Personal Radiation Monitoring
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Proper Use of Radiation Dose Metric Tracking for Patients Undergoing Medical Imaging Exams
Proper Use of Radiation Dose Metric Tracking for Patients Undergoing Medical Imaging Exams Frequently Asked Questions Introduction In August of 2021, the American Association of Physicists in Medicine (AAPM), the American College of Radiology (ACR), and the Health Physics Society (HPS) jointly released the following position statement advising against using information about a patient’s previous cumulative dose information from medical imaging exams to decide the appropriateness of future imaging exams. This statement was also endorsed by the Radiological Society of North America (RSNA). It is the position of the American Association of Physicists in Medicine (AAPM), the American College of Radiology (ACR), and the Health Physics Society (HPS) that the decision to perform a medical imaging exam should be based on clinical grounds, including the information available from prior imaging results, and not on the dose from prior imaging-related radiation exposures. AAPM has long advised, as recommended by the International Commission on Radiological Protection (ICRP), that justification of potential patient benefit and subsequent optimization of medical imaging exposures are the most appropriate actions to take to protect patients from unnecessary medical exposures. This is consistent with the foundational principles of radiation protection in medicine, namely that patient radiation dose limits are inappropriate for medical imaging exposures. Therefore, the AAPM recommends against using dose values, including effective dose, from a patient’s prior imaging exams for the purposes of medical decision making. Using quantities such as cumulative effective dose may, unintentionally or by institutional or regulatory policy, negatively impact medical decisions and patient care. This position statement applies to the use of metrics to longitudinally track a patient’s dose from medical radiation exposures and infer potential stochastic risk from them. -

Cumulative Radiation Dose in Patients Admitted with Subarachnoid Hemorrhage: a Prospective PATIENT SAFETY Study Using a Self-Developing Film Badge
Cumulative Radiation Dose in Patients Admitted with Subarachnoid Hemorrhage: A Prospective PATIENT SAFETY Study Using a Self-Developing Film Badge A.C. Mamourian BACKGROUND AND PURPOSE: While considerable attention has been directed to reducing the x-ray H. Young dose of individual imaging studies, there is little information available on the cumulative dose during imaging-intensive hospitalizations. We used a radiation-sensitive badge on 12 patients admitted with M.F. Stiefel SAH to determine if this approach was feasible and to measure the extent of their x-ray exposure. MATERIALS AND METHODS: After obtaining informed consent, we assigned a badge to each of 12 patients and used it for all brain imaging studies during their ICU stay. Cumulative dose was deter- mined by quantifying exposure on the badge and correlating it with the number and type of examinations. RESULTS: The average skin dose for the 3 patients who had only diagnostic DSA without endovascular intervention was 0.4 Gy (0.2–0.6 Gy). The average skin dose of the 8 patients who had both diagnostic DSA and interventions (eg, intra-arterial treatment of vasospasm and coiling of aneurysms) was 0.9 Gy (1.8–0.4 Gy). One patient had only CT examinations. There was no effort made to include or exclude the badge in the working view during interventions. CONCLUSIONS: It is feasible to incorporate a film badge that uses a visual scale to monitor the x-ray dose into the care of hospitalized patients. Cumulative skin doses in excess of 1 Gy were not uncommon (3/12) in this group of patients with acute SAH. -

The Ionising Radiations Regulations 2017
Title of document 4 ONR GUIDE THE IONISING RADIATIONS REGULATIONS 2017 Document Type: Nuclear Safety Technical Inspection Guide Unique Document ID and NS-INSP-GD-054 Revision 7 Revision No: Date Issued: April 2019 Review Date: April 2022 Professional Lead – Approved by: K McDonald Operational Inspection Record Reference: CM9 Folder 1.1.3.979. (2020/209725) Rev 6: Update to include reference to the Ionising Radiations Regulations 2017 Revision commentary: Rev 7: Updated review period TABLE OF CONTENTS 1. INTRODUCTION ................................................................................................................. 2 2. PURPOSE AND SCOPE ..................................................................................................... 2 3. THE IONISING RADIATIONS REGULATIONS 2017 .......................................................... 2 4. PURPOSE OF THE IONISING RADIATIONS REGULATIONS 2017 ................................. 3 5. GUIDANCE ON ARRANGEMENTS FOR THE IONISING RADIATIONS REGULATIONS 2017 ..................................................................................................................................... 3 6. GUIDANCE ON INSPECTION OF ARRANGEMENTS AND THEIR IMPLEMENTATION.. 5 7. FURTHER READING ........................................................................................................ 16 8. DEFINITIONS .................................................................................................................... 16 9. APPENDICES ................................................................................................................... -

Dosimeter Comparison Chart
DOSIMETER COMPARISON CHART Instadose®+ Instadose® EPD or APD TLD Dosimeter OSL Dosimeter Dosimeter Dosimeter Dosimeter Cost $ $ $ $$$$ Photon Photon Photon Photon Photon Beta Beta Neutron DEEP - Hp(10) DEEP - Hp(10) Neutron Neutron Measurements SHALLOW - Hp(0.07) SHALLOW - Hp(0.07) DEEP - Hp(10) DEEP - Hp(10) DEEP - Hp(10) SHALLOW - Hp(0.07) SHALLOW - Hp(0.07) SHALLOW - Hp(0.07) EYE - Hp(3) EYE - Hp(3) Read Out Accumulated Accumulated Accumulated Accumulated Accumulated (On-Demand) (On-Demand) (Lab Processing) (Lab Processing) & Dose Rate Unlimited On- Demand Dose Reads Re-Calibration Required Wearer Engagement High High Low Low High Online Management Portal (Website) Provider Dependent NVLAP Highly manual Accreditation process Immediate Online Badge Reassignment Provider Dependent Archiving Dose (Wearer) Meets Legal Highly manual Dose of Record process for meeting Requirements accreditation NO Collection/ Must be collected to Redistribution meet legal dose of Required record requirements Read/View Dose Data on Your Smartphone Automatic (Calendar-set) Dose Reads Wireless Radio Transmission of USB plug-in to PC Dose Data Communication Immediate High Dose Alerts Upon Successful Communication Instadose Dosimeters use direct ion storage (DIS) TLD (Thermoluminescent OSL (Optically EPDs (Electronic Descriptions technology to measure ionizing radiation through Dosimeter) measures Stimulated Personal Dosimeter) interactions that take place between the non- ionizing radiation Luminescence or APDs (Active volatile analog memory cell, which is surrounded exposure by assessing Dosimeter) measures Personal Dosimeter) by a gas filled ion chamber with a floating gate the intensity of visible ionizing radiation makes use of a diode that creates an electric charge enabling ionized light emitted by a crystal exposure when radiation (silicon or PIN, etc.) to particles to be measured by the change in the inside the detector when energy deposited in the detect “charges” induced electric charge created. -
New Techniques of Low Level Environmental Radiation Monitoring at Jlab
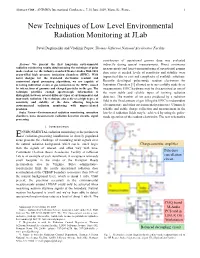
Abstract #188 - ANIMMA International Conference, 7-10 June 2009, Marseille, France 1 New Techniques of Low Level Environmental Radiation Monitoring at JLab Pavel Degtiarenko and Vladimir Popov, Thomas Jefferson National Accelerator Facility contribution of operational gamma dose was evaluated Abstract—We present the first long-term environmental indirectly during special measurements. Direct continuous radiation monitoring results obtained using the technique of pulse measurements and long-term monitoring of operational gamma mode readout for the industry-standard Reuter-Stokes RSS-1013 dose rates at needed levels of sensitivity and stability were argon-filled high pressure ionization chambers (HPIC). With novel designs for the front-end electronics readout and impractical due to cost and complexity of available solutions. customized signal processing algorithms, we are capable of Recently developed pulse-mode readout electronics for detecting individual events of gas ionization in the HPIC, caused Ionization Chambers [1] allowed us to successfully make these by interactions of gammas and charged particles in the gas. The measurements. HPIC hardware may be characterized as one of technique provides enough spectroscopic information to the most stable and reliable types of ionizing radiation distinguish between several different types of environmental and detectors. The number of ion pairs produced by a radiation man-made radiation. The technique also achieves a high degree of sensitivity and stability of the data, allowing long-term field in the fixed amount of gas filling the HPIC is independent environmental radiation monitoring with unprecedented of temperature and other environmental parameters. Ultimately precision. reliable and stable charge collection and measurement in the Index Terms—Environmental radiation monitoring, ionization low-level radiation fields may be achieved by using the pulse- chambers, noise measurement, radiation detection circuits, signal mode operation of the readout electronics. -
An Overview of NCRP Commentary No. 19 Objectives of This Presentation
Key Elements of Preparing Emergency Responders for Nuclear and Radiological Terrorism An Overview of NCRP Commentary No. 19 Objectives of this Presentation • Provide an overview of the Commentary to allow audiences to become familiar with the material. • Focus on key points discussed in the Commentary. • Provide additional explanations for the recommendations. Background • Commentary was prepared at the request of the Department of Homeland Security (DHS). • Recommendations are intended for DHS and state and local authorities who prepare emergency responders for terrorist incidents involving radiation or radioactive materials. Background • Commentary builds on previous NCRP reports – NCRP Report No. 65, Management of Persons Accidentally Contaminated with Radionuclides (1980). – NCRP Report No. 138, Management of Terrorist Events Involving Radioactive Material (2001). Background • Commentary No. 19 is limited to the key elements of preparing emergency responders for nuclear and radiological terrorism. • Details of implementation are left to the DHS in concert with state and local authorities. Serving on the NCRP Scientific Committee SC 2-1 that prepared this Commentary were: John W. Poston, Sr., Chairman Texas A&M University, College Station, Texas Steven M. Becker Brian Dodd The University of Alabama at Birmingham BDConsulting School of Public Health Las Vegas, Nevada Birmingham, Alabama John R. Frazier Brooke Buddemeier Auxier & Associates, Inc. Department of Homeland Security Knoxville, Tennessee Washington, D.C. Fun H. Fong, Jr. Jerrold T. Bushberg Centers for Disease Control and Prevention University of California, Davis Atlanta, Georgia Sacramento, California Ronald E. Goans John J. Cardarelli MJW Corporation Environmental Protection Agency Clinton, Tennessee Cincinnati, Ohio Ian S. Hamilton W. Craig Conklin Baylor College of Medicine Department of Homeland Security Houston, Texas Washington, D.C. -

Radiation Glossary
Radiation Glossary Activity The rate of disintegration (transformation) or decay of radioactive material. The units of activity are Curie (Ci) and the Becquerel (Bq). Agreement State Any state with which the U.S. Nuclear Regulatory Commission has entered into an effective agreement under subsection 274b. of the Atomic Energy Act of 1954, as amended. Under the agreement, the state regulates the use of by-product, source, and small quantities of special nuclear material within said state. Airborne Radioactive Material Radioactive material dispersed in the air in the form of dusts, fumes, particulates, mists, vapors, or gases. ALARA Acronym for "As Low As Reasonably Achievable". Making every reasonable effort to maintain exposures to ionizing radiation as far below the dose limits as practical, consistent with the purpose for which the licensed activity is undertaken. It takes into account the state of technology, the economics of improvements in relation to state of technology, the economics of improvements in relation to benefits to the public health and safety, societal and socioeconomic considerations, and in relation to utilization of radioactive materials and licensed materials in the public interest. Alpha Particle A positively charged particle ejected spontaneously from the nuclei of some radioactive elements. It is identical to a helium nucleus, with a mass number of 4 and a charge of +2. Annual Limit on Intake (ALI) Annual intake of a given radionuclide by "Reference Man" which would result in either a committed effective dose equivalent of 5 rems or a committed dose equivalent of 50 rems to an organ or tissue. Attenuation The process by which radiation is reduced in intensity when passing through some material. -

``Low Dose``And/Or``High Dose``In Radiation Protection: a Need To
IAEA-CN-67/154 "LOW DOSE" AND/OR "HIGH DOSE" IN RADIATION PROTECTION: A NEED TO SETTING CRITERIA FOR DOSE CLASSIFICATION Mehdi Sohrabi National Radiation Protection Department & XA9745670 Center for Research on Elevated Natural Radiation Atomic Energy Organization of Iran, Tehran ABSTRACT The "low dose" and/or "high dose" of ionizing radiation are common terms widely used in radiation applications, radiation protection and radiobiology, and natural radiation environment. Reading the title, the papers of this interesting and highly important conference and the related literature, one can simply raise the question; "What are the levels and/or criteria for defining a low dose or a high dose of ionizing radiation?". This is due to the fact that the criteria for these terms and for dose levels between these two extreme quantities have not yet been set, so that the terms relatively lower doses or higher doses are usually applied. Therefore, setting criteria for classification of radiation doses in the above mentioned areas seems a vital need. The author while realizing the existing problems to achieve this important task, has made efforts in this paper to justify this need and has proposed some criteria, in particular for the classification of natural radiation areas, based on a system of dose limitation. In radiation applications, a "low dose" is commonly associated to applications delivering a dose such as given to a patient in a medical diagnosis and a "high dose" is referred to a dose in applications such as radiotherapy, mutation breeding, control of sprouting, control of insects, delay ripening, and sterilization having a range of doses from 1 to 105 Gy, for which the term "high dose dosimetry" is applied [1]. -

Radiation Monitoring Units: Planning and Operational Guidance
HPA-CRCE-017 Radiation Monitoring Units: Planning and Operational Guidance N J Thompson, M J Youngman, J Moody, N P McColl, D R Cox, J Astbury, S Webb and S L Prosser © Health Protection Agency Approval: June 2011 Centre for Radiation, Chemical and Environmental Hazards Publication: July 2011 Environmental Hazards and Emergencies Department £21.00 Chilton, Didcot, Oxfordshire OX11 0RQ ISBN 978-0-85951-690-7 This report from HPA Centre for Radiation, Chemical and Environmental Hazards reflects understanding and evaluation of the current scientific evidence as presented and referenced in this document. EXECUTIVE SUMMARY EXECUTIVE SUMMARY In the event of a radiation emergency, there may be a requirement to establish a Radiation Monitoring Unit (RMU) to undertake radiation monitoring of the public (population monitoring). A RMU is used to determine levels of radioactive contamination in or on people and any subsequent requirement for decontamination. It will also inform decisions regarding the need for any medical interventions for persons contaminated with radioactive material. This document is to aid emergency planners when producing specific plans for radiation monitoring units. It is provided in two distinct sections. The first substantive section of the report (section 4) provides detailed information for emergency planners including information to inform the selection of suitable accommodation and equipment. A basic description of the process for people monitoring and data collection is also provided in this section since these may impact upon these early planning considerations. The second substantive section of the report (section 5) focuses on the more detailed operational aspects of the RMU’s lifecycle and begins with a structured discussion to aid decision regarding RMU activation. -

Radiation Protection
C.I.12 Radiation Protection Chapter 12 of the FSAR should provide information on radiation protection methods and estimated occupational radiation exposures of operating and construction personnel during normal operation and AOO. (In particular, AOO may include refueling; purging; fuel handling and storage; radioactive material handling, processing, use, storage, and disposal; maintenance; routine operational surveillance; ISI; and calibration.) Specifically, this chapter should provide information on facility and equipment design, planning and procedures programs, and techniques and practices employed by the applicant to meet the radiation protection standards set forth in 10 CFR Part 20, and to be consistent with the guidance given in the appropriate regulatory guides, where the practices set forth in such guides are used to implement NRC regulations. As warranted, this chapter should specifically reference needed information that appears in other chapters of the FSAR. The information that is typically present in Chapter 12, includes a discussion of how radiation practices are incorporated into plant policy and design decisions; a general description of the radiation source terms; radiation protection design features, including a description of plant shielding, ventilation systems, and area radiation and airborne radioactivity monitoring instrumentation; a dose assessment for operating and construction personnel; and a discussion of the design of the health physics facilities. C.I.12.1 Ensuring that Occupational Radiation Exposures Are As Low As Is Reasonably Achievable C.I.12.1.1 Policy Considerations The applicant should describe the management policy and organizational structure related to ensuring that occupational radiation exposures are ALARA. The applicant should describe the applicable responsibilities and related activities to be performed by management personnel who have responsibility for radiation protection and the policy of maintaining occupational exposures ALARA. -

Major Radiological Or Nuclear Incidents
Major Radiological or Nuclear Incidents: Potential Health and Medical Implications July 2018 This ASPR TRACIE document provides an overview of the potential health and medical response and recovery needs following a radiological or nuclear incident and outlines available resources for planners. The list of considerations is not exhaustive, but does reflect an environmental scan of publications and resources available on past incident response, numerous exercises, local and regional preparedness planning, and significant research on the subject. Those leading preparedness efforts for, or response and recovery from, a radiological or nuclear incident may use this document as a reference, while focusing on the assessments and issues specific to their communities and unmet needs as they are recognized. It is important to note, however, that entities engaged in planning for or responding to radiological incidents should consult with the radiation protection authorities in their state in addition to federal resources. Most states and local jurisdictions have existing plans for responding to radiological incidents and these plans can provide local information for health and medical providers. The U.S. Department of Health and Human Services (HHS) Radiation Emergency Medical Management (REMM) and the Centers for Disease Control and Prevention (CDC) Radiation Emergencies sites provide guidance for healthcare providers, primarily physicians, about clinical diagnosis and treatment of radiation injury and response issues during radiological and nuclear -
Practical Radiation Monitoring
Good Practice Guide No. 30 Practical Radiation Monitoring Issue 2 Measurement Good Practice Guide No. 30 Practical Radiation Monitoring Ó Queen’s Copyright Printer and Controller of HMSO, 2014 ISSN 1368-6550 National Physical Laboratory Hampton Road, Teddington, Middlesex, TW11 0LW Extracts from this report may be reproduced provided the source is acknowledged and the extract is not taken out of context. Approved on behalf of the Managing Director, NPL, by Dr Steven Judge Good Practice Guide No. 30, Issue 2 Acknowledgements This second issue of this Good Practice Guide has been produced by a working group of the Ionising Radiation Metrology Forum. Membership of the working group was as follows: Peter Burgess Nuvia Ltd Rob Corby Magnox Ltd Denise Delahunty RRPPS Birmingham Steven Judge National Physical Laboratory Lynsey Keightley National Physical Laboratory Clare Lee National Physical Laboratory Tony Richards Consultant (Leeds) John Simpson Consultant Mike Woods IRMC Ludovic Chevallereau Amec Ltd Thanks are due to all those that contributed to both the first and second issues. Thanks also go to Pauline Leggat, formerly of the National Physical Laboratory, for drawing the cartoons used in the Guide. i Good Practice Guide No. 30, Issue 2 Foreword This Good Practice Guide has been written by a working party of experts from the UK Ionising Radiation Metrology Forum*, it replaces the first issue published in 2002. It describes procedures and methods for assessing radiation levels, outlines the thought processes needed to carry out the measurements and gives practical advice. The methods described are general and based on currently accepted good practice. We hope the document will standardise the approach to radiation monitoring.