How to Document Wounds and Bruises
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Skin Injuries – Can We Determine Timing and Mechanism?
Skin injuries – can we determine timing and mechanism? Jo Tully VFPMS Seminar 2016 What skin injuries do we need to consider? • Bruising • Commonest accidental and inflicted skin injury • Basic principles that can be applied when formulating opinion • Abrasions • Lacerations }we need to be able to tell the difference • Incisions • Stabs/chops • Bite marks – animal v human / inflicted v ‘accidental’ v self-inflicted Our role…. We are often/usually/always asked…………….. • “What type of injury is it?” • “When did this injury occur?” • “How did this injury occur?” • “Was this injury inflicted or accidental?” • IS THIS CHILD ABUSE? • To be able to answer these questions (if we can) we need knowledge of • Anatomy/physiology/healing - injury interpretation • Forces • Mechanisms in relation to development, plausibility • Current evidence Bruising – can we really tell which bruises are caused by abuse? Definitions – bruising • BLUNT FORCE TRAUMA • Bruise =bleeding beneath intact skin due to BFT • Contusion = bruise in deeper tissues • Haematoma - extravasated blood filling a cavity (or potential space). Usually associated with swelling • Petechiae =Pinpoint sized (0.1-2mm) hemorrhages into the skin due to acute rise in venous pressure • medical causes • direct forces • indirect forces Medical Direct Indirect causes mechanical mechanical forces forces Factors affecting development and appearance of a bruise • Properties of impacting object or surface • Force of impact • Duration of impact • Site - properties of body region impacted (blood supply, -
Immune Thrombocytopenia Purpura (ITP)
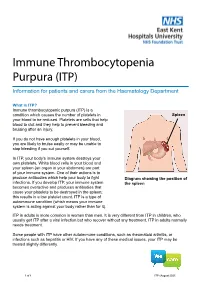
Immune Thrombocytopenia Purpura (ITP) Information for patients and carers from the Haematology Department What is ITP? Immune thrombocytopenic purpura (ITP) is a condition which causes the number of platelets in Spleen your blood to be reduced. Platelets are cells that help blood to clot and they help to prevent bleeding and bruising after an injury. If you do not have enough platelets in your blood, you are likely to bruise easily or may be unable to stop bleeding if you cut yourself. In ITP, your body’s immune system destroys your own platelets. White blood cells in your blood and your spleen (an organ in your abdomen) are part of your immune system. One of their actions is to produce antibodies which help your body to fight Diagram showing the position of infections. If you develop ITP, your immune system the spleen becomes overactive and produces antibodies that cause your platelets to be destroyed in the spleen; this results in a low platelet count. ITP is a type of autoimmune condition (which means your immune system is acting against your body rather than for it). ITP in adults is more common in women than men. It is very different from ITP in children, who usually get ITP after a viral infection but who recover without any treatment. ITP in adults normally needs treatment. Some people with ITP have other autoimmune conditions, such as rheumatoid arthritis, or infections such as hepatitis or HIV. If you have any of these medical issues, your ITP may be treated slightly differently. 1 of 8 ITP (August 2021) A normal platelet count is between 150 and 400 thousand million platelets per litre of blood. -

Wound Classification
Wound Classification Presented by Dr. Karen Zulkowski, D.N.S., RN Montana State University Welcome! Thank you for joining this webinar about how to assess and measure a wound. 2 A Little About Myself… • Associate professor at Montana State University • Executive editor of the Journal of the World Council of Enterstomal Therapists (JWCET) and WCET International Ostomy Guidelines (2014) • Editorial board member of Ostomy Wound Management and Advances in Skin and Wound Care • Legal consultant • Former NPUAP board member 3 Today We Will Talk About • How to assess a wound • How to measure a wound Please make a note of your questions. Your Quality Improvement (QI) Specialists will follow up with you after this webinar to address them. 4 Assessing and Measuring Wounds • You completed a skin assessment and found a wound. • Now you need to determine what type of wound you found. • If it is a pressure ulcer, you need to determine the stage. 5 Assessing and Measuring Wounds This is important because— • Each type of wound has a different etiology. • Treatment may be very different. However— • Not all wounds are clear cut. • The cause may be multifactoral. 6 Types of Wounds • Vascular (arterial, venous, and mixed) • Neuropathic (diabetic) • Moisture-associated dermatitis • Skin tear • Pressure ulcer 7 Mixed Etiologies Many wounds have mixed etiologies. • There may be both venous and arterial insufficiency. • There may be diabetes and pressure characteristics. 8 Moisture-Associated Skin Damage • Also called perineal dermatitis, diaper rash, incontinence-associated dermatitis (often confused with pressure ulcers) • An inflammation of the skin in the perineal area, on and between the buttocks, into the skin folds, and down the inner thighs • Scaling of the skin with papule and vesicle formation: – These may open, with “weeping” of the skin, which exacerbates skin damage. -

Gunshot Wounds
Gunshot Wounds Michael Sirkin, MD Chief, Orthopaedic Trauma Service Assistant Professor, New Jersey Medical School North Jersey Orthopaedic Institute Created March 2004; Reviewed March 2006, August 2010 Ballistics • Most bullets made of lead alloy – High specific gravity • Maximal mass • Less effect of air resistance • Bullet tips – Pointed – Round – Flat – Hollow Ballistics • Low velocity bullets – Made of low melting point lead alloys – If fired from high velocity they melt, 2° to friction • Deform • Change missile ballistics • High velocity bullets – Coated or jacketed with a harder metal – High temperature coating – Less deformity when fired Velocity • Energy = ½ mv2 • Energy increases by the square of the velocity and linearly with the mass • Velocity of missile is the most important factor determining amount of energy and subsequent tissue damage Kinetic Energy of High and Low Velocity Firearms Kinetic Energy of Shotgun Shells Wounding power • Low velocity, less severe – Less than 1000 ft/sec – Less than 230 grams • High velocity, very destructive – Greater than 2000 ft/sec – Weight less than 150 grams • Shotguns, very destructive at close range – About 1200 ft/sec – Weight up to 870 grams Factors that cause tissue damage • Crush and laceration • Secondary missiles • Cavitation • Shock wave Crush and Laceration • Principle mechanism in low velocity gunshot wounds • Material in path is crushed or lacerated • The kinetic energy is dissipated • Increased tissue damage with yaw or tumble – Increased profile – Increased rate of kinetic -

Pressure Ulcer Staging Cards and Skin Inspection Opportunities.Indd
Pressure Ulcer Staging Pressure Ulcer Staging Suspected Deep Tissue Injury (sDTI): Purple or maroon localized area of discolored Suspected Deep Tissue Injury (sDTI): Purple or maroon localized area of discolored intact skin or blood-fi lled blister due to damage of underlying soft tissue from pressure intact skin or blood-fi lled blister due to damage of underlying soft tissue from pressure and/or shear. The area may be preceded by tissue that is painful, fi rm, mushy, boggy, and/or shear. The area may be preceded by tissue that is painful, fi rm, mushy, boggy, warmer or cooler as compared to adjacent tissue. warmer or cooler as compared to adjacent tissue. Stage 1: Intact skin with non- Stage 1: Intact skin with non- blanchable redness of a localized blanchable redness of a localized area usually over a bony prominence. area usually over a bony prominence. Darkly pigmented skin may not have Darkly pigmented skin may not have visible blanching; its color may differ visible blanching; its color may differ from surrounding area. from surrounding area. Stage 2: Partial thickness loss of Stage 2: Partial thickness loss of dermis presenting as a shallow open dermis presenting as a shallow open ulcer with a red pink wound bed, ulcer with a red pink wound bed, without slough. May also present as without slough. May also present as an intact or open/ruptured serum- an intact or open/ruptured serum- fi lled blister. fi lled blister. Stage 3: Full thickness tissue loss. Stage 3: Full thickness tissue loss. Subcutaneous fat may be visible but Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. -

Penetrating Injury to the Head: Case Reviews K Regunath, S Awang*, S B Siti, M R Premananda, W M Tan, R H Haron**
CASE REPORT Penetrating Injury to the Head: Case Reviews K Regunath, S Awang*, S B Siti, M R Premananda, W M Tan, R H Haron** *Department of Neurosciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, **Department of Neurosurgery, Hospital Kuala Lumpur the right frontal lobe to a depth of approximately 2.5cm. SUMMARY (Figure 1: A & B) There was no obvious intracranial Penetrating injury to the head is considered a form of severe haemorrhage along the track of injury. The patient was taken traumatic brain injury. Although uncommon, most to the operating theatre and was put under general neurosurgical centres would have experienced treating anaesthesia. The nail was cut proximal to the entry wound patients with such an injury. Despite the presence of well and the piece of wood removed. The entry wound was found written guidelines for managing these cases, surgical to be contaminated with hair and debris. The nail was also treatment requires an individualized approach tailored to rusty. A bicoronal skin incision was fashioned centred on the the situation at hand. We describe a collection of three cases entry wound. A bifrontal craniotomy was fashioned and the of non-missile penetrating head injury which were managed bone flap removed sparing a small island of bone around the in two main Neurosurgical centres within Malaysia and the nail (Figure 1: C&D). Bilateral “U” shaped dural incisions unique management approaches for each of these cases. were made with the base to the midline. The nail was found to have penetrated with dura about 0.5cm from the edge of KEY WORDS: Penetrating head injury, nail related injury, atypical penetrating the sagittal sinus. -

Bleeds and Bruises in Children with Haemophilia
Bleeds and Bruises in CHildren WiTH HaeMOPHilia MusCle ANd/or JoiNt Bleeds Call the parent/guardian P.r.i.C.e. siGNs oF A serious HeAd Bleed P : Protection * Headache. Lower Limb: Take weight off the joint or muscle * drowsiness. Upper Limb: No carrying using affected arm * Nausea. r : rest * Vomiting. • Rest means rest! * unsteady Balance. • Try not to allow use of the joint or muscle where * irritability. possible. * Confusion. * seizures. i : ice * loss of consciousness. • Regular ice packs can help with pain & reduce swelling. • Put an ice pack over the affected area for 20 minutes. Repeat every two hours. DO NOT leave the ice pack on for more than 20 minutes siGNs oF A soFt tissue DO NOT place ice pack directly on skin (Use a tea Bleed towel/cold pack cover) * Bruising, discolouring of skin. C : Compression * Mild swelling. • Use an elasticated bandage to compress the affected area to reduce swelling. e : elevation • Elevate the affected limb to help reduce swelling. siGNs oF AN ABdoMiNAl • Keep the affected joint or muscle above the level of the Bleed heart. * Bloody, black or tar-like First Aid bowel motions. * red or brown urine. Mouth & Gum Bleeds * Pain. These can be hard to control because clots that form are * Vomiting of blood (blood washed away by saliva or knocked off by the tongue or food. Try giving the child an ice cube or ice pop to suck. may be red or black). These bleeds may need treatment by parents or the treatment centre. Nosebleeds siGNs oF BleediNG iNto tHe Tilt head forward and pinch the bridge of the nose below the bone for 10 - 20 minutes and / or put an ice-pack on JoiNts or MusCles the bridge of the nose for not more than 5 minutes. -

Isolated Plantar Vein Thrombosis Resembling a Corn with a Bruise
JE Hahm, et al pISSN 1013-9087ㆍeISSN 2005-3894 Ann Dermatol Vol. 31, No. 1, 2019 https://doi.org/10.5021/ad.2019.31.1.66 CASE REPORT Isolated Plantar Vein Thrombosis Resembling a Corn with a Bruise Ji Eun Hahm, Kang Su Kim, Jae Won Ha, Chul Woo Kim, Sang Seok Kim Department of Dermatology, Kangdong Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea Plantar vein thrombosis, rarely-reported disease, is usually or callus, plantar fibromatosis, or plantar verruca1. Among accompanied by pain and tenderness in the plantar region laborers, they may develop from excess pressure on the and should be differentiated from other dermatological con- bony prominences of the feet, repetitive uneven friction ditions causing plantar pain, such as hemorrhagic corn/cal- from footwear, or gait abnormalities. Plantar vein throm- lus, plantar epidermal cyst, verruca, or plantar fibromatosis. bosis is a rare condition causing plantar pain. The exact A 52-year-old man presented with a violaceous tender sub- cause of plantar vein thrombosis is yet unclear, but predis- cutaneous nodule overlying a hyperkeratotic plaque on his posing conditions, such as prior trauma, surgery, paraneo- sole. Initially, he thought it was a corn and applied keratolytic plastic syndromes, or coagulation disorders have been agents, which failed to work. Sonography revealed a well-de- described. To date, there is no established treatment ex- marcated mass with increased peripheral vascularity. His cept surgical excision, but reportedly, nonsteroidal anti-in- pain was relieved after a complete wide excision, which con- flammatory drug or heparin with elastic bandage is known firmed the mass to be plantar vein thrombosis after histo- to be effective for symptomatic control2-5. -

What Everyone Should Know to Stop Bleeding After an Injury
What Everyone Should Know to Stop Bleeding After an Injury THE HARTFORD CONSENSUS The Joint Committee to Increase Survival from Active Shooter and Intentional Mass Casualty Events was convened by the American College of Surgeons in response to the growing number and severity of these events. The committee met in Hartford Connecticut and has produced a number of documents with rec- ommendations. The documents represent the consensus opinion of a multi-dis- ciplinary committee involving medical groups, the military, the National Security Council, Homeland Security, the FBI, law enforcement, fire rescue, and EMS. These recommendations have become known as the Hartford Consensus. The overarching principle of the Hartford Consensus is that no one should die from uncontrolled bleeding. The Hartford Consensus recommends that all citizens learn to stop bleeding. Further information about the Hartford Consensus and bleeding control can be found on the website: Bleedingcontrol.org 2 SAVE A LIFE: What Everyone Should Know to Stop Bleeding After an Injury Authors: Peter T. Pons, MD, FACEP Lenworth Jacobs, MD, MPH, FACS Acknowledgements: The authors acknowledge the contributions of Michael Cohen and James “Brooks” Hart, CMI to the design of this manual. Some images adapted from Adam Wehrle, EMT-P and NAEMT. © 2017 American College of Surgeons CONTENTS SECTION 1 3 ■ Introduction ■ Primary Principles of Trauma Care Response ■ The ABCs of Bleeding SECTION 2 5 ■ Ensure Your Own Safety SECTION 3 6 ■ A – Alert – call 9-1-1 SECTION 4 7 ■ B – Bleeding – find the bleeding injury SECTION 5 9 ■ C – Compress – apply pressure to stop the bleeding by: ■ Covering the wound with a clean cloth and applying pressure by pushing directly on it with both hands, OR ■Using a tourniquet, OR ■ Packing (stuff) the wound with gauze or a clean cloth and then applying pressure with both hands SECTION 6 13 ■ Summary 2 SECTION 1: INTRODUCTION Welcome to the Stop the Bleed: Bleeding Control for the Injured information booklet. -
Wound Care: the Basics
Wound Care: The Basics Suzann Williams-Rosenthal, RN, MSN, WOC, GNP Norma Branham, RN, MSN, WOC, GNP University of Virginia May, 2010 What Type of Wound is it? How long has it been there? Acute-generally heal in a couple weeks, but can become chronic: Surgical Trauma Chronic -do not heal by normal repair process-takes weeks to months: Vascular-venous stasis, arterial ulcers Pressure ulcers Diabetic foot ulcers (neuropathic) Chronic Wounds Pressure Ulcer Staging Where is it? Where is it located? Use anatomical location-heel, ankle, sacrum, coccyx, etc. Measurements-in centimeters Length X Width X Depth • Length = greatest length (head to toe) • Width = greatest width (side to side) • Depth = measure by marking the depth with a Q- Tip and then hold to a ruler Wound Characteristics: Describe by percentage of each type of tissue: Granulation tissue: • red, cobblestone appearance (healing, filling in) Necrotic: • Slough-yellow, tan dead tissue (devitalized) • Eschar-black/brown necrotic tissue, can be hard or soft Evaluating additional tissue damage: Undermining Separation of tissue from the surface under the edge of the wound • Describe by clock face with patients head at 12 (“undermining is 1 cm from 12 to 4 o’clock”) Tunneling Channel that runs from the wound edge through to other tissue • “tunneling at 9 o’clock, measuring 3 cm long” Wound Drainage and Odor Exudate Fluid from wound • Document the amount, type and odor • Light, moderate, heavy • Drainage can be clear, sanguineous (bloody), serosanguineous (blood-tinged), -

Understanding Haemophilia
Understanding haemophilia Understanding haemophilia Contents Introduction 3 Haemophilia and your child 4 What is haemophilia? 5 What causes haemophilia? 5 Can females have haemophilia? 6 Carriers 8 Who is affected by haemophilia? 9 How severe is haemophilia? 9 Signs and symptoms of haemophilia 11 How is haemophilia diagnosed? 14 Diagnosis 14 Treatment 16 Port-a-cath 19 Managing joint bleeds with PRICE 19 Gene therapy 21 Possible complications of haemophilia 22 Inhibitors 22 Joint damage 22 Medical and dental treatment 23 Surgery Circumcision Dental care Medicines Vaccinations Bleeding disorder card Living with haemophilia 26 Sport and exercise 27 School, college and work 28 Travel 29 Pregnancy and haemophilia 30 Glossary of terms 32 About The Haemophilia Society 33 2 Understanding haemophilia Introduction This booklet is about haemophilia A and B. It gives a general overview of haemophilia and information on diagnosing, treating and living with the condition that we hope will answer your main questions. It has been written for people directly affected by haemophilia and for anyone interested in learning about haemophilia. If you are a parent and your child has recently been diagnosed with haemophilia you may be feeling quite overwhelmed. Remember, you’re not alone and many families are facing the same concerns and issues. Please do get in touch – we have lots of support and information available as well as services for parents and children. You can find out more via our website or Facebook pages, by emailing [email protected] or calling us on 020 7939 0780. The outlook is now the best it has ever been for people with haemophilia in the UK. -

Immune Thrombocytopenic Purpura in a Twin Girl Revealed by a Traumatic Injury in Parakou (North Benin)
Immune thrombocytopenic purpura in a twin girl revealed by a traumatic injury in parakou (North Benin) Adedemy JD 1*, Noudamadjo A 1, Kpanidja G 1, Agossou J 1, Agbeille Mohamed F 1, Dovonou CA 2 1 Mother and Child Department, Parakou Teaching Hospital, Republic of Benin, and Faculty of Medicine, University of Parakou West Africa 2 Department of Medicine, Parakou Teaching Hospital, and Faculty of Medicine, University of Parakou, West Africa Abstract Background: ITP seems to be rare but in tropical settings thrombocytopenia is often encountered among children. Objective: Authors through this case report are putting emphasy on the diagnosis and management of ITP in a 4 year old twin girl admitted in the pediatric emergency ward for hematuria and bleeding from various origins seen in the context of a domestic trauma. Results: The various clinical signs have been analyzed to confirm ITP through exclusion of other possible health conditions. The management of ITP depend on the severity of clinical signs and in some cases the situations can be life threatening. In this case report, Blood transfusion and corticosteroids were the main treatment tools. The hospital stay was about 47 days and an ambulatory follow up was conducted for almost 6 months. Conclusion: In the context of various bleeding disorders, hematuria and thrombocytopenia, autoimmune thrombocytopenia in a twin girl was revealed by a domestic trauma. Citation: Adedemy JD, Noudamadjo A, Kpanidja G, Agossou J, Agbeille MF, Dovonou CA (2019) Immune Thrombocytopenic Purpura in a twin girl revealed by a traumatic injury in Parakou (North Benin). Adv Pediatr Res 6:27.