Nontuberculous Mycobacteria (Ntm)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arcanobacterium Haemolyticum Type Strain (11018)
Lawrence Berkeley National Laboratory Recent Work Title Complete genome sequence of Arcanobacterium haemolyticum type strain (11018). Permalink https://escholarship.org/uc/item/03f632gf Journal Standards in genomic sciences, 3(2) ISSN 1944-3277 Authors Yasawong, Montri Teshima, Hazuki Lapidus, Alla et al. Publication Date 2010-09-28 DOI 10.4056/sigs.1123072 Peer reviewed eScholarship.org Powered by the California Digital Library University of California Standards in Genomic Sciences (2010) 3:126-135 DOI:10.4056/sigs.1123072 Complete genome sequence of Arcanobacterium T haemolyticum type strain (11018 ) Montri Yasawong1, Hazuki Teshima2,3, Alla Lapidus2, Matt Nolan2, Susan Lucas2, Tijana Glavina Del Rio2, Hope Tice2, Jan-Fang Cheng2, David Bruce2,3, Chris Detter2,3, Roxanne Tapia2,3, Cliff Han2,3, Lynne Goodwin2,3, Sam Pitluck2, Konstantinos Liolios2, Natalia Ivanova2, Konstantinos Mavromatis2, Natalia Mikhailova2, Amrita Pati2, Amy Chen4, Krishna Palaniappan4, Miriam Land2,5, Loren Hauser2,5, Yun-Juan Chang2,5, Cynthia D. Jeffries2,5, Manfred Rohde1, Johannes Sikorski6, Rüdiger Pukall6, Markus Göker6, Tanja Woyke2, James Bristow2, Jonathan A. Eisen2,7, Victor Markowitz4, Philip Hugenholtz2, Nikos C. Kyrpides2, and Hans-Peter Klenk6* 1 HZI – Helmholtz Centre for Infection Research, Braunschweig, Germany 2 DOE Joint Genome Institute, Walnut Creek, California, USA 3 Los Alamos National Laboratory, Bioscience Division, Los Alamos, New Mexico, USA 4 Biological Data Management and Technology Center, Lawrence Berkeley National Laboratory, Berkeley, California, USA 5 Oak Ridge National Laboratory, Oak Ridge, Tennessee, USA 6 DSMZ - German Collection of Microorganisms and Cell Cultures GmbH, Braunschweig, Germany 7 University of California Davis Genome Center, Davis, California, USA *Corresponding author: Hans-Peter Klenk Keywords: obligate parasite, human pathogen, pharyngeal lesions, skin lesions, facultative anaerobe, Actinomycetaceae, Actinobacteria, GEBA Arcanobacterium haemolyticum (ex MacLean et al. -

INTERNATIONAL BULLETIN of BACTERIOLOGICAL NOMENCLATURE and TAXONOMY Vol
INTERNATIONAL BULLETIN OF BACTERIOLOGICAL NOMENCLATURE AND TAXONOMY Vol. 15, No. 3 July 15, 1965 pp. 143-163 THE CLASSIFICATION AND PHYLOGENETIC RELATIONSHIPS OF THE ACTINOMYCETALES ' Leo Pine and Lucille Georg Communicable Disease Center, Public Health Service, U. S. Department of Health, Education, and Welfare, Atlanta, Georgia SUMMARY. The taxonomic and phylogenetic re- lationships of members of the order Actino- mycetales have been examined. On the basis of cellular and colony morphology, cell wall composition, fermentation products, and cer- tain physiological characteristics, the taxa within the family Actinomycetaceae were divided into two groups. Each group was closely related to members of the family -Lactobacillaceae. One group consisted of Actinomyces israelii, -A. naeslundii, ,A. pro- pionicus, Nocardia dentocariosus and Odonto- myces viscosis ("hamster organism"). The second group consisted of bovis, ,A. erik- sonii, and Lactobacillus bifidusA. type 11 (k parabifidus). This latter organism was re- named Actinomyces pa.rabifidus nov. comb. because its morphological, physiological and biochemical characteristics related it to the members of both groups of the genus Actino- myces. The families Streptomycetaceae and Mycobacteriaceae appeared more closely re- lated to the family Corynebacteriaceae than to the family Actinomycetaceae. The use of certain criteria for classification and deter- mination of phylogenetic relationships was discussed. We have stressed those areas in which necessasy information is lacking. A report to -

From Genotype to Phenotype: Inferring Relationships Between Microbial Traits and Genomic Components
From genotype to phenotype: inferring relationships between microbial traits and genomic components Inaugural-Dissertation zur Erlangung des Doktorgrades der Mathematisch-Naturwissenschaftlichen Fakult¨at der Heinrich-Heine-Universit¨atD¨usseldorf vorgelegt von Aaron Weimann aus Oberhausen D¨usseldorf,29.08.16 aus dem Institut f¨urInformatik der Heinrich-Heine-Universit¨atD¨usseldorf Gedruckt mit der Genehmigung der Mathemathisch-Naturwissenschaftlichen Fakult¨atder Heinrich-Heine-Universit¨atD¨usseldorf Referent: Prof. Dr. Alice C. McHardy Koreferent: Prof. Dr. Martin J. Lercher Tag der m¨undlichen Pr¨ufung: 24.02.17 Selbststandigkeitserkl¨ arung¨ Hiermit erkl¨areich, dass ich die vorliegende Dissertation eigenst¨andigund ohne fremde Hilfe angefertig habe. Arbeiten Dritter wurden entsprechend zitiert. Diese Dissertation wurde bisher in dieser oder ¨ahnlicher Form noch bei keiner anderen Institution eingereicht. Ich habe bisher keine erfolglosen Promotionsversuche un- ternommen. D¨usseldorf,den . ... ... ... (Aaron Weimann) Statement of authorship I hereby certify that this dissertation is the result of my own work. No other person's work has been used without due acknowledgement. This dissertation has not been submitted in the same or similar form to other institutions. I have not previously failed a doctoral examination procedure. Summary Bacteria live in almost any imaginable environment, from the most extreme envi- ronments (e.g. in hydrothermal vents) to the bovine and human gastrointestinal tract. By adapting to such diverse environments, they have developed a large arsenal of enzymes involved in a wide variety of biochemical reactions. While some such enzymes support our digestion or can be used for the optimization of biotechnological processes, others may be harmful { e.g. mediating the roles of bacteria in human diseases. -

INVESTIGATING the ACTINOMYCETE DIVERSITY INSIDE the HINDGUT of an INDIGENOUS TERMITE, Microhodotermes Viator
INVESTIGATING THE ACTINOMYCETE DIVERSITY INSIDE THE HINDGUT OF AN INDIGENOUS TERMITE, Microhodotermes viator by Jeffrey Rohland Thesis presented for the degree of Doctor of Philosophy in the Department of Molecular and Cell Biology, Faculty of Science, University of Cape Town, South Africa. April 2010 ACKNOWLEDGEMENTS Firstly and most importantly, I would like to thank my supervisor, Dr Paul Meyers. I have been in his lab since my Honours year, and he has always been a constant source of guidance, help and encouragement during all my years at UCT. His serious discussion of project related matters and also his lighter side and sense of humour have made the work that I have done a growing and learning experience, but also one that has been really enjoyable. I look up to him as a role model and mentor and acknowledge his contribution to making me the best possible researcher that I can be. Thank-you to all the members of Lab 202, past and present (especially to Gareth Everest – who was with me from the start), for all their help and advice and for making the lab a home away from home and generally a great place to work. I would also like to thank Di James and Bruna Galvão for all their help with the vast quantities of sequencing done during this project, and Dr Bronwyn Kirby for her help with the statistical analyses. Also, I must acknowledge Miranda Waldron and Mohammed Jaffer of the Electron Microsope Unit at the University of Cape Town for their help with scanning electron microscopy and transmission electron microscopy related matters, respectively. -
C O N F E R E N C E 25 1 May 2019
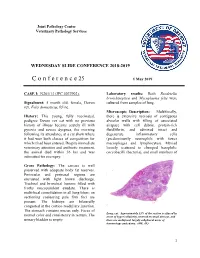
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2018-2019 C o n f e r e n c e 25 1 May 2019 CASE I: N261/13 (JPC 4037902). Laboratory results: Both Bordetella bronchiseptica and Mycoplasma felis were Signalment: 5 month old, female, Devon cultured from samples of lung. rex, Felis domesticus, feline. Microscopic Description: Multifocally, History: This young, fully vaccinated, there is extensive necrosis of contiguous pedigree Devon rex cat with no previous alveolar walls with filling of associated history of illness became acutely ill with airspace with cell debris, protein-rich pyrexia and severe dyspnea, the morning fluid/fibrin, and admixed intact and following its attendance at a cat show where degenerate inflammatory cells it had won both classes of competition for (predominantly neutrophils with fewer which it had been entered. Despite immediate macrophages and lymphocytes). Myriad veterinary attention and antibiotic treatment, loosely scattered to clumped basophilic the animal died within 36 hrs and was coccobacilli (bacteria), and small numbers of submitted for necropsy. Gross Pathology: The carcass is well preserved with adequate body fat reserves. Periocular and perinasal regions are encrusted with light brown discharge. Tracheal and bronchial lumens filled with frothy mucopurulent exudate. There is multifocal consolidation in all lung lobes: on sectioning coalescing pale firm foci are present. The kidneys are bilaterally congested at the cortico-medullary junction. The stomach contains mucus only. Feces of Lung, cat. Approximately 33% of the section is effaced by normal color and consistency in rectum. The areas of hyper\cellularity centered on small airways, and urinary bladder is empty. -

Microbial and Mineralogical Characterizations of Soils Collected from the Deep Biosphere of the Former Homestake Gold Mine, South Dakota
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln US Department of Energy Publications U.S. Department of Energy 2010 Microbial and Mineralogical Characterizations of Soils Collected from the Deep Biosphere of the Former Homestake Gold Mine, South Dakota Gurdeep Rastogi South Dakota School of Mines and Technology Shariff Osman Lawrence Berkeley National Laboratory Ravi K. Kukkadapu Pacific Northwest National Laboratory, [email protected] Mark Engelhard Pacific Northwest National Laboratory Parag A. Vaishampayan California Institute of Technology See next page for additional authors Follow this and additional works at: https://digitalcommons.unl.edu/usdoepub Part of the Bioresource and Agricultural Engineering Commons Rastogi, Gurdeep; Osman, Shariff; Kukkadapu, Ravi K.; Engelhard, Mark; Vaishampayan, Parag A.; Andersen, Gary L.; and Sani, Rajesh K., "Microbial and Mineralogical Characterizations of Soils Collected from the Deep Biosphere of the Former Homestake Gold Mine, South Dakota" (2010). US Department of Energy Publications. 170. https://digitalcommons.unl.edu/usdoepub/170 This Article is brought to you for free and open access by the U.S. Department of Energy at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in US Department of Energy Publications by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. Authors Gurdeep Rastogi, Shariff Osman, Ravi K. Kukkadapu, Mark Engelhard, Parag A. Vaishampayan, Gary L. Andersen, and Rajesh K. Sani This article is available at DigitalCommons@University of Nebraska - Lincoln: https://digitalcommons.unl.edu/ usdoepub/170 Microb Ecol (2010) 60:539–550 DOI 10.1007/s00248-010-9657-y SOIL MICROBIOLOGY Microbial and Mineralogical Characterizations of Soils Collected from the Deep Biosphere of the Former Homestake Gold Mine, South Dakota Gurdeep Rastogi & Shariff Osman & Ravi Kukkadapu & Mark Engelhard & Parag A. -

Lumpy Jaw" in Cattle
THE NOMENCLATURE AND CLASSIFICATION OF THE ACTINOMYCETES1 SELMAN A. WAKSMAN AND ARTHUR T. HENRICI' New Jersey Agricultural Experiment Station, Rutgers University, and the Department of Bacteriology, University of Minnesota Received for publication April 10, 1943 Since the publication by one of us (Waksman, 1940) of a system of classifica- tion of actinomycetes, considerable criticism was expressed in regard to the designation and position of the anaerobic pathogenic species, the cause of com- mon actinomycosis in man and "lumpy jaw" in cattle. This type of organism was placed in the genus Cohnistreptothrix Pinoy, the generic name Actinomyces being reserved for the aerobic species forming aerial mycelium-bearing spores. This could be justified on the ground that the organism seen by Harz was so poorly described and illustrated that it is unrecognizable by present day stand- ards, and that therefore a new name could well be applied to the organism of actinomycosis in cattle; that further the name Actinomyces was the first one ap- plied to cultivated, aerobic, spore-forming species which can be recognized by present day standards. This has been the attitude of a number of recent medical mycologists, especially the Italian workers (Ciferri and RedaeUi, 1929; Baldacci, 1939). Critics of Waksman's classification have, however, maintained that while Harz' description of his organism is perhaps vague, there is no question concern- ing the nature of the disease he studied, and that the chances are overwhelmingly in favor of his having actually observed the anaerobic pathogenic filamentous organism first described by Israel. Further, under the Botanical Code, the name Actinomyces must be applied either to the organism of "lumpy jaw" or not used at all. -

MALDI-TOF Best Practices Writing Group and the APHL TB Subcommittee, with Significant Input and Contributions from the Following Individuals
INFECTIOUS DISEASES AUGUST 2019 Best Practices for Identification of Mycobacterium Species Using Matrix-Assisted Laser Desorption Ionization-Time of Flight Mass Spectrometry PURPOSE AND BACKGROUND The ability to control tuberculosis in patients and populations depends on rapid detection and identification ofMycobacterium tuberculosis complex (MTBC). This requires a mechanism to accurately identify MTBC and other mycobacteria from primary broth cultures,1,2 and broth and/or solid media subculture growth.3–5 Matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF) is a rapid, sensitive and cost-effective method for organism identification that is routinely used in clinical and public health laboratories. The purpose of this document is to outline best practices for the use of the MALDI-TOF technique as it specifically applies to the identification ofMycobacterium species, including both MTBC and non-tuberculous Mycobacterium (NTM). This document, structured to mirror a laboratory’s own decision and implementation process, will guide readers through the considerations for using the MALDI-TOF system and the necessary steps to implement and maintain testing of MTBC and NTMs using MALDI-TOF. A reader who is considering whether MALDI-TOF is the best fit for their laboratory should review these additional resources.6–11 The MALDI-TOF system identifies microbes, usually bacteria or fungal species, through an analytical technique based on the detection and measurement of ionized analytes in the sample.12,13 When the sample is tested, the MALDI-TOF system generates a spectral profile—referred to as the peptide mass fingerprint (PMF)—which can then be compared to profiles in a database of known PMFs to find a match. -

Phylum Family Genus Abundance Occurrence Abundance Occurrence Abundance Occurrence Abundance Occurrence Clr Vs
Month 4 VCt n=10 CCt n=10 VLr n=9 CLr n=11 Pvalues of each 2by2 comparison Phylum Family Genus Abundance Occurrence Abundance Occurrence Abundance Occurrence Abundance Occurrence CLr vs. CCt VCt vs. CCt VLr vs. CCt CLr vs. VCt CLr vs. VLr VCt vs. VLr Actinobacteria P.Actinobacteria 81.2% 100% 63.6% 100% 62.2% 100% 48.2% 100% 0.863 0.052 0.780 0.223 1.000 0.156 Actinobacteria Actinomycetaceae F.Actinomycetaceae 0.0% 0% 0.0% 50% 0.1% 56% 0.1% 55% 0.404 0.033 0.641 0.012 0.481 0.011 Actinobacteria Actinomycetaceae Actinomyces G.Actinomyces 0.0% 0% 0.0% 40% 0.1% 56% 0.1% 55% 0.276 0.087 0.455 0.012 0.481 0.011 Actinobacteria Actinomycetaceae Varibaculum G.Varibaculum 0.0% 0% 0.0% 10% 0.0% 0% 0.0% 0% 0.476 1.000 1.000 1.000 1.000 1.000 Actinobacteria Bifidobacteriaceae F.Bifidobacteriaceae 57.3% 100% 54.9% 90% 53.4% 100% 40.8% 100% 0.918 0.579 0.780 0.387 1.000 0.315 Actinobacteria Bifidobacteriaceae Aeriscardovia G.Aeriscardovia 0.0% 0% 0.0% 0% 0.0% 0% 0.0% 9% 1.000 1.000 1.000 1.000 1.000 1.000 Actinobacteria Bifidobacteriaceae Bifidobacterium G.Bifidobacterium 56.6% 100% 54.4% 90% 53.1% 100% 40.1% 100% 0.973 0.579 0.780 0.426 1.000 0.400 Actinobacteria Bifidobacteriaceae f_Bifidobacteriaceae_g_Unc G.f_Bifidobacteriaceae_g_Unc 0.8% 90% 0.5% 90% 0.6% 100% 0.6% 82% 0.704 0.363 0.968 0.314 0.694 0.968 Actinobacteria c_Actinobacteria_f_Unc F.c_Actinobacteria_f_Unc 0.2% 70% 0.0% 50% 0.2% 89% 0.0% 45% 0.911 0.135 0.013 0.099 0.022 0.507 Actinobacteria c_Actinobacteria_f_Unc c_Actinobacteria_g_Unc G.c_Actinobacteria_g_Unc 0.2% 70% 0.0% 50% 0.2% -

Evaluation of the Airway Microbiome in Nontuberculous Mycobacteria Disease
ORIGINAL ARTICLE LUNG INFECTION Evaluation of the airway microbiome in nontuberculous mycobacteria disease Imran Sulaiman 1, Benjamin G. Wu1, Yonghua Li1, Adrienne S. Scott1, Patrick Malecha1, Benjamin Scaglione1, Jing Wang 1, Ashwin Basavaraj1, Samuel Chung1, Katrina Bantis1, Joseph Carpenito1, Jose C. Clemente3,4, Nan Shen3, Jamie Bessich1, Samaan Rafeq1, Gaetene Michaud1, Jessica Donington1, Charissa Naidoo5, Grant Theron5, Gail Schattner1, Suzette Garofano1, Rany Condos1, David Kamelhar1, Doreen Addrizzo-Harris1 and Leopoldo N. Segal1,2 Affiliations: 1Division of Pulmonary, Critical Care, and Sleep Medicine, New York University School of Medicine, New York, NY, USA. 2Dept of Medicine, New York University School of Medicine, New York, NY, USA. 3Dept of Genetics and Genomic Sciences and Immunology Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA. 4Precision Immunology Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA. 5Medicine and Health Sciences, Stellenbosch University, DST/NRF of Excellence for Biomedical Tuberculosis Research and SA MRC Centre for Molecular and Cellular Biology, Division of Molecular Biology and Human Genetics Tygerberg, Cape Town, South Africa. Correspondence: Leopoldo N. Segal, NYU School of Medicine, 462 First Ave 7W54, New York, NY 10016, USA. E-mail: [email protected] @ERSpublications 16S rRNA gene sequencing is not sensitive to detect Mycobacterium but identifies microbiota signatures associated with inflammation http://ow.ly/opXm30ldtQH Cite this article as: Sulaiman I, Wu BG, Li Y, et al. Evaluation of the airway microbiome in nontuberculous mycobacteria disease. Eur Respir J 2018; 52: 1800810 [https://doi.org/10.1183/ 13993003.00810-2018]. ABSTRACT Aspiration is associated with nontuberculous mycobacterial (NTM) pulmonary disease and airway dysbiosis is associated with increased inflammation. -

PDF Download
The International Journal of Biotechnology 2012 Vol.1, No.1, pp.1-20 ISSN(e): 2306-6148 ISSN(p): 2306-9864 © 2012 Conscientia Beam. All Rights Reserved. THERMOSTABLE XYLANASES OF MICROBIAL ORIGIN: RECENT INSIGHTS AND BIOTECHNOLOGICAL POTENTIAL S.S. Kanwar1 --- Sunita Devi2 1Professor and Head, Department of Microbiology, College of Basic Sciences,CSK Himachal Pradesh Agricultural University, India 2Ph. D Scholar, Department of Microbiology, College of Basic Sciences, CSK Himachal Pradesh Agricultural University, India ABSTRACT Xylanases are hydrolases which depolymerise the plant cell wall component-xylan, the second most abundant polysaccharide. They are mainly produced by microorganisms but can also be found in plants, marine algae, protozoans, crustaceans, insects, and snails. Because of their ability to break down xylan, these enzymes especially of microbial origin, have attracted more attention due to their potential role in pulping and bleaching processes, in food and feed industry, textile processes and organic waste treatment. Xylanases are more suitable in paper and pulp industry than lignin degrading enzymes. Owing to the increasing biotechnological importance of thermostable xylanases, many potential thermophilic and hyperthermophilic bacterial genera like Bacillus, Thermotoga, Streptomyces, Thermomyces, Pyrococcus and Sulfolobus and some fungal genera like Trichoderma, Aspergillus, Penicillum, Aureobasidium have been identified. As tolerance to higher pH and temperature are desirable properties of xylanase for effective use in pulp treatment, thermophillic organisms are of special interest as a source of novel thermostable xylanases. But for large scale production of xylanases, reduction of cost is still very challenging. This review encompasses the sources, classification, industrial and future prospects of xylanases with special reference to thermostable ones. -

Phylogenomics and Evolutionary Dynamics of the Family Actinomycetaceae
GBE Phylogenomics and Evolutionary Dynamics of the Family Actinomycetaceae Kelei Zhao1,y,WujiaoLi1,y, Chunlan Kang1, Lianming Du1, Ting Huang1, Xiuyue Zhang1,MinWu2,*, and Bisong Yue3,* 1Key Laboratory of Bio-resources and Eco-environment (Ministry of Education), College of Life Sciences, Sichuan University, Chengdu, China 2Department of Basic Sciences, School of Medicine and Health Sciences, University of North Dakota 3Sichuan Key Laboratory of Conservation Biology on Endangered Wildlife, College of Life Sciences, Sichuan University, Chengdu, China *Corresponding author: E-mail: [email protected]; [email protected]. yThese authors contributed equally to this work. Accepted: September 14, 2014 Data deposition: Whole Genome Shotgun projects of Trueperella pyogenes TP8 have been deposited at DDBJ/EMBL/GenBank under the accession CP007003. Abstract The family Actinomycetaceae comprises several important pathogens that impose serious threat to human health and cause sub- stantial infections of economically important animals. However, the phylogeny and evolutionary dynamic of this family are poorly characterized. Here, we provide detailed description of the genome characteristics of Trueperella pyogenes, a prevalent opportunistic bacterium that belongs to the family Actinomycetaceae, and the results of comparative genomics analyses suggested that T. pyogenes was a more versatile pathogen than Arcanobacterium haemolyticum in adapting various environments. We then per- formed phylogenetic analyses at the genomic level and showed that, on the whole, the established members of the family Actinomycetaceae were clearly separated with high bootstrap values but confused with the dominant genus Actinomyces, because the species of genus Actinomyces were divided into three main groups with different G+C content. Although T. pyogenes and A.