Procedure Manual will be reviewed at least annually or more often when deemed appropriate. Revisions will be reviewed as they occur. Current copies of the Intravenous Therapy Procedure Manual shall be maintained at each appropriate nursing station. I have reviewed this manual and agree to its approval. __________________________ (Administrator) __________________________ (Director of Nursing) __________________________ (Medical Director) - 2 - TABLE OF CONTENTS TABLE OF CONTENTS INTRODUCTION A. Purpose 1 B. Local Standard of Practice 1 RESPONSIBILITIES A. Responsibilities: M Chest Pharmacy 1 B. Responsibilities: Administrator 1 C. Responsibilities: Director of Nursing Services (DON/DNS) 1 D. Skills Validation 2 AMENDMENTS GUIDELINES A. Resident Candidacy for IV Therapy 1 B. Excluded IV Medications and Therapies 1 C. Processing the IV Order 1 D. IV Solutions/Medications: Storage 2 E. IV Solutions/Medications: Handling 3 F. IV Solutions and Supplies: Destroying and Returning 4 G. IV Tubing 5 H. Peripheral IV Catheters and Needles 6 I. Central Venous Devices 7 J. Documentation and Monitoring 8 K. IV Medication Administration Times 9 L. Emergency IV Supplies 10 I TABLE OF CONTENTS PROTOCOLS A. IV Antibiotic 1 1. Purpose 2. Guidelines 3. Nursing Responsibilities B. IV Push 2 1. Purpose 2. Guidelines C. Anaphylaxis Allergic Reaction 4 1. Purpose 2. Guidelines 3. Nursing Responsibilities and Interventions 4. Signs and Symptoms of Anaphylaxis 5. Drugs Used to Treat Anaphylaxis 6. Physician Protocol PRACTICE GUIDELINES A. Purpose 1 B. Personnel 1 C. Competencies 1 D. -

Injection Technique 1: Administering Drugs Via the Intramuscular Route
Copyright EMAP Publishing 2018 This article is not for distribution except for journal club use Clinical Practice Keywords Intramuscular injection/ Medicine administration/Absorption Practical procedures This article has been Injection technique double-blind peer reviewed Injection technique 1: administering drugs via the intramuscular route rugs administered by the intra- concerns that nurses are still performing Author Eileen Shepherd is clinical editor muscular (IM) route are depos- outdated and ritualistic practice relating to at Nursing Times. ited into vascular muscle site selection, aspirating back on the syringe Dtissue, which allows for rapid (Greenway, 2014) and skin cleansing. Abstract The intramuscular route allows absorption into the circulation (Dough- for rapid absorption of drugs into the erty and Lister, 2015; Ogston-Tuck, 2014). Site selection circulation. Using the correct injection Complications of poorly performed IM Four muscle sites are recommended for IM technique and selecting the correct site injection include: administration: will minimise the risk of complications. l Pain – strategies to reduce this are l Vastus lateris; outlined in Box 1; l Rectus femoris Citation Shepherd E (2018) Injection l Bleeding; l Deltoid; technique 1: administering drugs via l Abscess formation; l Ventrogluteal (Fig 1, Table 1). the intramuscular route. Nursing Times l Cellulitis; Traditionally the dorsogluteal (DG) [online]; 114: 8, 23-25. l Muscle fibrosis; muscle was used for IM injections but this l Injuries to nerves and blood vessels muscle is in close proximity to a major (Small, 2004); blood vessel and nerves, with sciatic nerve l Inadvertent intravenous (IV) access. injury a recognised complication (Small, These complications can be avoided if 2004). -

Clinical Update and Treatment of Lactation Insufficiency
Review Article Maternal Health CLINICAL UPDATE AND TREATMENT OF LACTATION INSUFFICIENCY ARSHIYA SULTANA* KHALEEQ UR RAHMAN** MANJULA S MS*** SUMMARY: Lactation is beneficial to mother’s health as well as provides specific nourishments, growth, and development to the baby. Hence, it is a nature’s precious gift for the infant; however, lactation insufficiency is one of the explanations mentioned most often by women throughout the world for the early discontinuation of breast- feeding and/or for the introduction of supplementary bottles. Globally, lactation insufficiency is a public health concern, as the use of breast milk substitutes increases the risk of morbidity and mortality among infants in developing countries, and these supplements are the most common cause of malnutrition. The incidence has been estimated to range from 23% to 63% during the first 4 months after delivery. The present article provides a literary search in English language of incidence, etiopathogensis, pathophysiology, clinical features, diagnosis, and current update on treatment of lactation insufficiency from different sources such as reference books, Medline, Pubmed, other Web sites, etc. Non-breast-fed infant are 14 times more likely to die due to diarrhea, 3 times more likely to die of respiratory infection, and twice as likely to die of other infections than an exclusively breast-fed child. Therefore, lactation insufficiency should be tackled in appropriate manner. Key words : Lactation insufficiency, lactation, galactagogue, breast-feeding INTRODUCTION Breast-feeding is advised becasue human milk is The synonyms of lactation insufficiency are as follows: species-specific nourishment for the baby, produces lactational inadequacy (1), breast milk insufficiency (2), optimum growth and development, and provides substantial lactation failure (3,4), mothers milk insufficiency (MMI) (2), protection from illness. -

SIDS and Other Sleep-Related Infant Deaths: Expansion of Recommendations for a Safe Infant Sleeping Environment
Organizational Principles to Guide and Define the Child Health Care System and/or Improve the Health of all Children POLICY STATEMENT SIDS and Other Sleep-Related Infant Deaths: Expansion of Recommendations for a Safe Infant Sleeping Environment TASK FORCE ON SUDDEN INFANT DEATH SYNDROME abstract KEY WORDS Despite a major decrease in the incidence of sudden infant death syn- SIDS, sudden infant death, infant mortality, sleep position, bed- sharing, tobacco, pacifier, immunization, bedding, sleep surface drome (SIDS) since the American Academy of Pediatrics (AAP) released ABBREVIATIONS its recommendation in 1992 that infants be placed for sleep in a non- SIDS—sudden infant death syndrome prone position, this decline has plateaued in recent years. Concur- SUID—sudden unexpected infant death rently, other causes of sudden unexpected infant death that occur AAP—American Academy of Pediatrics during sleep (sleep-related deaths), including suffocation, asphyxia, This document is copyrighted and is property of the American and entrapment, and ill-defined or unspecified causes of death have Academy of Pediatrics and its Board of Directors. All authors have filed conflict of interest statements with the American increased in incidence, particularly since the AAP published its last Academy of Pediatrics. Any conflicts have been resolved through statement on SIDS in 2005. It has become increasingly important to a process approved by the Board of Directors. The American address these other causes of sleep-related infant death. Many of the Academy of Pediatrics has neither solicited nor accepted any commercial involvement in the development of the content of modifiable and nonmodifiable risk factors for SIDS and suffocation are this publication. -

Definitions of Child Abuse and Neglect
STATE STATUTES Current Through March 2019 WHAT’S INSIDE Defining child abuse or Definitions of Child neglect in State law Abuse and Neglect Standards for reporting Child abuse and neglect are defined by Federal Persons responsible for the child and State laws. At the State level, child abuse and neglect may be defined in both civil and criminal Exceptions statutes. This publication presents civil definitions that determine the grounds for intervention by Summaries of State laws State child protective agencies.1 At the Federal level, the Child Abuse Prevention and Treatment To find statute information for a Act (CAPTA) has defined child abuse and neglect particular State, as "any recent act or failure to act on the part go to of a parent or caregiver that results in death, https://www.childwelfare. serious physical or emotional harm, sexual abuse, gov/topics/systemwide/ or exploitation, or an act or failure to act that laws-policies/state/. presents an imminent risk of serious harm."2 1 States also may define child abuse and neglect in criminal statutes. These definitions provide the grounds for the arrest and prosecution of the offenders. 2 CAPTA Reauthorization Act of 2010 (P.L. 111-320), 42 U.S.C. § 5101, Note (§ 3). Children’s Bureau/ACYF/ACF/HHS 800.394.3366 | Email: [email protected] | https://www.childwelfare.gov Definitions of Child Abuse and Neglect https://www.childwelfare.gov CAPTA defines sexual abuse as follows: and neglect in statute.5 States recognize the different types of abuse in their definitions, including physical abuse, The employment, use, persuasion, inducement, neglect, sexual abuse, and emotional abuse. -

Overcoming Breastfeeding Concerns- Part 2
9/21/2018 OVERCOMING BREASTFEEDING Presented by: CONCERNS- PART 2 Kary Johnson, IBCLC OVERVIEW • Pacifiers • Pumping • Low Milk Supply • Feeding Multiples • Supplementation • Discharge Guidelines PICTURE FROM HTTPS://WWW.ETSY.COM/LISTING/464346270/BREAST-ENCOURAGEMENT-CARD-BREASTFEEDING 1 9/21/2018 PACIFIERS Step 9: Counsel mothers on the use and risks of feeding bottles, teats and pacifiers. What does the AAP say? •NG/Gavage •“Mothers of healthy term infants should be instructed to use pacifiers at •Hypoglycemia infant nap or sleep time after breastfeeding is well established, at Infant approximately 3 go 4 weeks of age.” •Lab draws • “Pacifier use should be limited to specific medical situations. These include Pain •Circumcision uses for pain relief, as a calming agent, or as part of a structured program •Illness for enhancing oral motor function.” •Medications Maternal •PMAD • NICU: to organize suck, swallow, breathe pattern of premature infant (in addition to reasons above) (AAP, 2012) PACIFIERS Ask yourself…what is the reason for use? Management: • All effort should be made to prevent separation of mom & baby (i.e. newborn nursery) • Avoid overuse • Be careful to not incorrectly pacify infant hunger • Non-nutritive sucking on mother’s breast is a great alternative Overuse or misuse results in: • Decreased breastfeeding duration • Reduced milk supply • Dental issues, difficulty weaning, and use well into childhood 2 9/21/2018 BREAST PUMPING Reasons a mother may need to pump: • Nipple trauma • Low milk supply • Late preterm infants -

22428 Moxifloxacin Statisical PREA
U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research Office of Translational Science Office of Biostatistics S TATISTICAL R EVIEW AND E VALUATION CLINICAL STUDIES NDA/Serial Number: 22,428 Drug Name: Moxifloxacin AF (moxifloxacin hydrochloride ophthalmic solution) 0.5% Indication(s): Treatment of bacterial conjunctivitis Applicant: Alcon Pharmaceuticals, Ltd. Date(s): Letter date:21 May 2010; Filing date: 18 June, 2010; PDUFA goal date: 19 November 2010 Review Priority: Priority Biometrics Division: Anti-infective and Ophthalmology Products Statistical Reviewer: Mark. A. Gamalo, Ph.D. Concurring Reviewers: Yan Wang, Ph.D. Medical Division: Anti-infective and Ophthalmology Products Clinical Reviewer: Lucious Lim, M.D. Project Manager: Lori Gorski Keywords: superiority, Moxifloxacin hydrochloride ophthalmic solution, bacterial conjunctivitis, bulbar conjunctival injection, conjunctival discharge/exudate TABLE OF CONTENTS TABLE OF CONTENTS................................................................................................................ 2 LIST OF TABLES.......................................................................................................................... 3 1. EXECUTIVE SUMMARY ...................................................................................................... 4 1. 1 Conclusions and Recommendations..................................................................................... 4 1. 2 Brief Overview of Clinical Studies ..................................................................................... -
Informed Consent for Medication, Zyprexa
DEPARTMENT OF HEALTH SERVICES STATE OF WISCONSIN Division of Care and Treatment Services 42 CFR483.420(a)(2) F-24277 (09/2016) DHS 134.31(3)(o) DHS 94.03 & 94.09 §§ 51.61(1)(g) & (h) INFORMED CONSENT FOR MEDICATION Dosage and / or Side Effect information last revised on 04/16/2021 Completion of this form is voluntary. If not completed, the medication cannot be administered without a court order unless in an emergency. This consent is maintained in the client’s record and is accessible to authorized users. Name – Patient / Client (Last, First MI) ID Number Living Unit Date of Birth , Name – Individual Preparing This Form Name – Staff Contact Name / Telephone Number – Institution ANTICIPATED RECOMMENDED MEDICATION CATEGORY MEDICATION DOSAGE DAILY TOTAL DOSAGE RANGE RANGE Antipsychotic / Bipolar Agent Zyprexa oral tablet; Oral: 2.5 mg-50 mg with most doses in Zyprexa Zydis oral the 2.5 mg-20 mg range disintegrating tablet; IM: 5 mg-10 mg per dose, up to 3 doses Zyprexa Intramuscular 24 hours Injection; Long Acting Injectable: 150 mg-300 mg Zyprexa Relprevv IM every 2 weeks, Intramuscluar Injection 300 mg-405 mg IM every 4 weeks (olanzapine) The anticipated dosage range is to be individualized, may be above or below the recommended range but no medication will be administered without your informed and written consent. Recommended daily total dosage range of manufacturer, as stated in Physician’s Desk Reference (PDR) or another standard reference. This medication will be administered Orally Injection Other – Specify: 1. Reason for Use of Psychotropic Medication and Benefits Expected (note if this is ‘Off-Label’ Use) Include DSM-5 diagnosis or the diagnostic “working hypothesis.” 2. -

Pediatric Respiratory Rates Age Rate (Breaths Per Minute)
Pediatric Respiratory Rates Age Rate (breaths per minute) Infant (birth–1 year) 30–60 Toddler (1–3 years) 24–40 Preschooler (3–6 years) 22–34 School-age (6–12 years) 18–30 Adolescent (12–18 years) 12–16 Pediatric Pulse Rates Age Low High Infant (birth–1 year) 100 160 Toddler (1–3 years) 90 150 Preschooler (3–6 years) 80 140 School-age (6–12 years) 70 120 Adolescent (12–18 years) 60 100 Pulse rates for a child who is sleeping may be 10 percent lower than the low rate listed. Low-Normal Pediatric Systolic Blood Pressure Age* Low Normal Infant (birth–1 year) greater than 60* Toddler (1–3 years) greater than 70* Preschooler (3–6 years) greater than 75 School-age (6–12 years) greater than 80 Adolescent (12–18 years) greater than 90 *Note: In infants and children aged three years or younger, the presence of a strong central pulse should be substituted for a blood pressure reading. Pediatric CUPS Assessment Category Assessment Actions Example Critical Absent airway, Perform rapid initial Severe traumatic injury breathing, or interventions and transport with respiratory arrest or circulation simultaneously cardiac arrest Unstable Compromised airway, Perform rapid initial Significant injury with breathing, or interventions and transport respiratory distress, circulation with simultaneously active bleeding, shock; altered mental status near-drowning; unresponsiveness Potentially Normal airway, Perform initial assessment Minor fractures; unstable breathing, circulation, with interventions; transport pedestrian struck by car and mental status BUT -

Product Monograph
PRODUCT MONOGRAPH Pr SANDOZ ONDANSETRON ODT Ondansetron Orally Disintegrating Tablets 4 mg and 8 mg ondansetron Manufacturer Standard Pr SANDOZ ONDANSETRON Ondansetron Tablets 4 mg and 8 mg ondansetron (as ondansetron hydrochloride dihydrate) Manufacturer Standard PrONDANSETRON INJECTION USP (ondansetron hydrochloride dihydrate) 2 mg/mL PrONDANSETRON HYDROCHLORIDE DIHYDRATE INJECTION Ondansetron Injection Manufacturer Standard 2 mg/mL Ondansetron (as ondansetron hydrochloride dihydrate) for injection Antiemetic (5-HT3-receptor antagonist) Sandoz Canada Inc. Date of Preparation: 145 Jules-Léger September 26, 2016 Boucherville, Québec, Canada J4B 7K8 Control No.: 198381 Ondansetron by Sandoz Page 1 of 43 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION .......................................................... 3 SUMMARY PRODUCT INFORMATION ................................................................................. 3 INDICATIONS AND CLINICAL USE ....................................................................................... 4 CONTRAINDICATIONS ............................................................................................................ 4 WARNINGS AND PRECAUTIONS .......................................................................................... 5 ADVERSE REACTIONS ............................................................................................................ 7 DRUG INTERACTIONS ............................................................................................................ -
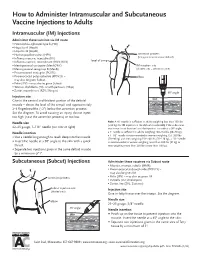
How to Administer Intramuscular and Subcutaneous Vaccines to Adults
How to Administer Intramuscular and Subcutaneous Vaccine Injections to Adults Intramuscular (IM) Injections Administer these vaccines via IM route • Haemophilus influenzae type b (Hib) • Hepatitis A (HepA) • Hepatitis B (HepB) • Human papillomavirus (HPV) acromion process (bony prominence above deltoid) • Influenza vaccine, injectable (IIV) • level of armpit • Influenza vaccine, recombinant (RIV3; RIV4) • Meningococcal conjugate (MenACWY) IM injection site • Meningococcal serogroup B (MenB) (shaded area = deltoid muscle) • Pneumococcal conjugate (PCV13) • Pneumococcal polysaccharide (PPSV23) – elbow may also be given Subcut • Polio (IPV) – may also be given Subcut • Tetanus, diphtheria (Td), or with pertussis (Tdap) • Zoster, recombinant (RZV; Shingrix) 90° angle Injection site skin Give in the central and thickest portion of the deltoid muscle – above the level of the armpit and approximately subcutaneous tissue 2–3 fingerbreadths (~2") below the acromion process. See the diagram. To avoid causing an injury, do not inject muscle too high (near the acromion process) or too low. Needle size Note: A ⅝" needle is sufficient in adults weighing less than 130 lbs (<60 kg) for IM injection in the deltoid muscle only if the subcutane- 22–25 gauge, 1–1½" needle (see note at right) ous tissue is not bunched and the injection is made at a 90° angle; Needle insertion a 1" needle is sufficient in adults weighing 130–152 lbs (60–70 kg); a 1–1½" needle is recommended in women weighing 153–200 lbs • Use a needle long enough to reach deep into the muscle. (70–90 kg) and men weighing 153–260 lbs (70–118 kg); a 1½" needle • Insert the needle at a 90° angle to the skin with a quick is recommended in women weighing more than 200 lbs (91 kg) or thrust.