Bolton Neighbourhood Engagement Report 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sunday 5Th September 2021
Prayer by Elaine and Phil Weaver on behalf of National and International Ministry team Covid is continuing to impact our mission partners significantly, and in many countries the situation is much worse than the UK. Please continue praying for their health; for their ministry activities; and for the governments and health systems in their countries. Welcome to St. Peter’s. We are 4 churches: St. Peter’s, St. Andrew’s, Barrow Bridge and Smithills Fellowship Release International is calling for prayer for Afghan Christians, following the rapid One Parish—One Church—One Vision takeover of their country by the Taliban. It is also working to lobby for safe passage for Christian refugees whose lives could be at risk. Please see https://releaseinternational.org/christians-in-afghanistan-call-to-prayer/ Sunday 5th September 2021 – Please pray for Urban Outreach as they work Urban Outreach (Dave & Chris Bagley) Church Without Walls - Livestreaming of services: You are warmly invited to with partners across Greater Manchester to house, help and support refugees arriving from join us for our service LIVE at 10.30am each Sunday on Zoom, Afghanistan. Donations of nappies, sanitary towels and baby clothes (as well as food) have Facebook and YouTube. Click on the ‘Church Live’ image at specifically been requested and these can be left in any of the parish Grub Tubs. www.stpetersparish.info to go straight to this service. The YouTube Craig & Elaine Watson (KISC Kathmandu) – Give thanks Craig and Elaine have arrived link for Sunday’s service is https://youtu.be/H9E731gYgew. safely in Kathmandu and have a place to live. -

How to Register
HOW TO REGISTER DISABLED ACCESS KEARSLEY The practice premises provides marked disabled MEDICAL CENTRE parking, wheelchair access, a disabled toilet, and The practice runs an open list to patients all patient facilities are available on the ground Jackson Street, Kearsley level. residing within the practice boundary. Bolton BL4 8EP Our boundary covers postcodes:- Telephone : 01204 462200 VIOLENT/ABUSIVE PATIENTS Fax: 01204 462744 The practice has a zero tolerance policy. Any BL4 (Kearsley, Farnworth) www.kearsleymedicalcentre.nhs.uk patient demonstrating threatening abusive/violent M26 (Stoneclough, Prestolee, Ringley, behaviour will be removed from the practice list. DOCTORS Outwood) COMPLAINTS/SUGGESTIONS The practice runs an in-house complaints M27 (Clifton up to M62 junction 16 slip road). procedure which is available if you are unhappy Dr George Herbert Ogden with any aspect of our service. Please contact MBChB MRCGP DRCOG DFFP surgery for details. I To register with the practice you will need Dr Liaqat Ali Natha If you have a suggestion, to improve our service the following: MBChB please ask the receptionist for a form. 1 New Patient Registration Pack, Dr Sumit Guhathakurta OUT OF HOURS EMERGENCIES completed together with 2 forms of ID MBChB MRCGP If you require urgent medical advice please ring 2 Appointment with practice nurse. 111 for assistance. If you require urgent medical Dr Charlotte Moran assistance when the surgery is closed, please Patients may specify the GP they wish to be telephone the surgery for further information. MBChB nMRCGP 999 should be dialled for medical emergencies registered with at registration, although the only Dr Rebecca Cruickshank choice of GP cannot be absolute, it depends on MBChB MRCGP availability, appropriateness and reasonable- USEFUL TELEPHONE NUMBERS Dr Molly Douglas ness. -

Neighbourhood Management & Area Working Programme
NEIGHBOURHOOD MANAGEMENT & AREA WORKING PROGRAMMES This document provides the breakdown of Neighbourhood Management and Area working funding over the past 6 years. The funding was allocated originally in 2-year programmes, and more recently as 1-year programme. The Neighbourhood Management programmes were coordinated and managed by Bolton Council (BMBC) and Bolton at Home (for Breightmet, Tonge with the Haulgh, Hulton Lane, Washacre and Johnson Fold). Members have discretion to shape priorities and spend within their areas but have been guided by the principles that projects should help to improve outcomes and narrow the gap between our least deprived and most deprived areas, and have a clear benefit to the quality of life in an area. The Council is publishing this historical information as part of its commitment to transparency; and has undertaken to publish information about new allocations on a regular basis. Note: April 2021 – This document has been updated to include the Neighbourhood Management information for the Bolton at Home managed areas. This includes: Breightmet, Tonge with the Haulgh, Hulton Lane, Washacre and Johnson Fold. 1 NEIGHBOURHOOD MANAGEMENT PROGRAMME 2013 – 2015 Neighbourhood Management - Crompton 2013 - 2015 Total £78,296 Project £ Lancs Wildlife Trust project tree planting and working with schools and groups 7,500 Various Traffic Regulation Orders covering Baythorpe St, Ullswater St and others 5,705 Crompton Road safety improvements 4,590 Police - Cobden room hire 10th July 2013 80 Police - 19th August 2014 48 Sledmere Close Street Lights 1,700 Dormer St - street lights 4,600 Road safety barriers outside former Bowling Green pub, Blackburn Rd 400 Road Safety Markings at St. -

Housing Land Availability Study 2008
Housing Land Availability Study Adjusted to March 2008 Development and Regeneration Department Planning Division– Spatial Planning Team 1 Current Housing Land Commitment Adjusted to March 2008 Background 1) This note updates the housing land position relating to the situation at the 31st March 2008 and considers the distribution of development land, provides information on new planning permission ns, and assesses the balance between private and housing association provision. It also provides detailed information relating to dwellings completed in the past year. Housing Land Requirements & Supply 2) Planning Policy Statement 3: Housing (PPS 3) was published in November 2006 with an objective to ensure that the planning system delivers a flexible, responsive supply of land, reflecting the principles of “Plan, Monitor, Manage”. From April 2007 Local Planning Authorities are required to identify sufficient specific and deliverable sites to ensure a rolling 5-year supply of housing and demonstrate the extent to which existing plans already fulfil the housing requirement. To be deliverable sites must be: available, suitable and achievable in the next 5 years and there is also a requirement to demonstrate a 15 year supply. 3) To address this the Local Planning Authority is required to undertake an annual Strategic Housing Land Availability Assessment (SHLAA). The first SHLAA for Bolton was commenced in December 2007 by consultants Roger Tym & Partners and the results from this will be published in the summer 2008 including a 5 and 15 year housing supply figures. 4) The SHLAA replaces the former annual Housing Land Availability Study that updated the housing land position in the Borough and reported on the distribution of development land, provided information on new planning permissions and dwelling completions. -
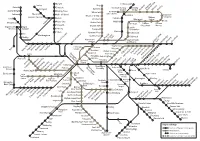
Wayfarer Rail Diagram 2020 (TPL Spring 2020)
Darwen Littleborough Chorley Bury Parbold Entwistle Rochdale Railway Smithy Adlington Radcliffe Kingsway Station Bridge Newbold Milnrow Newhey Appley Bridge Bromley Cross Business Park Whitefield Rochdale Blackrod Town Centre Gathurst Hall i' th' Wood Rochdale Shaw and Besses o' th' Barn Crompton Horwich Parkway Bolton Castleton Oldham Orrell Prestwich Westwood Central Moses Gate Mills Hill Derker Pemberton Heaton Park Lostock Freehold Oldham Oldham Farnworth Bowker Vale King Street Mumps Wigan North Wigan South Western Wallgate Kearsley Crumpsall Chadderton Moston Clifton Abraham Moss Hollinwood Ince Westhoughton Queens Road Hindley Failsworth MonsallCentral Manchester Park Newton Heath Salford Crescent Salford Central Victoria and Moston Ashton-underStalybridgeMossley Greenfield -Lyne Clayton Hall Exchange Victoria Square Velopark Bryn Swinton Daisy HillHag FoldAthertonWalkdenMoorside Shudehill Etihad Campus Deansgate- Market St Holt Town Edge Lane Droylsden Eccles Castlefield AudenshawAshtonAshton Moss West Piccadilly New Islington Cemetery Road Patricroft Gardens Ashton-under-Lyne Piccadilly St Peter’s Guide Weaste Square ArdwickAshburys GortonFairfield Bridge FloweryNewton FieldGodley for HydeHattersleyBroadbottomDinting Hadfield Eccles Langworthy Cornbrook Deansgate Manchester Manchester Newton-le- Ladywell Broadway Pomona Oxford Road Belle Vue Willows HarbourAnchorage City Salford QuaysExchange Quay Piccadilly Hyde North MediaCityUK Ryder Denton Glossop Brow Earlestown Trafford Hyde Central intu Wharfside Bar Reddish Trafford North -

Great Lever Area Forum Meeting – 8Th
GREAT LEVER AREA FORUM MEETING – 8TH NOVEMBER 2012 Present – 11members of the public attended the meeting Councillor Mohammed Ayub Great Lever Ward Councillor Mohammed Iqbal Great Lever Ward Councillor Madeline Murray Great Lever Ward Also in attendance Tim Hill - Area Forum Chief Officer John Pye - Neighbourhood Manager, Chief Executive’s Department Stephen Rowson - Business Support Officer, Chief Executive’s Department Andy Bolan - Environmental Services Mark Hoban - Environmental Services Shauna Morton - Bolton at Home Denise Kehoe - Bolton at Home Chris Farrell - Greater Manchester Police Chris Walsh - Greater Manchester Police Simon Hines - Greater Manchester Police Apologies were received from Yasmin Qureshi MP. Councillor Murray in the Chair. 9. WELCOME, INTRODUCTIONS Councillor Murray welcomed everyone and introduced the Officers in attendance she also advised residents that the last two remaining budget meetings Bolton Council were to be held on Wednesday 14th November 2012. 10. DECLARATIONS OF INTEREST FROM COUNCILLORS AND OFFICERS There were no Declarations of Interest. 11. MINUTES OF THE PREVIOUS MEETING The minutes of the previous meeting were submitted and approved as a correct record. Further to minute 5, members were advised that the planning application for Clarendon School had now received planning consent. 12. MANAGED WEEKLY COLLECTIONS Mark Hoban from the Environmental Services gave a presentation in relation to Bolton Council’s managed weekly waste collections. The main points were: The Council had to save £35.6 million between 2013- 2015 Central and Local Government commitment to increase recycling in Bolton was falling behind Larger aim was for zero waste to landfill and more recycling through all the newly built facilities Transformation of services would ease the burden of budget cuts on vulnerable adults and children Significant rising costs for the disposal of residual waste £15.8m - £24.6m. -

Classified Road List
CLASSIFIED HIGHWAYS Ainsworth Lane Bolton B6208 Albert Road Farnworth A575 Arthur Lane Turton B6196 Arthur Street Bolton B6207 Bank Street Bolton A676 Beaumont Road Bolton A58 Belmont Road Bolton A675 Blackburn Road Turton and Bolton A666 Blackhorse Street Blackrod B5408 Blackrod by-Pass Blackrod A6 Blair Lane Bolton Class 3 Bolton Road Farnworth A575 Bolton Road Kearsley A666 Bolton Road Turton A676 Bolton Road Farnworth A575 Bolton Road Kearsley A666 Bolton Road Westhoughton B5235 Bow Street Bolton B6205 Bradford Road Farnworth Class 3 Bradford Street Bolton A579 Bradshaw Brow Turton A676 Bradshaw Road Turton A676 Bradshawgate Bolton A575 Bridge Street Bolton B6205 Bridgeman Place Bolton A579 Buckley Lane Farnworth A5082 Bury New Road Bolton A673 Bury Road Bolton A58 Cannon Street Bolton B6201 Castle Street Bolton B6209 Chapeltown Road Turton B6319 Chorley New Road Horwich and Bolton A673 Chorley Old Road Horwich and Bolton B6226 Chorley Road Blackrod A6 Chorley Road Westhougton A6 Chorley Road Blackrod B5408 Church Lane Westhoughton Church Street Little Lever A6053 Church Street Westhoughton B5236 Church Street Blackrod B5408 Church Street Horwich B6226 College Way Bolton B6202 Colliers Row Road Bolton Class 3 Cricketer’s Way Westhoughton A58 Crompton Way Bolton A58 Crown Lane Horwich B5238 Dark Lane Blackrod Class 3 Darwen Road Turton B6472 Deane Road Bolton A676 Deansgate Bolton A676 Derby Street Bolton A579 Dicconson Lane Westhoughton B5239 Dove Bank Road Little Lever B6209 Eagley Way Bolton Class 3 Egerton Street Farnworth A575 -

The London Gazette, 15Th January 1988 527
THE LONDON GAZETTE, 15TH JANUARY 1988 527 ROSS, Manny of 57 Lyndhurst Gardens, Finchley, London, N.3 O'KEEFE, James Lawrence, residing at 52/54 Charles Lane, of no present occupation, formerly a TRAINEE MACHINIST Haslingden, Lancashire, lately residing and carrying on previously a COMPANY DIRECTOR. Court—HIGH business at Cuba Mill, Bolton Road North, Stubbins, COURT OF JUSTICE. No. of Matter—1084 of 1982. Date Ramsbottom, Greater Manchester as a COMMERCIAL Fixed for Hearing—4th February 1988. 10.30 a.m. Place- VEHICLE REPAIRER and MOTOR DEALER under the Court 38A, Ground Floor, West Green Building, Royal Courts style of Mercury Motors, previously residing and carrying on of Justice, Strand, London WC2A 2JY. business as a HAULAGE CONTRACTOR at Lockgate, Rawtenstall Road, Haslingden, 13 Sidmouth Avenue, Haslingden and Longhquse Farm, Haslingden and formerly ROTHWELL, Leonard Bryce, a CATERER of and lately trading trading as a MOT Testing Station at Bridge Mill, Rochdale at 31 Hungerdown, Chingford, London E.4 as D. L. R. Road, Edenfield all in Lancashire. Court—BOLTON. No. of Catering as a CATERING CONTRACTOR. Court—HIGH Matter—46 of 1982. Date Fixed for Hearing—21st January COURT OF JUSTICE. No. of Matter—400 of 1982. Date 1988. 10.30 a.m. Place—Bolton County Court, The Court Fixed for Hearing—4th February 1988. 10.30 a.m. Place- House, Blackhorse Street, Bolton. Court 38A, Ground Floor, West Green Building, Royal Courts of Justice, Strand, London WC2A 2JY. PENARSKI, Aleksander Wladyslaw (described in the Receiving SUTTON, Eric of 37 Richmond Road, Twickenham, Middlesex, Order as Alex Penarski) Professional Boxer, residing and lately Vending Machine Siting Agent trading as Indorvend Services carrying on business as a CAR SALESMAN at 38A Darley at 37 Richmond Road, Twickenham, Middlesex, described as Grove, Farnworth, Bolton, in the county of Greater a VENDING MACHINE DISTRIBUTOR. -
Communicating with the Neighbourhoods
Communicating with the Neighbourhoods June 2018 This work was commissioned from Healthwatch Bolton by Bolton CCG as part of the Bolton Engagement Alliance Communicating with the Neighbourhoods - June 2018 1 Communicating with the Neighbourhoods - Abstract This report is based on conversations or responses freely given by members of the public. Where possible quotations are used to illustrate individual or collectively important experiences. Engagement officers collect responses verbatim and we also present these in our final report as an appendix. This is important in showing the accuracy of our analysis, and so that further work can be done by anyone wishing to do so. A full explanation of the guiding principles and framework for how we do engagement and analysis can be found online on our website www.healthwatchbolton.co.uk. HWB - Communicating with the Neighbourhoods - June 2018 2 Communicating with the Neighbourhoods - Disclaimer Please note that this report relates to findings observed and contributed by members of the public in relation to the specific project as set out in the methodology section of the report. Our report is not a representative portrayal of the experiences of all service users and staff, only an analysis of what was contributed by members of the public, service users, patients and staff within the project context as described. HWB - Communicating with the Neighbourhoods - June 2018 3 Communicating with the Neighbourhoods - Background This piece of work builds on Neighbourhood Engagement Workshops carried out in September and October 2017 by the Bolton Engagement Alliance. The reports of these workshops make a number of suggestions as to how individuals in the Neighbourhoods could be kept informed about developments in health and social care. -

Strategic Flood Risk Assessment for Greater Manchester
Strategic Flood Risk Assessment for Greater Manchester Sub-Regional Assessment Appendix B – Supporting Information “Living Document” June 2008 Association of Greater Manchester Authorities SFRA – Sub-Regional Assessment Revision Schedule Strategic Flood Risk Assessment for Greater Manchester June 2008 Rev Date Details Prepared by Reviewed by Approved by 01 August 2007 DRAFT Michael Timmins Jon Robinson David Dales Principal Flood Risk Associate Director Specialist Peter Morgan Alan Houghton Planner Head of Planning North West 02 December DRAFT FINAL Michael Timmins Jon Robinson David Dales 2007 Principal Flood Risk Associate Director Specialist Peter Morgan Alan Houghton Planner Head of Planning North West 03 June 2008 FINAL Michael Timmins Jon Robinson David Dales Principal Flood Risk Associate Director Specialist Anita Longworth Alan Houghton Principal Planner Head of Planning North West Scott Wilson St James's Buildings, Oxford Street, Manchester, This document has been prepared in accordance with the scope of Scott Wilson's M1 6EF, appointment with its client and is subject to the terms of that appointment. It is addressed to and for the sole and confidential use and reliance of Scott Wilson's client. Scott Wilson United Kingdom accepts no liability for any use of this document other than by its client and only for the purposes for which it was prepared and provided. No person other than the client may copy (in whole or in part) use or rely on the contents of this document, without the prior written permission of the Company Secretary of Scott Wilson Ltd. Any advice, opinions, Tel: +44 (0)161 236 8655 or recommendations within this document should be read and relied upon only in the context of the document as a whole. -

2018-0411 Response by Greater Manchester Police
GREATER MANCHESTER POLICE Ian Hopkins QPM, MBA Chief Constable Ms Joanne Kearsley HM Senior Coroner HM Coroner's Court The Phoenix Centre, L/Cpl Stephen Shaw MC Way Heywood OL191LR 28 February 2019 Dear Ms Kearsley Re: Regulation 28 Report following the Inquest touching upon the death of Gregory Rewkowski Thank you for your report sent by email dated 3 January 2019 in respect of Gregory Rewkowski (deceased) and pursuant to Regulations 28 and 29 of The Coroners (Investigations) Regulations 2013 and paragraph 7, Schedule 5 of the Coroners and Justice Act 2009. Having carefully considered your report and the matters therein, I reply to the concerns raised as follows: Extract from Regulation 28, point 1: There is a lack of acknowledgement of the role of the police when dealing with people who are taken on a Section 136 from their own home. The Court did not explore the numbers of Section 136 patients who are taken to a place of safety from their home address. The Court heard how Mr Rewkowski had been taken from his own home on the 1th September. Other agencies are clearly familiar with this process and how GMP facilitate this. However this was also used as an explanation as to why GMP may have been restricted in what they could do on the 2th and 2Efh October i.e. " ... there is nothing we can do if we attend at his own home. We have no powers." There appears to be a significant difference between the legal position and the practical reality of how police deal with such matters if they are called to a home address. -

Board of Directors Agenda
Board of Directors Thu 26 November 2020, 09:00 - 12:30 WebEx Agenda 09:00 - 09:00 1. Welcome and Introductions 0 min Verbal Donna Hall 01 Agenda Part One Board meeting November 2020_v2.1.pdf (3 pages) 1.1. Bolton a poem by Ibby Ismail 09:00 - 09:00 2. Patient Story 0 min Verbal Marie Forshaw 09:00 - 09:00 3. Apologies for Absence 0 min Verbal Esther Steel 09:00 - 09:00 4. Declarations of Interest 0 min Verbal Donna Hall 09:00 - 09:00 5. Minutes of the meeting held on 30th July 2020 0 min Minutes Donna Hall 5 Board of Directors Minutes - 24.09.2020 copy.pdf (11 pages) 09:00 - 09:00 6. Action Sheet 0 min Action Sheet Donna Hall 6 Board actions September 2020.pdf (1 pages) 09:00 - 09:00 7. Matters Arising 0 min Verbal Donna Hall 09:00 - 09:00 8. CEO Report 0 min Report Fiona Noden 8. CEO report November 20_v2.pdf (6 pages) 09:00 - 09:00 9. Covid Update and Reset 0 min Presentation Andy Ennis and Sharon Martin 9.1. Covid Health and Wellbeing James Mawrey 9.1 BOD report - Staff HWB update Nov20-v2.pdf (5 pages) 09:00 - 09:00 10. Flu Vaccination update 0 min Report Marie Forshaw 10 Healthcare worker flu vaccination best practice management checklist Nov 20 (2).pdf (2 pages) 09:00 - 09:00 11. Integrated Performance Report 0 min Report Andy Ennis 11. Integrated Performance Report Nov 2020.pdf (50 pages) 09:00 - 09:00 12.