Anterior and Medial Thigh Muscles
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Study of Variation of Great Saphenous Veins and Its Surgical Significance (Original Study)
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 17, Issue 2 Ver. 10 February. (2018), PP 21-26 www.iosrjournals.org Study of Variation of Great Saphenous Veins and Its Surgical Significance (Original Study) Dr Surekha W. Meshram1, Dr. Yogesh Ganorkar2, Dr V.P. Rukhmode3, Dr. Tarkeshwar Golghate4 1(M.B.B.S,M.D) Associate Professor, Dept. of Anatomy Govt. Medical College Gondia, Maharashtra 2(M.B.B.S,M.D) Assistant Professor, Dept. of Anatomy Govt. Medical College Gondia, Maharashtra 3 (M.B.B.S, M.S) Professor and Head, Dept. of Anatomy Govt. Medical College Gondia, Maharashtra 4(M.B.B.S, M.D) Assiciate Professor, Dept. of Anatomy Govt. Medical College, Nagpur, Maharashtra Corresponding Author: Dr. Surekha W. Meshram Abstract Introduction: Veins of lower limbs are more involves for various venous disorders as compare to upper limbs. Most common venous disorders occurring in lower limbs are varicose veins, deep venous thrombosis and venous ulcers. Varicose veins are found in large population of world affecting both the males and females. Surgical operations are performed in all over the world to cure it. In the varicose vein surgery, surgeon successfully do the ligation as well as stripping of the great saphenous vein and its tributaries. Duplication of a great saphenous vein can be a potential cause for recurrent varicose veins after surgery as well as complications may occur during the surgery. Method: The present study was done by dissection method on 50 lower limbs of cadavers. Its aim was to identify the incidence and pattern of duplication of long saphenous vein in Indian population. -

Patellofemoral Syndrome: Evaluation & Management Scott Sevinsky MSPT
Patellofemoral Syndrome: Evaluation & Management Scott Sevinsky MSPT What is Patellofemoral Syndrome? Patellofemoral syndrome (PFS) is a term commonly used to describe a condition where the patella ‘tracks’ or glides improperly between the femoral condyles. This improper tracking causes pain in the anterior knee and may lead to degenerative changes or dislocation of the knee cap. To be more precise the term ‘anterior knee pain’ is suggested to encompass all pain-related problems of the anterior part of the knee. By excluding anterior knee pain due to intra-articular pathology, peripatellar tendinitis or bursitis, plica syndromes, Sinding Larsen’s disease, Osgood Schlatter’s disease, neuromas and other rarely occurring pathologies it is suggested that remaining patients with a clinical presentation of anterior knee pain could be diagnosed with PFPS. The term ‘patellofemoral’ is used as no distinction can be made as to which specific structure of the patella or femur is affected. The term ‘chondromalacia patellae’, defined at the beginning of the 20th century to describe pathological changes of the retropatellar cartilage,7,8 was for half a century, used as a synonym for the syndrome of patellofemoral pain. However, several studies during the last 2 decades have shown a poor correlation between articular cartilage damage and the still not well-defined pain mechanism of retropatellar pain. Review of Knee Anatomy 1. Femur – thigh bone; longest bone in the body. · Lateral femoral condyle larger than medial condyle & projects farther anteriorly. · Medial femoral condyle longer anterior to posterior · Distal surfaces are convex · Intercondylar (trochlear) notch: groove in which the patella glides or ‘tracks’ 2. -

Study Guide Medical Terminology by Thea Liza Batan About the Author
Study Guide Medical Terminology By Thea Liza Batan About the Author Thea Liza Batan earned a Master of Science in Nursing Administration in 2007 from Xavier University in Cincinnati, Ohio. She has worked as a staff nurse, nurse instructor, and level department head. She currently works as a simulation coordinator and a free- lance writer specializing in nursing and healthcare. All terms mentioned in this text that are known to be trademarks or service marks have been appropriately capitalized. Use of a term in this text shouldn’t be regarded as affecting the validity of any trademark or service mark. Copyright © 2017 by Penn Foster, Inc. All rights reserved. No part of the material protected by this copyright may be reproduced or utilized in any form or by any means, electronic or mechanical, including photocopying, recording, or by any information storage and retrieval system, without permission in writing from the copyright owner. Requests for permission to make copies of any part of the work should be mailed to Copyright Permissions, Penn Foster, 925 Oak Street, Scranton, Pennsylvania 18515. Printed in the United States of America CONTENTS INSTRUCTIONS 1 READING ASSIGNMENTS 3 LESSON 1: THE FUNDAMENTALS OF MEDICAL TERMINOLOGY 5 LESSON 2: DIAGNOSIS, INTERVENTION, AND HUMAN BODY TERMS 28 LESSON 3: MUSCULOSKELETAL, CIRCULATORY, AND RESPIRATORY SYSTEM TERMS 44 LESSON 4: DIGESTIVE, URINARY, AND REPRODUCTIVE SYSTEM TERMS 69 LESSON 5: INTEGUMENTARY, NERVOUS, AND ENDOCRINE S YSTEM TERMS 96 SELF-CHECK ANSWERS 134 © PENN FOSTER, INC. 2017 MEDICAL TERMINOLOGY PAGE III Contents INSTRUCTIONS INTRODUCTION Welcome to your course on medical terminology. You’re taking this course because you’re most likely interested in pursuing a health and science career, which entails proficiencyincommunicatingwithhealthcareprofessionalssuchasphysicians,nurses, or dentists. -

Luxating Patella
LUXATING PATELLA What is a luxating patella? The patella, or kneecap, is normally located in the center of the knee joint. The term luxating means, “out of place” or “dislocated”. Therefore, a luxating patella is a kneecap that moves out of its normal location. What causes this? The muscles of the thigh attach to the top of the kneecap. There is a ligament, the patellar ligament, running from the bottom of the kneecap to a point on the tibia just below the knee joint. When the thigh muscles contract, force is transmitted through the patella and patellar ligament to a point on the top of the tibia. This results in extension or straightening of the knee. The patella stays in the center of the leg because the point of attachment of the patellar ligament is on the midline and because the patella slides in a groove on the lower end of the femur (the bone between the knee and the hip). The patella luxates because the point of attachment of the patellar ligament is not on the midline of the tibia. It is almost always located too far medial (toward the middle of the body). As the thigh muscles contract, the force is pulled medial. After several months or years of this abnormal movement, the inner side of the groove in the femur wears down. Once the side of the groove wears down, the patella is then free to dislocate. When this occurs, the dog has difficulty bearing weight on the leg. It may learn how to kick the leg and snap the patella back into its normal location. -
Intramedullary Nailing for Femur Fracture Management a Guide for Parents
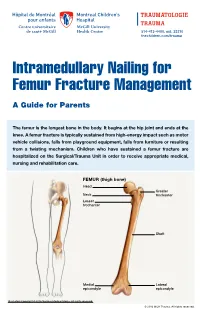
514-412-4400, ext. 23310 thechildren.com/trauma Intramedullary Nailing for Femur Fracture Management A Guide for Parents The femur is the longest bone in the body. It begins at the hip joint and ends at the knee. A femur fracture is typically sustained from high-energy impact such as motor vehicle collisions, falls from playground equipment, falls from furniture or resulting from a twisting mechanism. Children who have sustained a femur fracture are hospitalized on the Surgical/Trauma Unit in order to receive appropriate medical, nursing and rehabilitation care. FEMUR (thigh bone) Head Greater Neck trochanter Lesser trochanter Shaft Medial Lateral epicondyle epicondyle Illustration Copyright © 2016 Nucleus Medical Media, All rights reserved. © 2016 MCH Trauma. All rights reserved. FEMUR FRACTURE MANAGEMENT The pediatric Orthopedic Surgeon will assess your child in order to determine the optimal treatment method. Treatment goals include: achieving proper bone realignment, rapid healing, and the return to normal daily activities. The treatment method chosen is primarily based on the child’s age but also taken into consideration are: fracture type, location and other injuries sustained if applicable. Prior to the surgery, your child may be placed in skin traction. This will ensure the bone is in an optimal healing position until it is surgically repaired. Occasionally, traction may be used for a longer period of time. The surgeon will determine if this management is needed based on the specific fracture type and/or location. ELASTIC/FLEXIBLE INTRAMEDULLARY NAILING This surgery is performed by the Orthopedic Surgeon in the Operating Room under general anesthesia. The surgeon will usually make two small incisions near the knee joint in order to insert two flexible titanium rods (intramedullary nails) Flexible through the femur. -

Unilateral Proximal Focal Femoral Deficiency, Fibular Aplasia, Tibial
The Egyptian Journal of Medical Human Genetics (2014) 15, 299–303 Ain Shams University The Egyptian Journal of Medical Human Genetics www.ejmhg.eg.net www.sciencedirect.com CASE REPORT Unilateral proximal focal femoral deficiency, fibular aplasia, tibial campomelia and oligosyndactyly in an Egyptian child – Probable FFU syndrome Rabah M. Shawky a,*, Heba Salah Abd Elkhalek a, Shaimaa Gad a, Shaimaa Abdelsattar Mohammad b a Pediatric Department, Genetics Unit, Ain Shams University, Egypt b Radio Diagnosis Department, Ain Shams University, Egypt Received 2 March 2014; accepted 18 March 2014 Available online 30 April 2014 KEYWORDS Abstract We report a fifteen month old Egyptian male child, the third in order of birth of healthy Short femur; non consanguineous parents, who has normal mentality, normal upper limbs and left lower limb. Limb anomaly; The right lower limb has short femur, and tibia with anterior bowing, and an overlying skin dimple. FFU syndrome; The right foot has also oligosyndactyly (three toes), and the foot is in vulgus position. There is lim- Proximal focal femoral ited abduction at the hip joint, full flexion and extension at the knee, limited dorsiflexion and plan- deficiency; tar flexion at the ankle joint. The X-ray of the lower limb and pelvis shows proximal focal femoral Fibular aplasia; deficiency, absent right fibula with shortening of the right tibia and anterior bowing of its distal Tibial campomelia; third. The acetabulum is shallow. He has a family history of congenital cyanotic heart disease. Oligosyndactyly Our patient represents most probably the first case of femur fibula ulna syndrome (FFU) in Egypt with unilateral right leg affection. -

Lower Limb Venous Drainage
Vascular Anatomy of Lower Limb Dr. Gitanjali Khorwal Arteries of Lower Limb Medial and Lateral malleolar arteries Lower Limb Venous Drainage Superficial veins : Great Saphenous Vein and Short Saphenous Vein Deep veins: Tibial, Peroneal, Popliteal, Femoral veins Perforators: Blood flow deep veins in the sole superficial veins in the dorsum But In leg and thigh from superficial to deep veins. Factors helping venous return • Negative intra-thoracic pressure. • Transmitted pulsations from adjacent arteries. • Valves maintain uni-directional flow. • Valves in perforating veins prevent reflux into low pressure superficial veins. • Calf Pump—Peripheral Heart. • Vis-a –tergo produced by contraction of heart. • Suction action of diaphragm during inspiration. Dorsal venous arch of Foot • It lies in the subcutaneous tissue over the heads of metatarsals with convexity directed distally. • It is formed by union of 4 dorsal metatarsal veins. Each dorsal metatarsal vein recieves blood in the clefts from • dorsal digital veins. • and proximal and distal perforating veins conveying blood from plantar surface of sole. Great saphenous Vein Begins from the medial side of dorsal venous arch. Supplemented by medial marginal vein Ascends 2.5 cm anterior to medial malleolus. Passes posterior to medial border of patella. Ascends along medial thigh. Penetrates deep fascia of femoral triangle: Pierces the Cribriform fascia. Saphenous opening. Drains into femoral vein. superficial epigastric v. superficial circumflex iliac v. superficial ext. pudendal v. posteromedial vein anterolateral vein GREAT SAPHENOUS VEIN anterior leg vein posterior arch vein dorsal venous arch medial marginal vein Thoraco-epigastric vein Deep external pudendal v. Tributaries of Great Saphenous vein Tributaries of Great Saphenous vein saphenous opening superficial epigastric superficial circumflex iliac superficial external pudendal posteromedial vein anterolateral vein adductor c. -

Vessels in Femoral Triangle in a Rare Relationship Bandyopadhyay M, Biswas S, Roy R
Case Report Singapore Med J 2010; 51(1) : e3 Vessels in femoral triangle in a rare relationship Bandyopadhyay M, Biswas S, Roy R ABSTRACT vein, the longest superficial vein in the body, ends in the The femoral region of the thigh is utilised for femoral vein, which is a short distance away from the various clinical procedures, both open and inguinal ligament after passing through the saphenous closed, particularly in respect to arterial and opening.(2) venous cannulations. A rare vascular pattern was observed during the dissection of the femoral CASE REPORT region on both sides of the intact formaldehyde- A routine dissection in undergraduate teaching of an preserved cadaver of a 42-year-old Indian intact formaldehyde-preserved cadaver of a 42-year-old man from West Bengal. The relationships and Indian man from West Bengal revealed a rare pattern patterns found were contrary to the belief that of relationship between the femoral vessels on both the femoral vein is always medial to the artery, sides. The femoral artery crossed the femoral vein deep just below the inguinal ligament and the common to the inguinal ligament, such that the artery was lying femoral artery. The femoral artery crossed the superficial to the vein at the base of the femoral triangle. vein just deep to the inguinal ligament so that The profunda femoris artery was seen lying lateral, and the femoral vein was lying deep to the artery at the great saphenous vein medial, to the femoral vessels the base of the femoral triangle. Just deep to the in the triangle. -

Back of Leg I
Back of Leg I Dr. Garima Sehgal Associate Professor “Only those who risk going too far, can possibly find King George’s Medical University out how far one can go.” UP, Lucknow — T.S. Elliot DISCLAIMER Presentation has been made only for educational purpose Images and data used in the presentation have been taken from various textbooks and other online resources Author of the presentation claims no ownership for this material Learning Objectives By the end of this teaching session on Back of leg – I all the MBBS 1st year students must be able to: • Enumerate the contents of superficial fascia of back of leg • Write a short note on small saphenous vein • Describe cutaneous innervation in the back of leg • Write a short note on sural nerve • Enumerate the boundaries of posterior compartment of leg • Enumerate the fascial compartments in back of leg & their contents • Write a short note on flexor retinaculum of leg- its attachments & structures passing underneath • Describe the origin, insertion nerve supply and actions of superficial muscles of the posterior compartment of leg Introduction- Back of Leg / Calf • Powerful superficial antigravity muscles • (gastrocnemius, soleus) • Muscles are large in size • Inserted into the heel • Raise the heel during walking Superficial fascia of Back of leg • Contains superficial veins- • small saphenous vein with its tributaries • part of course of great saphenous vein • Cutaneous nerves in the back of leg- 1. Saphenous nerve 2. Posterior division of medial cutaneous nerve of thigh 3. Posterior cutaneous -

Anatomy of Abdominal Incisions
ANATOMY FOR THE MRCS but is time-consuming. A lower midline incision is needed for an Anatomy of abdominal emergency Caesarean section (where minutes may be crucial for baby and mother). The surgeon must also be sure of the pathol- incisions ogy before performing this approach. Close the Pfannenstiel and start again with a lower midline if the ‘pelvic mass’ proves to be Harold Ellis a carcinoma of the sigmoid colon! There are more than one dozen abdominal incisions quoted in surgical textbooks, but the ones in common use today (and which the candidate must know in detail) are discussed below. The midline incision (Figures 1–4) Opening the abdomen is the essential preliminary to the per- formance of a laparotomy. A correctly performed abdominal The midline abdominal incision has many advantages because it: exposure is based on sound anatomical knowledge, hence it is a • is very quick to perform common question in the Operative Surgery section of the MRCS • is relatively easy to close examination. • is virtually bloodless (no muscles are cut or nerves divided). • affords excellent access to the abdominal cavity and retroperi- toneal structures Incisions • can be extended from the xiphoid to the pubic symphysis. Essential features If closure is performed using the mass closure technique, pros- The surgeon needs ready and direct access to the organ requir- pective randomized clinical trials have shown no difference in ing investigation and treatment, so the incision must provide the incidence of wound dehiscence or incisional hernia com- sufficient room for the procedure to be performed. The incision pared with transverse or paramedian incisions.1 should (if possible): The upper midline incision is placed exactly in the midline • be capable of easy extension (to allow for any enlargement of and extends from the tip of the xiphoid to about 1 cm above the scope of the operation) the umbilicus. -

Clinical Anatomy of the Lower Extremity
Государственное бюджетное образовательное учреждение высшего профессионального образования «Иркутский государственный медицинский университет» Министерства здравоохранения Российской Федерации Department of Operative Surgery and Topographic Anatomy Clinical anatomy of the lower extremity Teaching aid Иркутск ИГМУ 2016 УДК [617.58 + 611.728](075.8) ББК 54.578.4я73. К 49 Recommended by faculty methodological council of medical department of SBEI HE ISMU The Ministry of Health of The Russian Federation as a training manual for independent work of foreign students from medical faculty, faculty of pediatrics, faculty of dentistry, protocol № 01.02.2016. Authors: G.I. Songolov - associate professor, Head of Department of Operative Surgery and Topographic Anatomy, PhD, MD SBEI HE ISMU The Ministry of Health of The Russian Federation. O. P.Galeeva - associate professor of Department of Operative Surgery and Topographic Anatomy, MD, PhD SBEI HE ISMU The Ministry of Health of The Russian Federation. A.A. Yudin - assistant of department of Operative Surgery and Topographic Anatomy SBEI HE ISMU The Ministry of Health of The Russian Federation. S. N. Redkov – assistant of department of Operative Surgery and Topographic Anatomy SBEI HE ISMU THE Ministry of Health of The Russian Federation. Reviewers: E.V. Gvildis - head of department of foreign languages with the course of the Latin and Russian as foreign languages of SBEI HE ISMU The Ministry of Health of The Russian Federation, PhD, L.V. Sorokina - associate Professor of Department of Anesthesiology and Reanimation at ISMU, PhD, MD Songolov G.I K49 Clinical anatomy of lower extremity: teaching aid / Songolov G.I, Galeeva O.P, Redkov S.N, Yudin, A.A.; State budget educational institution of higher education of the Ministry of Health and Social Development of the Russian Federation; "Irkutsk State Medical University" of the Ministry of Health and Social Development of the Russian Federation Irkutsk ISMU, 2016, 45 p. -

Anterior Abdominal Wall
Abdominal wall Borders of the Abdomen • Abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below • Borders Superior: Costal cartilages 7-12. Xiphoid process: • Inferior: Pubic bone and iliac crest: Level of L4. • Umbilicus: Level of IV disc L3-L4 Abdominal Quadrants Formed by two intersecting lines: Vertical & Horizontal Intersect at umbilicus. Quadrants: Upper left. Upper right. Lower left. Lower right Abdominal Regions Divided into 9 regions by two pairs of planes: 1- Vertical Planes: -Left and right lateral planes - Midclavicular planes -passes through the midpoint between the ant.sup.iliac spine and symphysis pupis 2- Horizontal Planes: -Subcostal plane - at level of L3 vertebra -Joins the lower end of costal cartilage on each side -Intertubercular plane: -- At the level of L5 vertebra - Through tubercles of iliac crests. Abdominal wall divided into:- Anterior abdominal wall Posterior abdominal wall What are the Layers of Anterior Skin Abdominal Wall Superficial Fascia - Above the umbilicus one layer - Below the umbilicus two layers . Camper's fascia - fatty superficial layer. Scarp's fascia - deep membranous layer. Deep fascia : . Thin layer of C.T covering the muscle may absent Muscular layer . External oblique muscle . Internal oblique muscle . Transverse abdominal muscle . Rectus abdominis Transversalis fascia Extraperitoneal fascia Parietal Peritoneum Superficial Fascia . Camper's fascia - fatty layer= dartos muscle in male . Scarpa's fascia - membranous layer. Attachment of scarpa’s fascia= membranous fascia INF: Fascia lata Sides: Pubic arch Post: Perineal body - Membranous layer in scrotum referred to as colle’s fascia - Rupture of penile urethra lead to extravasations of urine into(scrotum, perineum, penis &abdomen) Muscles .