Infusion/Injection Coding Education Injection/Infusion Hierarchy for Facility Reporting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Study Protocol and Statistical Analysis Plan
The University of Texas Southwestern Medical Center at Dallas Institutional Review Board PROJECT SUMMARY Study Title: Ultrasound-guided fascia iliaca compartment block versus periarticular infiltration for pain management after total hip arthroplasty: a randomized controlled trial Principal Investigator: Irina Gasanova, MD Sponsor/Funding Source: Department of Anesthesiology and Pain Management, UT Southwestern Medical School IRB Number: STU 122015-022 NCT Number: NCT02658240 Date of Document: 01 April 2016 Page 1 of 7 Purpose: In this randomized, controlled, observer-blinded study we plan to evaluate ultrasound-guided fascia iliaca compartment block with ropivacaine and periarticular infiltration with ropivacaine for postoperative pain management after total hip arthroplasty (THA). Background: Despite substantial advances in our understanding of the pathophysiology of pain and availability of newer analgesic techniques, postoperative pain is not always effectively treated (1). Optimal pain management technique balances pain relief with concerns about safety and adverse effects associated with analgesic techniques. Currently, postoperative pain is commonly treated with systemic opioids, which are associated with numerous adverse effects including nausea and vomiting, dizziness, drowsiness, pruritus, urinary retention, and respiratory depression (2). Use of regional and local anesthesia has been shown to reduce opioid requirements and opioid-related side effects. Therefore, their use has been emphasized (3, 4, 5, 6). Fascia Iliaca compartment block (FICB) is a field block that blocks the nerves from the lumbar plexus supplying the thigh (i.e., lateral femoral cutaneous femoral and obturator nerves). The obturator nerve is sometimes involved in the FICB but probably plays little role in postoperative pain relief for most surgeries of the hip and proximal femur. -

Intravenous Therapy Procedure Manual
INTRAVENOUS THERAPY PROCEDURE MANUAL - 1 - LETTER OF ACCEPTANCE __________________________________________ hereby approves (Facility) the attached Reference Manual as of _____________________. (Date) The Intravenous Therapy Procedure Manual will be reviewed at least annually or more often when deemed appropriate. Revisions will be reviewed as they occur. Current copies of the Intravenous Therapy Procedure Manual shall be maintained at each appropriate nursing station. I have reviewed this manual and agree to its approval. __________________________ (Administrator) __________________________ (Director of Nursing) __________________________ (Medical Director) - 2 - TABLE OF CONTENTS TABLE OF CONTENTS INTRODUCTION A. Purpose 1 B. Local Standard of Practice 1 RESPONSIBILITIES A. Responsibilities: M Chest Pharmacy 1 B. Responsibilities: Administrator 1 C. Responsibilities: Director of Nursing Services (DON/DNS) 1 D. Skills Validation 2 AMENDMENTS GUIDELINES A. Resident Candidacy for IV Therapy 1 B. Excluded IV Medications and Therapies 1 C. Processing the IV Order 1 D. IV Solutions/Medications: Storage 2 E. IV Solutions/Medications: Handling 3 F. IV Solutions and Supplies: Destroying and Returning 4 G. IV Tubing 5 H. Peripheral IV Catheters and Needles 6 I. Central Venous Devices 7 J. Documentation and Monitoring 8 K. IV Medication Administration Times 9 L. Emergency IV Supplies 10 I TABLE OF CONTENTS PROTOCOLS A. IV Antibiotic 1 1. Purpose 2. Guidelines 3. Nursing Responsibilities B. IV Push 2 1. Purpose 2. Guidelines C. Anaphylaxis Allergic Reaction 4 1. Purpose 2. Guidelines 3. Nursing Responsibilities and Interventions 4. Signs and Symptoms of Anaphylaxis 5. Drugs Used to Treat Anaphylaxis 6. Physician Protocol PRACTICE GUIDELINES A. Purpose 1 B. Personnel 1 C. Competencies 1 D. -

Injection Technique 1: Administering Drugs Via the Intramuscular Route
Copyright EMAP Publishing 2018 This article is not for distribution except for journal club use Clinical Practice Keywords Intramuscular injection/ Medicine administration/Absorption Practical procedures This article has been Injection technique double-blind peer reviewed Injection technique 1: administering drugs via the intramuscular route rugs administered by the intra- concerns that nurses are still performing Author Eileen Shepherd is clinical editor muscular (IM) route are depos- outdated and ritualistic practice relating to at Nursing Times. ited into vascular muscle site selection, aspirating back on the syringe Dtissue, which allows for rapid (Greenway, 2014) and skin cleansing. Abstract The intramuscular route allows absorption into the circulation (Dough- for rapid absorption of drugs into the erty and Lister, 2015; Ogston-Tuck, 2014). Site selection circulation. Using the correct injection Complications of poorly performed IM Four muscle sites are recommended for IM technique and selecting the correct site injection include: administration: will minimise the risk of complications. l Pain – strategies to reduce this are l Vastus lateris; outlined in Box 1; l Rectus femoris Citation Shepherd E (2018) Injection l Bleeding; l Deltoid; technique 1: administering drugs via l Abscess formation; l Ventrogluteal (Fig 1, Table 1). the intramuscular route. Nursing Times l Cellulitis; Traditionally the dorsogluteal (DG) [online]; 114: 8, 23-25. l Muscle fibrosis; muscle was used for IM injections but this l Injuries to nerves and blood vessels muscle is in close proximity to a major (Small, 2004); blood vessel and nerves, with sciatic nerve l Inadvertent intravenous (IV) access. injury a recognised complication (Small, These complications can be avoided if 2004). -

An Overview On: Sublingual Route for Systemic Drug Delivery
International Journal of Research in Pharmaceutical and Biomedical Sciences ISSN: 2229-3701 __________________________________________Review Article An Overview on: Sublingual Route for Systemic Drug Delivery K. Patel Nibha1 and SS. Pancholi2* 1Department of Pharmaceutics, BITS Institute of Pharmacy, Gujarat Technological university, Varnama, Vadodara, Gujarat, India 2BITS Institute of Pharmacy, Gujarat Technological University, Varnama, Vadodara, Gujarat, India. __________________________________________________________________________________ ABSTRACT Oral mucosal drug delivery is an alternative and promising method of systemic drug delivery which offers several advantages. Sublingual literally meaning is ''under the tongue'', administrating substance via mouth in such a way that the substance is rapidly absorbed via blood vessels under tongue. Sublingual route offers advantages such as bypasses hepatic first pass metabolic process which gives better bioavailability, rapid onset of action, patient compliance , self-medicated. Dysphagia (difficulty in swallowing) is common among in all ages of people and more in pediatric, geriatric, psychiatric patients. In terms of permeability, sublingual area of oral cavity is more permeable than buccal area which is in turn is more permeable than palatal area. Different techniques are used to formulate the sublingual dosage forms. Sublingual drug administration is applied in field of cardiovascular drugs, steroids, enzymes and some barbiturates. This review highlights advantages, disadvantages, different sublingual formulation such as tablets and films, evaluation. Key Words: Sublingual delivery, techniques, improved bioavailability, evaluation. INTRODUCTION and direct access to systemic circulation, the oral Drugs have been applied to the mucosa for topical mucosal route is suitable for drugs, which are application for many years. However, recently susceptible to acid hydrolysis in the stomach or there has been interest in exploiting the oral cavity which are extensively metabolized in the liver. -

Vaccine Administration Joellen Wolicki, BSN, RN and Elaine Miller, RN, BSN, MPH
Vaccine Administration JoEllen Wolicki, BSN, RN and Elaine Miller, RN, BSN, MPH This chapter summarizes best practices related to vaccine administration, a key factor in ensuring vaccination is as safe NOTES and effective as possible. Administration involves a series of actions: assessing patient vaccination status and determining needed vaccines, screening for contraindications and precautions, educating patients, preparing and administering vaccines properly, and documenting the vaccines administered. Professional standards for medication administration, manufacturer instructions, and organizational policies and procedures should always be followed when applicable. 6 Staff Training and Education Policies should be in place to validate health care professionals’ knowledge of, and skills in, vaccine administration. All health care professionals should receive comprehensive, competency- based training before administering vaccines. Training, including an observation component, should be integrated into health care professionals’ education programs including orientation for new staff and annual continuing education requirements for all staff. In addition, health care professionals should receive educational updates as needed, such as when vaccine administration recommendations are updated or when new vaccines are added to the facility’s inventory. Training should also be offered to temporary staff who may be filling in on days when the facility is short-staffed or helping during peak periods of vaccine administration such as influenza season. Once initial training has been completed, accountability checks should be in place to ensure staff follow all vaccine administration policies and procedures. Before Administering Vaccine Health care professionals should be knowledgeable about appropriate techniques to prepare and care for patients when administering vaccines. Assess for Needed Vaccines The patient’s immunization status should be reviewed at every health care visit. -

22428 Moxifloxacin Statisical PREA
U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research Office of Translational Science Office of Biostatistics S TATISTICAL R EVIEW AND E VALUATION CLINICAL STUDIES NDA/Serial Number: 22,428 Drug Name: Moxifloxacin AF (moxifloxacin hydrochloride ophthalmic solution) 0.5% Indication(s): Treatment of bacterial conjunctivitis Applicant: Alcon Pharmaceuticals, Ltd. Date(s): Letter date:21 May 2010; Filing date: 18 June, 2010; PDUFA goal date: 19 November 2010 Review Priority: Priority Biometrics Division: Anti-infective and Ophthalmology Products Statistical Reviewer: Mark. A. Gamalo, Ph.D. Concurring Reviewers: Yan Wang, Ph.D. Medical Division: Anti-infective and Ophthalmology Products Clinical Reviewer: Lucious Lim, M.D. Project Manager: Lori Gorski Keywords: superiority, Moxifloxacin hydrochloride ophthalmic solution, bacterial conjunctivitis, bulbar conjunctival injection, conjunctival discharge/exudate TABLE OF CONTENTS TABLE OF CONTENTS................................................................................................................ 2 LIST OF TABLES.......................................................................................................................... 3 1. EXECUTIVE SUMMARY ...................................................................................................... 4 1. 1 Conclusions and Recommendations..................................................................................... 4 1. 2 Brief Overview of Clinical Studies ..................................................................................... -

Chapter 1 Controlling Drug Delivery
chapter 1 Controlling drug delivery Overview In this chapter we will: & differentiate drug delivery systems according to their physical state & differentiate drug delivery systems according to their route of administration & differentiate drug delivery systems according to their type of drug release & discuss drug transport across epithelial barriers. Introduction KeyPoints & Continued developments in Pharmacotherapy can be defined as the treatment chemistry, molecular biology and prevention of illness and disease by means of and genomics support the drugs of chemical or biological origin. It ranks discovery and developments among the most important methods of medical of new drugs and new drug treatment, together with surgery, physical targets. & treatment, radiation and psychotherapy. There The drug delivery system are many success stories concerning the use of employed can control the pharmacological action of a drugs and vaccines in the treatment, prevention drug, influencing its and in some cases even eradication of diseases pharmacokinetic and (e.g. smallpox, which is currently the only subsequent therapeutic human infectious disease completely profile. eradicated). Although it is almost impossible to estimate the exact extent of the impact of pharmacotherapy on human health, there can be no doubt that pharmacotherapy, together with improved sanitation, better diet and better housing, has improved people’s health, life expectancy and quality of life. Tip Unprecedented developments in genomics Combinatorial chemistry is a way to and molecular biology today offer a plethora of build a variety of structurally related new drug targets. The use of modern chemical drug compounds rapidly and synthetic methods (such as combinatorial systematically. These are assembled chemistry) enables the syntheses of a large from a range of molecular entities number of new drug candidates in shorter times which are put together in different ‘ ’ than ever before. -
Informed Consent for Medication, Zyprexa
DEPARTMENT OF HEALTH SERVICES STATE OF WISCONSIN Division of Care and Treatment Services 42 CFR483.420(a)(2) F-24277 (09/2016) DHS 134.31(3)(o) DHS 94.03 & 94.09 §§ 51.61(1)(g) & (h) INFORMED CONSENT FOR MEDICATION Dosage and / or Side Effect information last revised on 04/16/2021 Completion of this form is voluntary. If not completed, the medication cannot be administered without a court order unless in an emergency. This consent is maintained in the client’s record and is accessible to authorized users. Name – Patient / Client (Last, First MI) ID Number Living Unit Date of Birth , Name – Individual Preparing This Form Name – Staff Contact Name / Telephone Number – Institution ANTICIPATED RECOMMENDED MEDICATION CATEGORY MEDICATION DOSAGE DAILY TOTAL DOSAGE RANGE RANGE Antipsychotic / Bipolar Agent Zyprexa oral tablet; Oral: 2.5 mg-50 mg with most doses in Zyprexa Zydis oral the 2.5 mg-20 mg range disintegrating tablet; IM: 5 mg-10 mg per dose, up to 3 doses Zyprexa Intramuscular 24 hours Injection; Long Acting Injectable: 150 mg-300 mg Zyprexa Relprevv IM every 2 weeks, Intramuscluar Injection 300 mg-405 mg IM every 4 weeks (olanzapine) The anticipated dosage range is to be individualized, may be above or below the recommended range but no medication will be administered without your informed and written consent. Recommended daily total dosage range of manufacturer, as stated in Physician’s Desk Reference (PDR) or another standard reference. This medication will be administered Orally Injection Other – Specify: 1. Reason for Use of Psychotropic Medication and Benefits Expected (note if this is ‘Off-Label’ Use) Include DSM-5 diagnosis or the diagnostic “working hypothesis.” 2. -

Drug Administration
Chapter 3: Drug Administration 2 Contact Hours By: Katie Ingersoll, RPh, PharmD Author Disclosure: Katie Ingersoll and Elite do not have any actual or Questions regarding statements of credit and other customer service potential conflicts of interest in relation to this lesson. issues should be directed to 1-888-666-9053. This lesson is $12.00. Universal Activity Number (UAN): 0761-9999-17-079-H01-P Educational Review Systems is accredited by the Activity Type: Knowledge-based Accreditation Council of Pharmacy Education (ACPE) Initial Release Date: April 1, 2017 as a provider of continuing pharmaceutical education. Expiration Date: April 1, 2019 This program is approved for 2 hours (0.2 CEUs) of Target Audience: Pharmacists in a community-based setting. continuing pharmacy education credit. Proof of participation will be posted to your NABP CPE profile within 4 to 6 To Obtain Credit: A minimum test score of 70 percent is needed weeks to participants who have successfully completed the post-test. to obtain a credit. Please submit your answers either by mail, fax, or Participants must participate in the entire presentation and complete online at Pharmacy.EliteCME.com. the course evaluation to receive continuing pharmacy education credit. Learning objectives After completion of this course, healthcare professionals will be able Discuss the administration of medications in patients using enteral to: and parenteral nutrition. Describe the eight rights of medication administration. Discuss special considerations for administering medications in Explain the administration of enteral and parenteral medications. pediatric and geriatric patients. Introduction Medication errors that occur at the point of drug administration poised to reduce the frequency of medication administration errors. -

Product Monograph
PRODUCT MONOGRAPH Pr SANDOZ ONDANSETRON ODT Ondansetron Orally Disintegrating Tablets 4 mg and 8 mg ondansetron Manufacturer Standard Pr SANDOZ ONDANSETRON Ondansetron Tablets 4 mg and 8 mg ondansetron (as ondansetron hydrochloride dihydrate) Manufacturer Standard PrONDANSETRON INJECTION USP (ondansetron hydrochloride dihydrate) 2 mg/mL PrONDANSETRON HYDROCHLORIDE DIHYDRATE INJECTION Ondansetron Injection Manufacturer Standard 2 mg/mL Ondansetron (as ondansetron hydrochloride dihydrate) for injection Antiemetic (5-HT3-receptor antagonist) Sandoz Canada Inc. Date of Preparation: 145 Jules-Léger September 26, 2016 Boucherville, Québec, Canada J4B 7K8 Control No.: 198381 Ondansetron by Sandoz Page 1 of 43 Table of Contents PART I: HEALTH PROFESSIONAL INFORMATION .......................................................... 3 SUMMARY PRODUCT INFORMATION ................................................................................. 3 INDICATIONS AND CLINICAL USE ....................................................................................... 4 CONTRAINDICATIONS ............................................................................................................ 4 WARNINGS AND PRECAUTIONS .......................................................................................... 5 ADVERSE REACTIONS ............................................................................................................ 7 DRUG INTERACTIONS ............................................................................................................ -

Inhalation Therapy - Approaches and Challenges
Online - 2455-3891 Vol 11, Issue 4, 2018 Print - 0974-2441 Review Article INHALATION THERAPY - APPROACHES AND CHALLENGES SAYANI BHATTACHARYYA*, BHARANI S SOGALI Department of Pharmaceutics, Krupanidhi College of Pharmacy, No: 12/1 Carmelaram Road, Chikka Bellandur, Varthur, Hobli, Carmelaram Post, Bengaluru – 560 035, Karnataka, India. Email:[email protected] Received: 05 December 2017, Revised and Accepted: 02 January 2018 ABSTRACT Inhalation therapy is an effective way for local and systemic delivery of miscellaneous drugs for pulmonary and non-pulmonary diseases. The inhalation therapy aims to target specific cells or regions of the lung, bypassing the lung’s clearance mechanisms and thereby providing high retention of the drug for longer periods. It helps in improved penetration of intravenously administered antibiotics into lung parenchymal tissue and bronchial secretions, and as a result, their potential systemic toxicity is reduced when given over prolonged periods of time. The advancement in device technology supports the development of more efficient therapy in the form of delivering finer particles into the lung in large doses. Therefore, meticulous daily management of lung disease, together with prompt, aggressive treatment of exacerbations can be achieved through inhalation to preserve lung function. This review summarizes the features of inhalation delivery devices, their advantages and limitations, challenges in formulation and brief description of novel technologies currently marketed. Keywords: Lung, Inhalation, Target, Local delivery, Systemic delivery, Novel technologies. © 2018 The Authors. Published by Innovare Academic Sciences Pvt Ltd. This is an open access article under the CC BY license (http://creativecommons. org/licenses/by/4. 0/) DOI: http://dx.doi.org/10.22159/ajpcr.2018.v11i4.24117 INTRODUCTION while drug localized at the upper airways are removed by ciliated cells in the epithelial region. -
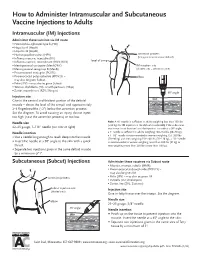
How to Administer Intramuscular and Subcutaneous Vaccines to Adults
How to Administer Intramuscular and Subcutaneous Vaccine Injections to Adults Intramuscular (IM) Injections Administer these vaccines via IM route • Haemophilus influenzae type b (Hib) • Hepatitis A (HepA) • Hepatitis B (HepB) • Human papillomavirus (HPV) acromion process (bony prominence above deltoid) • Influenza vaccine, injectable (IIV) • level of armpit • Influenza vaccine, recombinant (RIV3; RIV4) • Meningococcal conjugate (MenACWY) IM injection site • Meningococcal serogroup B (MenB) (shaded area = deltoid muscle) • Pneumococcal conjugate (PCV13) • Pneumococcal polysaccharide (PPSV23) – elbow may also be given Subcut • Polio (IPV) – may also be given Subcut • Tetanus, diphtheria (Td), or with pertussis (Tdap) • Zoster, recombinant (RZV; Shingrix) 90° angle Injection site skin Give in the central and thickest portion of the deltoid muscle – above the level of the armpit and approximately subcutaneous tissue 2–3 fingerbreadths (~2") below the acromion process. See the diagram. To avoid causing an injury, do not inject muscle too high (near the acromion process) or too low. Needle size Note: A ⅝" needle is sufficient in adults weighing less than 130 lbs (<60 kg) for IM injection in the deltoid muscle only if the subcutane- 22–25 gauge, 1–1½" needle (see note at right) ous tissue is not bunched and the injection is made at a 90° angle; Needle insertion a 1" needle is sufficient in adults weighing 130–152 lbs (60–70 kg); a 1–1½" needle is recommended in women weighing 153–200 lbs • Use a needle long enough to reach deep into the muscle. (70–90 kg) and men weighing 153–260 lbs (70–118 kg); a 1½" needle • Insert the needle at a 90° angle to the skin with a quick is recommended in women weighing more than 200 lbs (91 kg) or thrust.