Applications of Machine Learning to Diagnosis and Treatment of Neurodegenerative Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Artificial Consciousness and the Consciousness-Attention Dissociation
Consciousness and Cognition 45 (2016) 210–225 Contents lists available at ScienceDirect Consciousness and Cognition journal homepage: www.elsevier.com/locate/concog Review article Artificial consciousness and the consciousness-attention dissociation ⇑ Harry Haroutioun Haladjian a, , Carlos Montemayor b a Laboratoire Psychologie de la Perception, CNRS (UMR 8242), Université Paris Descartes, Centre Biomédical des Saints-Pères, 45 rue des Saints-Pères, 75006 Paris, France b San Francisco State University, Philosophy Department, 1600 Holloway Avenue, San Francisco, CA 94132 USA article info abstract Article history: Artificial Intelligence is at a turning point, with a substantial increase in projects aiming to Received 6 July 2016 implement sophisticated forms of human intelligence in machines. This research attempts Accepted 12 August 2016 to model specific forms of intelligence through brute-force search heuristics and also reproduce features of human perception and cognition, including emotions. Such goals have implications for artificial consciousness, with some arguing that it will be achievable Keywords: once we overcome short-term engineering challenges. We believe, however, that phenom- Artificial intelligence enal consciousness cannot be implemented in machines. This becomes clear when consid- Artificial consciousness ering emotions and examining the dissociation between consciousness and attention in Consciousness Visual attention humans. While we may be able to program ethical behavior based on rules and machine Phenomenology learning, we will never be able to reproduce emotions or empathy by programming such Emotions control systems—these will be merely simulations. Arguments in favor of this claim include Empathy considerations about evolution, the neuropsychological aspects of emotions, and the disso- ciation between attention and consciousness found in humans. -
Artificial Brain Project of Visual Motion
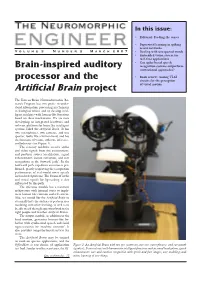
In this issue: • Editorial: Feeding the senses • Supervised learning in spiking neural networks V o l u m e 3 N u m b e r 2 M a r c h 2 0 0 7 • Dealing with unexpected words • Embedded vision system for real-time applications • Can spike-based speech Brain-inspired auditory recognition systems outperform conventional approaches? processor and the • Book review: Analog VLSI circuits for the perception Artificial Brain project of visual motion The Korean Brain Neuroinformatics Re- search Program has two goals: to under- stand information processing mechanisms in biological brains and to develop intel- ligent machines with human-like functions based on these mechanisms. We are now developing an integrated hardware and software platform for brain-like intelligent systems called the Artificial Brain. It has two microphones, two cameras, and one speaker, looks like a human head, and has the functions of vision, audition, inference, and behavior (see Figure 1). The sensory modules receive audio and video signals from the environment, and perform source localization, signal enhancement, feature extraction, and user recognition in the forward ‘path’. In the backward path, top-down attention is per- formed, greatly improving the recognition performance of real-world noisy speech and occluded patterns. The fusion of audio and visual signals for lip-reading is also influenced by this path. The inference module has a recurrent architecture with internal states to imple- ment human-like emotion and self-esteem. Also, we would like the Artificial Brain to eventually have the abilities to perform user modeling and active learning, as well as to be able to ask the right questions both to the right people and to other Artificial Brains. -

ABS: Scanning Neural Networks for Back-Doors by Artificial Brain
ABS: Scanning Neural Networks for Back-doors by Artificial Brain Stimulation Yingqi Liu Wen-Chuan Lee Guanhong Tao [email protected] [email protected] [email protected] Purdue University Purdue University Purdue University Shiqing Ma Yousra Aafer Xiangyu Zhang [email protected] [email protected] [email protected] Rutgers University Purdue University Purdue University ABSTRACT Kingdom. ACM, New York, NY, USA, 18 pages. https://doi.org/10.1145/ This paper presents a technique to scan neural network based AI 3319535.3363216 models to determine if they are trojaned. Pre-trained AI models may contain back-doors that are injected through training or by 1 INTRODUCTION transforming inner neuron weights. These trojaned models operate Neural networks based artificial intelligence models are widely normally when regular inputs are provided, and mis-classify to a used in many applications, such as face recognition [47], object specific output label when the input is stamped with some special detection [49] and autonomous driving [14], demonstrating their pattern called trojan trigger. We develop a novel technique that advantages over traditional computing methodologies. More and analyzes inner neuron behaviors by determining how output acti- more people tend to believe that the applications of AI models vations change when we introduce different levels of stimulation to in all aspects of life is around the corner [7, 8]. With increasing a neuron. The neurons that substantially elevate the activation of a complexity and functionalities, training such models entails enor- particular output label regardless of the provided input is considered mous efforts in collecting training data and optimizing performance. -
The Project Loon
AISSMS INSTITUTE OF INFORMATION TECHNOLOGY Affiliated to Savitribai Phule Pune University , Approved by AICTE, New Delhi and Recognised by Govt. Of Maharashtra (ID No. PU/PN/ENGG/124/1998) Accredited by NAAC with ‘A’ Grade TELESCAN 2K19 TELESCAN 2019 Editorial Committee We, the students of Electronics & Telecommunication feel the privilege to present the Technical Departmental Magazine of Academic year- TELESCAN 2019 in front of you the magazine provides a platform for the students to express their technical knowledge and enhance their own technical knowledge. We would like to thank Dr.M.P.Sardey (HOD) and Prof. Santosh H Lavate for their constant support and encouraging us throughout the semester to make the magazine great hit. Editorial Team: Staff Co-ordinator: Sanmay Kamble (BE) Santosh H Lavate Abhishek Parte (BE) Supriya Lohar Nehal Gholse (TE) Ankush Muley (TE) TELESCAN 2019 VISION OF E&TC DEPARTMENT To provide quality education in Electronics & Telecommunication Engineering with professional ethics MISSION OF E&TC DEPATMENT To develop technical competency, ethics for professional growth and sense of social responsibility among students TELESCAN 2019 INDEX Sr No. Topic Page No. 1 3 Dimensional Integrated Circuit 1 2 4D Printer 4 3 5 Nanometer Semiconductor 5 4 AI: Changing The Face Of Defence 7 5 Artificial Intelligence 10 6 AI: A Boon Or A Bane 11 7 Block Chain 12 8 Blue Brain 14 9 Cobra Effect 16 10 A New Era In Industrial Production 18 11 Radiometry 20 12 Growing Need For Large Bank Of Test Item 21 13 The Project Loon 23 14 -

Phenotypes and Endotypes of Uncontrolled Severe Asthma
Phenotypes and New Treatments for Severe Asthma REVIEWS Phenotypes and Endotypes of Uncontrolled Severe Asthma: New Treatments P Campo,1 F Rodríguez,2 S Sánchez-García,3 P Barranco,4 S Quirce,4 C Pérez- Francés,5 E Gómez-Torrijos,6 R Cárdenas,6 JM Olaguibel,7 J Delgado8 Severe Asthma Workgroup of the SEAIC Asthma Committee 1UGC Allergy, Hospital General de Málaga, Málaga, Spain 2Department of Allergy, Hospital Universitario Marqués de Valdecilla, Santander, Spain 3Allergy Section, Hospital Infantil Universitario Niño Jesús, Madrid, Spain 4Department of Allergy, Hospital La Paz Institute for Health Research (IdiPAZ), Madrid, Spain 5Department of Allergy, Hospital Universitario Dr. Peset, Valencia, Spain 6Department of Allergy, Hospital General Universitario de Ciudad Real, Ciudad Real, Spain 7Department of Allergy, Complejo Hospitalario de Navarra, Pamplona, Spain 8UGC Allergy, Hospital Universitario Virgen Macarena, Sevilla, Spain ■ Abstract Severe asthma is a heterogeneous disease that affects only 5%-10% of asthmatic patients, although it accounts for a signifi cant percentage of the consumption of health care resources. Severe asthma is characterized by the need for treatment with high doses of inhaled corticosteroids and includes several clinical and pathophysiological phenotypes. To a large extent, this heterogeneity restricts characterization of the disease and, in most cases, hinders the selection of appropriate treatment. In recent years, therefore, emphasis has been placed on improving our understanding of the various phenotypes of severe asthma and the identifi cation of biomarkers for each of these phenotypes. Likewise, the concept of the endotype has been gaining acceptance with regard to the various subtypes of the disease, which are classifi ed according to their unique functional or pathophysiological mechanism. -

An New Type of Artificial Brain Using Controlled Neurons
New Developments in Neural Networks, J. R. Burger An New Type Of Artificial Brain Using Controlled Neurons John Robert Burger, Emeritus Professor, ECE Department, California State University Northridge, [email protected] Abstract -- Plans for a new type of artificial brain are possible because of realistic neurons in logically structured arrays of controlled toggles, one toggle per neuron. Controlled toggles can be made to compute, in parallel, parameters of critical importance for each of several complex images recalled from associative long term memory. Controlled toggles are shown below to amount to a new type of neural network that supports autonomous behavior and action. I. INTRODUCTION A brain-inspired system is proposed below in order to demonstrate the utility of electrically realistic neurons as controlled toggles. Plans for artificial brains are certainly not new [1, 2]. As in other such systems, the system below will monitor external information, analogous to that flowing from eyes, ears and other sensors. If the information is significant, for instance, bright spots, or loud passages, or if identical information is presented several times, it will automatically be committed to associative long term memory; it will automatically be memorized. External information is concurrently impressed on a short term memory, which is a logical row of short term memory neurons. From here cues are derived and held long enough to accomplish a search of associative long term memory. Unless the cues are very exacting indeed, several returned images are expected. Each return then undergoes calculations for priority; an image with maximum priority is imposed on (and overwrites the current contents of) short term memory. -

Is Google Making Us Stupid?
Is Google Making Us Stupid? What the Internet is doing to our brains Nicholas Carr Jul 1 2008, 12:00 PM ET "Dave, stop. Stop, will you? Stop, Dave. Will you stop, Dave?” So the supercomputer HAL pleads with the implacable astronaut Dave Bowman in a famous and weirdly poignant scene toward the end of Stanley Kubrick’s 2001: A Space Odyssey. Bowman, having nearly been sent to a deep-space death by the malfunctioning machine, is calmly, coldly disconnecting the memory circuits that control its artificial “ brain. “Dave, my mind is going,” HAL says, forlornly. “I can feel it. I can feel it.” I can feel it, too. Over the past few years I’ve had an uncomfortable sense that someone, or something, has been tinkering with my brain, remapping the neural circuitry, reprogramming the memory. My mind isn’t going—so far as I can tell—but it’s changing. I’m not thinking the way I used to think. I can feel it most strongly when I’m reading. Immersing myself in a book or a lengthy article used to be easy. My mind would get caught up in the narrative or the turns of the argument, and I’d spend hours strolling through long stretches of prose. That’s rarely the case anymore. Now my concentration often starts to drift after two or three pages. I get fidgety, lose the thread, and begin looking for something else to do. I feel as if I’m always dragging my wayward brain back to the text. The deep reading that used to come naturally has become a struggle. -

Identifying Pathophysiological Bases of Disease in COVID-19 Carla J
Goldin et al. Translational Medicine Communications (2020) 5:15 Translational Medicine https://doi.org/10.1186/s41231-020-00067-w Communications REVIEW Open Access Identifying pathophysiological bases of disease in COVID-19 Carla J. Goldin1,2, Ramiro Vázquez3,4, Fernando P. Polack1 and Damian Alvarez-Paggi1,2* Abstract COVID-19 is an infectious disease caused by the SARS-CoV-2 virus that can affect lung physiology encompassing a wide spectrum of severities, ranging from asymptomatic and mild symptoms to severe and fatal cases; the latter including massive neutrophil infiltration, stroke and multiple organ failure. Despite many recents findings, a clear mechanistic description underlying symptomatology is lacking. In this article, we thoroughly review the available data involving risk factors, age, gender, comorbidities, symptoms of disease, cellular and molecular mechanisms and the details behind host/pathogen interaction that hints at the existence of different pathophysiological mechanisms of disease. There is clear evidence that, by targeting the angiotensin-converting enzyme II (ACE2) –its natural receptor–, SARS-CoV-2 would mainly affect the renin- angiotensin-aldosterone system (RAAS), whose imbalance triggers diverse symptomatology-associated pathological processes. Downstream actors of the RAAS cascade are identified, and their interaction with risk factors and comorbidities are presented, rationalizing why a specific subgroup of individuals that present already lower ACE2 levels is particularly more susceptible to severe forms of disease. Finally, the notion of endotype discovery in the context of COVID-19 is introduced. We hypothesize that COVID-19, and its associated spectrum of severities, is an umbrella term covering different pathophysiological mechanisms (endotypes). This approach should dramatically accelerate our understanding and treatment of disease(s), enabling further discovery of pathophysiological mechanisms and leading to the identification of specific groups of patients that may benefit from personalized treatments. -

A World Survey of Artificial Brain Projects, Part II Biologically Inspired
Neurocomputing 74 (2010) 30–49 Contents lists available at ScienceDirect Neurocomputing journal homepage: www.elsevier.com/locate/neucom A world survey of artificial brain projects, Part II: Biologically inspired cognitive architectures Ben Goertzel a,b,n, Ruiting Lian b, Itamar Arel c, Hugo de Garis b, Shuo Chen b a Novamente LLC, 1405 Bernerd Place, Rockville, MD 20851, USA b Fujian Key Lab of the Brain-like Intelligent Systems, Xiamen University, Xiamen, China c Machine Intelligence Lab, Department of Electrical Engineering and Computer Science, University of Tennessee, Knoxville, USA article info abstract Available online 18 September 2010 A number of leading cognitive architectures that are inspired by the human brain, at various levels of Keywords: granularity, are reviewed and compared, with special attention paid to the way their internal structures Artificial brains and dynamics map onto neural processes. Four categories of Biologically Inspired Cognitive Cognitive architectures Architectures (BICAs) are considered, with multiple examples of each category briefly reviewed, and selected examples discussed in more depth: primarily symbolic architectures (e.g. ACT-R), emergentist architectures (e.g. DeSTIN), developmental robotics architectures (e.g. IM-CLEVER), and our central focus, hybrid architectures (e.g. LIDA, CLARION, 4D/RCS, DUAL, MicroPsi, and OpenCog). Given the state of the art in BICA, it is not yet possible to tell whether emulating the brain on the architectural level is going to be enough to allow rough emulation of brain function; and given the state of the art in neuroscience, it is not yet possible to connect BICAs with large-scale brain simulations in a thoroughgoing way. -

Sigg, Stephan a Global Brain Fuelled by Local Intelligence
This is an electronic reprint of the original article. This reprint may differ from the original in pagination and typographic detail. Naas, Si Ahmed; Mohammed, Thaha; Sigg, Stephan A global brain fuelled by local intelligence Published in: Proceedings of 16th International Conference on Mobility, Sensing and Networking (MSN 2020) DOI: 10.1109/MSN50589.2020.00021 Published: 01/04/2021 Document Version Peer reviewed version Please cite the original version: Naas, S. A., Mohammed, T., & Sigg, S. (2021). A global brain fuelled by local intelligence: Optimizing mobile services and networks with AI. In Proceedings of 16th International Conference on Mobility, Sensing and Networking (MSN 2020) (pp. 23-32). [9394314] IEEE. https://doi.org/10.1109/MSN50589.2020.00021 This material is protected by copyright and other intellectual property rights, and duplication or sale of all or part of any of the repository collections is not permitted, except that material may be duplicated by you for your research use or educational purposes in electronic or print form. You must obtain permission for any other use. Electronic or print copies may not be offered, whether for sale or otherwise to anyone who is not an authorised user. Powered by TCPDF (www.tcpdf.org) © 2020 IEEE. This is the author’s version of an article that has been published by IEEE. Personal use of this material is permitted. Permission from IEEE must be obtained for all other uses, in any current or future media, including reprinting/republishing this material for advertising or promotional purposes, creating new collective works, for resale or redistribution to servers or lists, or reuse of any copyrighted component of this work in other works. -

Endotype Clustering in Chronic Rhinosinusitis Based on the Chemokine Expression Pattern
Endotype clustering in chronic rhinosinusitis based on the chemokine expression pattern Ulrike F¨orster-Ruhrmann1, Greta Pierchalla1, Agnieszka Szczepek2, Joachim Fluhr1, Metin Artuc1, Torsten Zuberbier1, Claus Bachert3, and Heidi Olze1 1Charit´eUniversit¨atsmedizinBerlin 2Charite Universitatsmedizin Berlin 3University Hospital Ghent May 11, 2020 Abstract Background: Chronic rhinosinusitis with and without nasal polyps (CRSwNP/ CRSsNP) is an inflammatory disease affecting the nasal and sinus mucosal lining. Here, to further characterize this heterogeneous disease, we performed an extended endotyping of CRS using the nasal tissue from CRS-patients and a new approach of expression profiling of chemokines related to Th2- type cytokine IL-5. Methods: In this case-control study, we included 66 patients with CRS (CRSwNP n=26; CRSsNP n=40) diagnosed according to the EPOS 2020 criteria. The control group (n=25) consisted of CRS-free patients scheduled for inferior turbinate surgery. The concentration of following chemokines and cytokines was determined in tissue samples obtained during routine surgery from all subjects: TARC/ CCL17, PARC/ CCL18, eotaxin/ CCL11, MCP-3/ CCL7, MIP-1a/ CCL3, IP-10/ CXCL10, ENA-78/ CCL5, and IL-5. The analysis was performed by partition-based clustering. Results: In CRS tissues, the concentration of eotaxin, TARC, total IgE, IL-5, and ECP was significantly higher than in control (p<0.005). The analysis identified seven clusters. Cluster-1 was IL-5- and inflammatory chemokines-negative (11% CRSwNP). Cluster-2 had low IL-5 concentration and elevated MCP-3/CCL7 (100% CRSsNP). Clusters -3 and -4 expressed IP-10/CXCL10 (type-1-dominated), TARC/CCL17 and eotaxin/CCL11 (both type-2-dominated) (CRSwNP 13-31%). -

Upgrading Human Brain to Blue Brain
dicine e & N om a n n a o t N e f c o h Ganji and Nayana, J Nanomed Nanotechnol 2015, 6:3 l n Journal of a o n l o r g u DOI: 10.4172/2157-7439.1000287 y o J ISSN: 2157-7439 Nanomedicine & Nanotechnology Short Communication Open Access Upgrading Human Brain to Blue Brain Shruti Ganji* and Kamala Nayana Department of Information Technology (3/4), M.V.S.R Engineering College, Saroornagar Mandal, Nadargul, Hyderabad, Telangana 501510, India Abstract Blue brain is the name given to the world’s first virtual brain. That means a machine that can function as human brain. There is an attempt to create an artificial brain that can think, response, take decision, and keep anything in memory. The most important thing is to upload the contents of the normal brain into the computer or virtual brain with help of nanobots. Keywords: Blue; Virtual; Artificial brain; Nanobots Introduction In future, our brains are going to be attacked by the blue brain!! Yeah that’s right, but there is nothing to be worried, as it is going to be really useful for us. As sir Isaac Newton once said that we are like small kids on the sea shore, who are getting curious and excited by finding sea shells and fossils, but beyond the beach there is a huge ocean with diverse creatures and things yet to be discovered. Similarly he wants to say that in the field of technology, there are many things to be invented that might bring a drastic change in the field of science and technology [1].