EPI Coverage Assessment Survey
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Beautification and the Embodiment of Authenticity in Post-War Eastern Sri Lanka
University of Pennsylvania ScholarlyCommons Undergraduate Humanities Forum 2014-2015: Penn Humanities Forum Undergraduate Color Research Fellows 5-2015 Ornamenting Fingernails and Roads: Beautification and the Embodiment of Authenticity in Post-War Eastern Sri Lanka Kimberly Kolor University of Pennsylvania Follow this and additional works at: https://repository.upenn.edu/uhf_2015 Part of the Asian History Commons Kolor, Kimberly, "Ornamenting Fingernails and Roads: Beautification and the Embodiment of uthenticityA in Post-War Eastern Sri Lanka" (2015). Undergraduate Humanities Forum 2014-2015: Color. 7. https://repository.upenn.edu/uhf_2015/7 This paper was part of the 2014-2015 Penn Humanities Forum on Color. Find out more at http://www.phf.upenn.edu/annual-topics/color. This paper is posted at ScholarlyCommons. https://repository.upenn.edu/uhf_2015/7 For more information, please contact [email protected]. Ornamenting Fingernails and Roads: Beautification and the Embodiment of Authenticity in Post-War Eastern Sri Lanka Abstract In post-conflict Sri Lanka, communal tensions continue ot be negotiated, contested, and remade. Color codes virtually every aspect of daily life in salient local idioms. Scholars rarely focus on the lived visual semiotics of local, everyday exchanges from how women ornament their nails to how communities beautify their open—and sometimes contested—spaces. I draw on my ethnographic data from Eastern Sri Lanka and explore ‘color’ as negotiated through personal and public ornaments and notions of beauty with a material culture focus. I argue for a broad view of ‘public,’ which includes often marginalized and feminized public modalities. This view also explores how beauty and ornament are salient technologies of community and cultural authenticity that build on histories of ethnic imaginaries. -

CHAP 9 Sri Lanka
79o 00' 79o 30' 80o 00' 80o 30' 81o 00' 81o 30' 82o 00' Kankesanturai Point Pedro A I Karaitivu I. Jana D Peninsula N Kayts Jana SRI LANKA I Palk Strait National capital Ja na Elephant Pass Punkudutivu I. Lag Provincial capital oon Devipattinam Delft I. Town, village Palk Bay Kilinochchi Provincial boundary - Puthukkudiyiruppu Nanthi Kadal Main road Rameswaram Iranaitivu Is. Mullaittivu Secondary road Pamban I. Ferry Vellankulam Dhanushkodi Talaimannar Manjulam Nayaru Lagoon Railroad A da m' Airport s Bridge NORTHERN Nedunkeni 9o 00' Kokkilai Lagoon Mannar I. Mannar Puliyankulam Pulmoddai Madhu Road Bay of Bengal Gulf of Mannar Silavatturai Vavuniya Nilaveli Pankulam Kebitigollewa Trincomalee Horuwupotana r Bay Medawachchiya diya A d o o o 8 30' ru 8 30' v K i A Karaitivu I. ru Hamillewa n a Mutur Y Pomparippu Anuradhapura Kantalai n o NORTH CENTRAL Kalpitiya o g Maragahewa a Kathiraveli L Kal m a Oy a a l a t t Puttalam Kekirawa Habarane u 8o 00' P Galgamuwa 8o 00' NORTH Polonnaruwa Dambula Valachchenai Anamaduwa a y O Mundal Maho a Chenkaladi Lake r u WESTERN d Batticaloa Naula a M uru ed D Ganewatta a EASTERN g n Madura Oya a G Reservoir Chilaw i l Maha Oya o Kurunegala e o 7 30' w 7 30' Matale a Paddiruppu h Kuliyapitiya a CENTRAL M Kehelula Kalmunai Pannala Kandy Mahiyangana Uhana Randenigale ya Amparai a O a Mah Reservoir y Negombo Kegalla O Gal Tirrukkovil Negombo Victoria Falls Reservoir Bibile Senanayake Lagoon Gampaha Samudra Ja-Ela o a Nuwara Badulla o 7 00' ng 7 00' Kelan a Avissawella Eliya Colombo i G Sri Jayewardenepura -

Sri Lanka – Tamils – Eastern Province – Batticaloa – Colombo
Refugee Review Tribunal AUSTRALIA RRT RESEARCH RESPONSE Research Response Number: LKA34481 Country: Sri Lanka Date: 11 March 2009 Keywords: Sri Lanka – Tamils – Eastern Province – Batticaloa – Colombo – International Business Systems Institute – Education system – Sri Lankan Army-Liberation Tigers of Tamil Eelam conflict – Risk of arrest This response was prepared by the Research & Information Services Section of the Refugee Review Tribunal (RRT) after researching publicly accessible information currently available to the RRT within time constraints. This response is not, and does not purport to be, conclusive as to the merit of any particular claim to refugee status or asylum. This research response may not, under any circumstance, be cited in a decision or any other document. Anyone wishing to use this information may only cite the primary source material contained herein. Questions 1. Please provide information on the International Business Systems Institute in Kaluvanchikkudy. 2. Is it likely that someone would attain a high school or higher education qualification in Sri Lanka without learning a language other than Tamil? 3. Please provide an overview/timeline of relevant events in the Eastern Province of Sri Lanka from 1986 to 2004, with particular reference to the Sri Lankan Army (SLA)-Liberation Tigers of Tamil Eelam (LTTE) conflict. 4. What is the current situation and risk of arrest for male Tamils in Batticaloa and Colombo? RESPONSE 1. Please provide information on the International Business Systems Institute in Kaluvanchikkudy. Note: Kaluvanchikkudy is also transliterated as Kaluwanchikudy is some sources. No references could be located to the International Business Systems Institute in Kaluvanchikkudy. The Education Guide Sri Lanka website maintains a list of the “Training Institutes Registered under the Ministry of Skills Development, Vocational and Tertiary Education”, and among these is ‘International Business System Overseas (Pvt) Ltd’ (IBS). -
Update UNHCR/CDR Background Paper on Sri Lanka
NATIONS UNIES UNITED NATIONS HAUT COMMISSARIAT HIGH COMMISSIONER POUR LES REFUGIES FOR REFUGEES BACKGROUND PAPER ON REFUGEES AND ASYLUM SEEKERS FROM Sri Lanka UNHCR CENTRE FOR DOCUMENTATION AND RESEARCH GENEVA, JUNE 2001 THIS INFORMATION PAPER WAS PREPARED IN THE COUNTRY RESEARCH AND ANALYSIS UNIT OF UNHCR’S CENTRE FOR DOCUMENTATION AND RESEARCH ON THE BASIS OF PUBLICLY AVAILABLE INFORMATION, ANALYSIS AND COMMENT, IN COLLABORATION WITH THE UNHCR STATISTICAL UNIT. ALL SOURCES ARE CITED. THIS PAPER IS NOT, AND DOES NOT, PURPORT TO BE, FULLY EXHAUSTIVE WITH REGARD TO CONDITIONS IN THE COUNTRY SURVEYED, OR CONCLUSIVE AS TO THE MERITS OF ANY PARTICULAR CLAIM TO REFUGEE STATUS OR ASYLUM. ISSN 1020-8410 Table of Contents LIST OF ACRONYMS.............................................................................................................................. 3 1 INTRODUCTION........................................................................................................................... 4 2 MAJOR POLITICAL DEVELOPMENTS IN SRI LANKA SINCE MARCH 1999................ 7 3 LEGAL CONTEXT...................................................................................................................... 17 3.1 International Legal Context ................................................................................................. 17 3.2 National Legal Context........................................................................................................ 19 4 REVIEW OF THE HUMAN RIGHTS SITUATION............................................................... -

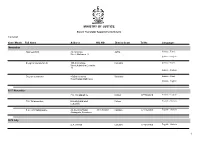
Divisional Secretariats Contact Details
Divisional Secretariats Contact Details District Divisional Secretariat Divisional Secretary Assistant Divisional Secretary Life Location Telephone Mobile Code Name E-mail Address Telephone Fax Name Telephone Mobile Number Name Number 5-2 Ampara Ampara Addalaichenai [email protected] Addalaichenai 0672277336 0672279213 J Liyakath Ali 0672055336 0778512717 0672277452 Mr.MAC.Ahamed Naseel 0779805066 Ampara Ampara [email protected] Divisional Secretariat, Dammarathana Road,Indrasarapura,Ampara 0632223435 0632223004 Mr.H.S.N. De Z.Siriwardana 0632223495 0718010121 063-2222351 Vacant Vacant Ampara Sammanthurai [email protected] Sammanthurai 0672260236 0672261124 Mr. S.L.M. Hanifa 0672260236 0716829843 0672260293 Mr.MM.Aseek 0777123453 Ampara Kalmunai (South) [email protected] Divisional Secretariat, Kalmunai 0672229236 0672229380 Mr.M.M.Nazeer 0672229236 0772710361 0672224430 Vacant - Ampara Padiyathalawa [email protected] Divisional Secretariat Padiyathalawa 0632246035 0632246190 R.M.N.Wijayathunga 0632246045 0718480734 0632050856 W.Wimansa Senewirathna 0712508960 Ampara Sainthamarathu [email protected] Main Street Sainthamaruthu 0672221890 0672221890 Mr. I.M.Rikas 0752800852 0672056490 I.M Rikas 0777994493 Ampara Dehiattakandiya [email protected] Divisional Secretariat, Dehiattakandiya. 027-2250167 027-2250197 Mr.R.M.N.C.Hemakumara 027-2250177 0701287125 027-2250081 Mr.S.Partheepan 0714314324 Ampara Navithanvelly [email protected] Divisional secretariat, Navithanveli, Amparai 0672224580 0672223256 MR S.RANGANATHAN 0672223256 0776701027 0672056885 MR N.NAVANEETHARAJAH 0777065410 0718430744/0 Ampara Akkaraipattu [email protected] Main Street, Divisional Secretariat- Akkaraipattu 067 22 77 380 067 22 800 41 M.S.Mohmaed Razzan 067 2277236 765527050 - Mrs. A.K. Roshin Thaj 774659595 Ampara Ninthavur Nintavur Main Street, Nintavur 0672250036 0672250036 Mr. T.M.M. -
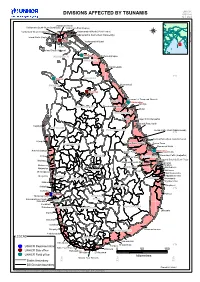
DIVISIONS AFFECTED by TSUNAMIS GIS Unit Sri Lanka
UNHCR DIVISIONS AFFECTED BY TSUNAMIS GIS Unit Sri Lanka ValikamamValikamam NorthNorth ValikamamValikamam South-WestSouth-West (Sandilipay)(Sandilipay) ValikamamValikamam EastEast (Kopay)(Kopay) Valikamam West (Chankanai) VadamaradchiVadamaradchi NorthNorth (Point(Point Perdro)Perdro) JAFFNAJAFFNA VadamaradchiVadamaradchi South-WestSouth-West (Karaveddy)(Karaveddy) Island North (Kayts) JaffnaJaffna VadamaradchiVadamaradchi EastEast Divisions.WOR Affected Jaffna DelftDelft DelftDelftIsland South (Velanai) KillinochchiKillinochchi KILINOCHCHIKILINOCHCHI KillinochchiKillinochchi PuthukudiyiruppuPuthukudiyiruppu MULLAITIVUMULLAITIVU MaritimepattuMaritimepattu 9°N MannarMannar VAVUNIYAVAVUNIYA MANNARMANNAR KuchchaveliKuchchaveli VavuniyaVavuniya TrincomaleeTrincomalee TownTown andand GravetsGravets MorawewaMorawewa TrincomaleeTrincomalee KinniyaKinniya ANURADHAPURAANURADHAPURA ThambalagamuwaThambalagamuwa MutturMuttur TRINCOMALEETRINCOMALEE SeruvilaSeruvila Verugal/Verugal/ EchchilampattaiEchchilampattai KoralaiKoralai PattuPattu NorthNorth KalpitiyaKalpitiya PUTTALAMPUTTALAM POLONNARUWAPOLONNARUWA KoralaiKoralai PattuPattu WestWest (Oddamavadi)(Oddamavadi) 8°N KoralaiKoralai PattuPattu WestWest (Valachchenai)(Valachchenai) MundelMundel KoralaiKoralai PattuPattu (South)(South) EravurEravur TownTown KURUNEGALAKURUNEGALA KoralaiKoralai PattuPattu (South)(South) EravurEravur TownTown ManmunaiManmunai NorthNorth ArachchikattuwaArachchikattuwa BatticaloaBatticaloa EravurEravur PattuPattu BatticaloaBatticaloaKattankudyKattankudy ManmunaiManmunai -
Name List of Sworn Translators in Sri Lanka
MINISTRY OF JUSTICE Sworn Translator Appointments Details 1/29/2021 Year / Month Full Name Address NIC NO District Court Tel No Languages November Rasheed.H.M. 76,1st Cross Jaffna Sinhala - Tamil Street,Ninthavur 12 Sinhala - English Sivagnanasundaram.S. 109,4/2,Collage Colombo Sinhala - Tamil Street,Kotahena,Colombo 13 Sinhala - English Dreyton senaratna 45,Old kalmunai Baticaloa Sinhala - Tamil Road,Kalladi,Batticaloa Sinhala - English 1977 November P.M. Thilakarathne Chilaw 0777892610 Sinhala - English P.M. Thilakarathne kirimathiyana East, Chilaw English - Sinhala Lunuwilla. S.D. Cyril Sadanayake 26, De silva Road, 331490350V Kalutara 0771926906 English - Sinhala Atabagoda, Panadura 1979 July D.A. vincent Colombo 0776738956 English - Sinhala 1 1/29/2021 Year / Month Full Name Address NIC NO District Court Tel No Languages 1992 July H.M.D.A. Herath 28, Kolawatta, veyangda 391842205V Gampaha 0332233032 Sinhala - English 2000 June W.A. Somaratna 12, sanasa Square, Gampaha 0332224351 English - Sinhala Gampaha 2004 July kalaichelvi Niranjan 465/1/2, Havelock Road, Colombo English - Tamil Colombo 06 2008 May saroja indrani weeratunga 1E9 ,Jayawardanagama, colombo English - battaramulla Sinhala - 2008 September Saroja Indrani Weeratunga 1/E/9, Jayawadanagama, Colombo Sinhala - English Battaramulla 2011 July P. Maheswaran 41/B, Ammankovil Road, Kalmunai English - Sinhala Kalmunai -2 Tamil - K.O. Nanda Karunanayake 65/2, Church Road, Gampaha 0718433122 Sinhala - English Gampaha 2011 November J.D. Gunarathna "Shantha", Kalutara 0771887585 Sinhala - English Kandawatta,Mulatiyana, Agalawatta. 2 1/29/2021 Year / Month Full Name Address NIC NO District Court Tel No Languages 2012 January B.P. Eranga Nadeshani Maheshika 35, Sri madhananda 855162954V Panadura 0773188790 English - French Mawatha, Panadura 0773188790 Sinhala - 2013 Khan.C.M.S. -

Integrated Strategic Environmental Assessment of the Northern Province of Sri Lanka Report
Integrated Strategic Environmental Assessment of the Northern Province of Sri Lanka A multi-agency approach coordinated by Central Environment Authority and Disaster Management Centre, Supported by United Nations Development Programme and United Nations Environment Programme Integrated Strategic Environmental Assessment of the Northern Province of Sri Lanka November 2014 A Multi-agency approach coordinated by the Central Environmental Authority (CEA) of the Ministry of Environment and Renewable Energy and Disaster Management Centre (DMC) of the Ministry of Disaster Management, supported by United Nations Development Programme (UNDP) and United Nations Environment Programme (UNEP) Integrated Strategic Environment Assessment of the Northern Province of Sri Lanka ISBN number: 978-955-9012-55-9 First edition: November 2014 © Editors: Dr. Ananda Mallawatantri Prof. Buddhi Marambe Dr. Connor Skehan Published by: Central Environment Authority 104, Parisara Piyasa, Battaramulla Sri Lanka Disaster Management Centre No 2, Vidya Mawatha, Colombo 7 Sri Lanka Related publication: Map Atlas: ISEA-North ii Message from the Hon. Minister of Environment and Renewable Energy Strategic Environmental Assessment (SEA) is a systematic decision support process, aiming to ensure that due consideration is given to environmental and other sustainability aspects during the development of plans, policies and programmes. SEA is widely used in many countries as an aid to strategic decision making. In May 2006, the Cabinet of Ministers approved a Cabinet of Memorandum -

Tides of Violence: Mapping the Sri Lankan Conflict from 1983 to 2009 About the Public Interest Advocacy Centre
Tides of violence: mapping the Sri Lankan conflict from 1983 to 2009 About the Public Interest Advocacy Centre The Public Interest Advocacy Centre (PIAC) is an independent, non-profit legal centre based in Sydney. Established in 1982, PIAC tackles barriers to justice and fairness experienced by people who are vulnerable or facing disadvantage. We ensure basic rights are enjoyed across the community through legal assistance and strategic litigation, public policy development, communication and training. 2nd edition May 2019 Contact: Public Interest Advocacy Centre Level 5, 175 Liverpool St Sydney NSW 2000 Website: www.piac.asn.au Public Interest Advocacy Centre @PIACnews The Public Interest Advocacy Centre office is located on the land of the Gadigal of the Eora Nation. TIDES OF VIOLENCE: MAPPING THE SRI LANKAN CONFLICT FROM 1983 TO 2009 03 EXECUTIVE SUMMARY ....................................................................................................................... 09 Background to CMAP .............................................................................................................................................09 Report overview .......................................................................................................................................................09 Key violation patterns in each time period ......................................................................................................09 24 July 1983 – 28 July 1987 .................................................................................................................................10 -

Sri Lanka –Eastern Province – Trincomalee – Security Situation – Human Rights – Military and Paramilitary Groups – TMVP – Tamils with LTTE Links – Kiliveddy - Muthur
Refugee Review Tribunal AUSTRALIA RRT RESEARCH RESPONSE Research Response Number: LKA35265 Country: Sri Lanka Date: 5 August 2009 Keywords: – Sri Lanka –Eastern Province – Trincomalee – Security situation – Human Rights – Military and paramilitary groups – TMVP – Tamils with LTTE Links – Kiliveddy - Muthur This response was prepared by the Research & Information Services Section of the Refugee Review Tribunal (RRT) after researching publicly accessible information currently available to the RRT within time constraints. This response is not, and does not purport to be, conclusive as to the merit of any particular claim to refugee status or asylum. This research response may not, under any circumstance, be cited in a decision or any other document. Anyone wishing to use this information may only cite the primary source material contained herein. Questions 1. Please provide an update of the security situation in the East of Sri Lanka, particularly Trincomalee. 2. Is there a large military presence in Trincomalee? Are there reports of human rights abuses by the military in the east? 3. Do paramilitary groups/pro-government militias (such as those previously headed by Karuna and/or Pilliyan) still operate in Trincomalee? Are they still a threat to Tamils who are suspected of having LTTE links? 4. Is there any evidence of a town called Kiliveddy Muthur Trincomalee? Prior to the Sri Lankan government claiming victory over the LTTE, was Kiliveddy controlled by the LTTE or the government? RESPONSE 1. Please provide an update of the security situation in the East of Sri Lanka, particularly Trincomalee. The response to this question has been divided into two sections, the first dealing specifically with security in Trincomalee and the second relating more generally to the security situation in the Eastern Province of Sri Lanka. -

Jaffna District – 2007
BASIC POPULATION INFORMATION ON JAFFNA DISTRICT – 2007 Preliminary Report Based on Special Enumeration – 2007 Department of Census and Statistics June 2008 Foreword The Department of Census and Statistics (DCS), carried out a special enumeration in Eastern province and in Jaffna district in Northern province. The objective of this enumeration is to provide the necessary basic information needed to formulate development programmes and relief activities for the people. This preliminary publication for Jaffna district has been compiled from the reports obtained from the District based on summaries prepared by enumerators and supervisors. A final detailed publication will be disseminated after the computer processing of questionnaires. This preliminary release gives some basic information for Jaffna district, such as population by divisional secretary’s division, urban/rural population, sex, age (under 18 years and 18 years and over) and ethnicity. Data on displaced persons due to conflict or tsunami are also included. Some important information which is useful for regional level planning purposes are given by Grama Niladhari Divisions. This enumeration is based on the usual residents of households in the district. These figures should be regarded as provisional. I wish to express my sincere thanks to the staff of the department and all other government officials and others who worked with dedication and diligence for the successful completion of the enumeration. I am also grateful to the general public for extending their fullest co‐operation in this important undertaking. This publication has been prepared by Population Census Division of this Department. D.B.P. Suranjana Vidyaratne Director General of Census and Statistics 6th June 2008 Department of Census and Statistics, 15/12, Maitland Crescent, Colombo 7. -
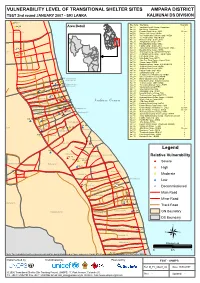
VULNERABILITY LEVEL of TRANSITIONAL SHELTER SITES AMPARA DISTRICT TSST 2Nd Round JANUARY 2007 - SRI LANKA KALMUNAI DS DIVISION
VULNERABILITY LEVEL OF TRANSITIONAL SHELTER SITES AMPARA DISTRICT TSST 2nd round JANUARY 2007 - SRI LANKA KALMUNAI DS DIVISION *#Kal_16 Site Code Site Name Total Vul. Kal_02 *# Area Detail Kal_01 Varathan RiceMill Camp - Samaritans 1 Kal_02 Bar Camp - Samaritan 1 Periyaneelavanai 01B Kal_04 Ponniah Road Camp - WDC Decom Kal_06 Vishnu Kovil Camp - NHDA 1 Kal_07 VC Road Muslim Division Camp - NHDA 1 Kal_08 V.C.Road Camp - WDC/NHDA 1 Kal_12 Moossa Camp - Sewa Lanka 2 Kal_15 Sanganthurai Camp - JVP 1 Kal_16 Masjidul Aqbar Camp - WDC 1 Kal_17 Hudha Camp - Sewa Lanka 1 Kal_04 Kal_18 Aqbar Jummah Mosque Road Camp - WDC 3 0* Kal_19 Masjidul Aqbar Camp - NHDA 2 ai 01A Kal_20 S.M.Road Camp - UNHCR/EHED/FCE 2 *#Kal_01 Kal_21 Al-Manar Central Camp - FORUT/WDC 1 Kal_22 Hijra Road Camp - JVP 2 Kal_23 Hijra Road Camp -MFCD 2 Kal_24 Sam Sum Road Camp - Islamic Relief 1 Kal_25 Shums Camp - EHED 2 Kal_26 Maqbooliya Lane Camp - EHED/UNHCR 2 Kal_27 Al-Minah Road Camp - NHDA 1 Kal_28 Al-Minan Road Camp - WDC 1 Kal_30 Hajiyar Road Camp - WDC 1 Kal_31 Sahanthura Camp - JVP 2 Kal_33 Sellappa Cross Road Camp - EHED 1 Kal_34 Valluvar(AI-Minan Camp)-EHED 2 Kal_17 Kal_12 Periyaneelavanai Kal_35 Maha Vidyalaya Camp - EHED 2 *# Muslim Sec.02 Kal_07 *# Kal_37 Khali Kovil Camp - NHDA/Sevalanka 2 *# *# *# Kal_38 Thathan Camp - MSF / EHED 1 Kal_06 Periyaneelavanai Kal_39 Thiroufathy Amman Camp - EHED 1 Kal_08 Muslim Sec.01 Kal_68 Kal_40 Vipulananda Camp-EHED 1 Periyaneelavanai 02 Kal_69 Kal_20 Kal_41 Visuvasikal Illam Camp 1 *# Kal_15 *# Kal_19 *# Kal_27*# *# *# Kal_43