Readingsample
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lecture Notes on Human Anatomy. Part One, Fourth Edition. PUB DATE Sep 89 NOTE 79P.; for Related Documents, See SE 051 219-221
DOCUMENT RESUME ED 315 320 SE 051 218 AUTHOR Conrey, Kathleen TITLE Lecture Notes on Human Anatomy. Part One, Fourth Edition. PUB DATE Sep 89 NOTE 79p.; For related documents, see SE 051 219-221. Black and white illustrations will not reproduce clearly. AVAILABLE FROM Aramaki Design and Publications, 12077 Jefferson Blvd., Culver City, CA 90506 ($7.75). PUB TYPE Guides - Classroom Use - Materials (For Learner) (051) EDRS PRICE MF01 Plus Postage. PC Not Available from EDRS. DESCRIPTORS *Anatomy; *Biological Sciences; *College Science; Higher Education; *Human Body; *Lecture Method; Science Education; Secondary Education; Secondary School Science; Teaching Guides; Teaching Methods ABSTRACT During the process of studying the specific course content of human anatomy, students are being educated to expand their vocabulary, deal successfully with complex tasks, anduse a specific way of thinking. This is the first volume in a set of notes which are designed to accompany a lecture series in human anatomy. This volume Includes discussions of anatomical planes and positions, body cavities, and architecture; studies of the skeleton including bones and joints; studies of the musculature of the body; and studiesof the nervous system including the central, autonomic, motor and sensory systems. (CW) *****1.**k07********Y*******t1.****+***********,****A*******r****** % Reproductions supplied by EDRS are the best that can be made from the original document. **************************************************************A**t***** "PERMISSION TO REPRODUCE -

38.3 Joints and Skeletal Movement.Pdf
1198 Chapter 38 | The Musculoskeletal System Decalcification of Bones Question: What effect does the removal of calcium and collagen have on bone structure? Background: Conduct a literature search on the role of calcium and collagen in maintaining bone structure. Conduct a literature search on diseases in which bone structure is compromised. Hypothesis: Develop a hypothesis that states predictions of the flexibility, strength, and mass of bones that have had the calcium and collagen components removed. Develop a hypothesis regarding the attempt to add calcium back to decalcified bones. Test the hypothesis: Test the prediction by removing calcium from chicken bones by placing them in a jar of vinegar for seven days. Test the hypothesis regarding adding calcium back to decalcified bone by placing the decalcified chicken bones into a jar of water with calcium supplements added. Test the prediction by denaturing the collagen from the bones by baking them at 250°C for three hours. Analyze the data: Create a table showing the changes in bone flexibility, strength, and mass in the three different environments. Report the results: Under which conditions was the bone most flexible? Under which conditions was the bone the strongest? Draw a conclusion: Did the results support or refute the hypothesis? How do the results observed in this experiment correspond to diseases that destroy bone tissue? 38.3 | Joints and Skeletal Movement By the end of this section, you will be able to do the following: • Classify the different types of joints on the basis of structure • Explain the role of joints in skeletal movement The point at which two or more bones meet is called a joint, or articulation. -

Gen Anat-Joints
JOINTS Joint is a junction between two or more bones Classification •Functional Based on the range and type of movement they permit •Structural On the basis of their anatomic structure Functional Classification • Synarthrosis No movement e.g. Fibrous joint • Amphiarthrosis Slight movement e.g. Cartilagenous joint • Diarthrosis Movement present Cavity present Also called as Synovial joint eg.shoulder joint Structural Classification Based on type of connective tissue binding the two adjacent articulating bones Presence or absence of synovial cavity in between the articulating bone • Fibrous • Cartilagenous • Synovial Fibrous Joint Bones are connected to each other by fibrous (connective ) tissue No movement No synovial cavity • Suture • Syndesmosis • Gomphosis Sutural Joints • A thin layer of dens fibrous tissue binds the adjacent bones • These appear between the bones which ossify in membrane • Present between the bones of skull e.g . coronal suture, sagittal suture • Schindylesis: – rigid bone fits in to a groove on a neighbouring bone e.g. Vomer and sphenoid Gomphosis • Peg and socket variety • Cone shaped root of tooth fits in to a socket of jaw • Immovable • Root is attached to the socket by fibrous tissue (periodontal ligament). Syndesmosis • Bony surfaces are bound together by interosseous ligament or membrane • Membrane permits slight movement • Functionally classified as amphiarthrosis e.g. inferior tibiofibular joint Cartilaginous joint • Bones are held together by cartilage • Absence of synovial cavity . Synchondrosis . Symphysis Synchondrosis • Primary cartilaginous joint • Connecting material between two bones is hyaline cartilage • Temporary joint • Immovable joint • After a certain age cartilage is replaced by bone (synostosis) • e.g. Epiphyseal plate connecting epiphysis and diphysis of a long bone, joint between basi-occiput and basi-sphenoid Symphysis • Secondary cartilaginous joint (fibrocartilaginous joint) • Permanent joint • Occur in median plane of the body • Slightly movable • e.g. -

RADIOULNAR JOINTS the Radius and Ulna Articulate by –
RADIOULNAR JOINTS The radius and ulna articulate by – • Synovial 1. Superior radioulnar joint 2. Inferior radioulnar joint • Non synovial Middle radioulnar union Superior Radioulnar Joint This articulation is a trochoid or pivot-joint between • the circumference of the head of the radius • ring formed by the radial notch of the ulna and the annular ligament. The Annular Ligament (orbicular ligament) This ligament is a strong band of fibers, which encircles the head of the radius, and retains it in contact with the radial notch of the ulna. It forms about four-fifths of the osseo- fibrous ring, and is attached to the anterior and posterior margins of the radial notch a few of its lower fibers are continued around below the cavity and form at this level a complete fibrous ring. Its upper border blends with the capsule of elbow joint while from its lower border a thin loose synovial membrane passes to be attached to the neck of the radius The superficial surface of the annular ligament is strengthened by the radial collateral ligament of the elbow, and affords origin to part of the Supinator. Its deep surface is smooth, and lined by synovial membrane, which is continuous with that of the elbow-joint. Quadrate ligament A thickened band which extends from the inferior border of the annular ligament below the radial notch to the neck of the radius is known as the quadrate ligament. Movements The movements allowed in this articulation are limited to rotatory movements of the head of the radius within the ring formed by the annular ligament and the radial notch of the ulna • rotation forward being called pronation • rotation backward, supination Middle Radioulnar Union The shafts of the radius and ulna are connected by Oblique Cord and Interosseous Membrane The Oblique Cord (oblique ligament) The oblique cord is a small, flattened band, extending downward and laterally, from the lateral side of the ulnar tuberosity to the radius a little below the radial tuberosity. -
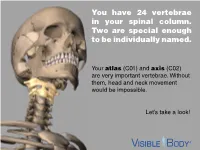
You Have 24 Vertebrae in Your Spinal Column. Two Are Special Enough to Be Individually Named
You have 24 vertebrae in your spinal column. Two are special enough to be individually named. Your atlas (C01) and axis (C02) are very important vertebrae. Without them, head and neck movement would be impossible. Let’s take a look! The atlas and axis are the most superior bones in the cervical vertebrae. The atlas is the top-most vertebra, sitting just below the skull. The axis is below it. Together, the atlas and axis support the skull, facilitate head and neck movement, and protect the spinal cord. (Think of the atlas and axis as best buds for life. You will never find one without the other.) www.visiblebody.com There are many types of vertebral joints, but the atlas and axis form the only craniovertebral joints in the human body. A craniovertebral joint is a joint that permits movement between the cervical vertebrae and the neurocranium. The atlanto-occipital joint (pictured) connects the atlas to the occipital bone. It flexes the neck, allowing you to nod your head. The atlanto-axial joint connects the axis to the atlas. It permits rotational movement of the head. www.visiblebody.com The atlanto-axial joint is a compound synovial joint. This pivot joint allows for rotation of the head and neck. Watch this joint in action! A pivot joint is made by the end of one articulating bone rotating in a ring formed by another bone and its ligaments. www.visiblebody.com The atlas and axis are part of the seven cervical vertebrae. These vertebrae have a few unique features: They are the smallest of the vertebrae. -

Structural Kinesiology (PDF)
Kinesiology & Body Mechanics • Kinesiology - study of motion or human movement • Anatomic kinesiology - study of human Chapter 1 musculoskeletal system & musculotendinous system Foundations of Structural Kinesiology • Biomechanics - application of mechanical physics to human motion Manual of Structural Kinesiology R.T. Floyd, EdD, ATC, CSCS Manual of Manual of Structural Kinesiology Foundations of Structural Kinesiology 1-1 Structural Kinesiology Foundations of Structural Kinesiology 1-2 Kinesiology & Body Mechanics Kinesiology & Body Mechanics • Structural kinesiology - study of muscles as • Muscles vary greatly in size, shape, & they are involved in science of movement structure from one part of body to another • Both skeletal & muscular structures are • More than 600 muscles are found in human involved body • Bones are different sizes & shapes − particularly at the joints, which allow or limit movement Manual of Manual of Structural Kinesiology Foundations of Structural Kinesiology 1-3 Structural Kinesiology Foundations of Structural Kinesiology 1-4 Who needs Kinesiology? Why Kinesiology? • Anatomists, coaches, strength and • should have an adequate knowledge & understanding of all large muscle groups to conditioning specialists, personal teach others how to strengthen, improve, & trainers, nurses, physical educators, maintain these parts of human body physical therapists, physicians, athletic • should not only know how & what to do in trainers, massage therapists & others in relation to conditioning & training but also know health-related -

Self Quiz Chapter 9 (Joints) Anatomy & Physiology I
Self Quiz Chapter 9 (Joints) Anatomy & Physiology I Pro: Manhal Chbat 1. Which of the following is a functional classification of joints and applies to joints that allow a wide range of motion? A) amphiarthrosis B) diarthrosis C) synarthrosis D) fibrous E) cartilaginous 2. Consider the anatomy of the pubic bones. They are joined by cartilage and allow limited movement. Their junction is classified as a(n): A) amphiarthrosis. B) cartilaginous joint. C) synarthrosis D) A and B are correct. E) A, B, and C are correct. 3. Which of the following is an example of a synarthrosis? A) a suture in the skull B) the vertebral column C) the atlanto-occipital joint D) the knee E) the elbow 4. The synovial membrane A) is the inner layer of the articular capsule. B) consists of columnar epithelial cells. C) makes mucous to lubricate the joints. D) includes accumulations of dense connective tissue. E) All of the above are correct. 5. Synovial fluid A) lubricates diarthrotic joints. B) helps absorb mechanical shocks. C) brings nutrients and O2 to cartilage in diarthroses. D) removes wastes and CO2 from cartilages in diarthroses. E) All of the above are correct. 6. Mensici A) are pads of hyaline cartilage. B) help bones fit together more closely. C) help decrease the stability of a joint. D) block the flow of synovial fluid within a joint. E) All of the above are correct. 7. Bursae A) are fat-filled sacs. B) are integral parts of the articular capsule. C) are never observed between ligaments and bones. D) help reduce friction between moving parts. -

Current Perspectives in Conventional and Advanced Imaging of the Distal Radioulnar Joint Dysfunction: Review for the Musculoskeletal Radiologist
Skeletal Radiology (2019) 48:331–348 https://doi.org/10.1007/s00256-018-3042-1 REVIEW ARTICLE Current perspectives in conventional and advanced imaging of the distal radioulnar joint dysfunction: review for the musculoskeletal radiologist Aishwarya Gulati1 & Vibhor Wadhwa2 & Oganes Ashikyan3 & Luis Cerezal4 & Avneesh Chhabra3,5,6 Received: 25 December 2017 /Revised: 27 July 2018 /Accepted: 1 August 2018 /Published online: 1 September 2018 # ISS 2018 Abstract Distal radioulnar joint (DRUJ) dysfunction is a common cause of ulnar sided wrist pain. Physical examination yields only subtle clues towards the underlying etiology. Thus, imaging is commonly obtained towards an improved characterization of DRUJ pathology, especially multimodality imaging, which is frequently resorted to arrive at an accurate diagnosis. With increasing use of advanced MRI and CT techniques, DRUJ imaging has become an important part of a musculoskeletal radiologist’s practice. This article discusses the normal anatomy and biomechanics of the DRUJ, illustrates common clinical abnormalities, and provides a comprehensive overview of the imaging evaluation with an insight into the role of advanced cross-sectional modalities in this domain. Keywords Distal radioulnar joint . DRUJ . Instability . CT . MRI . Dynamic imaging Introduction in cartilage loss and bone erosions, ligament abnormalities, altered kinetics in the setting of instability, and occult frac- The distal radioulnar joint (DRUJ) is the distal articulation tures, among others [4–6]. Understanding the details of anat- between the radius and ulna. It is a major weight-bearing joint omy and mechanics of the DRUJ is an important prerequisite at the wrist, which distributes forces across the forearm bones to the systematic image interpretation. -

Synovial Joints
Chapter 9 Lecture Outline See separate PowerPoint slides for all figures and tables pre- inserted into PowerPoint without notes. Copyright © McGraw-Hill Education. Permission required for reproduction or display. 1 Introduction • Joints link the bones of the skeletal system, permit effective movement, and protect the softer organs • Joint anatomy and movements will provide a foundation for the study of muscle actions 9-2 Joints and Their Classification • Expected Learning Outcomes – Explain what joints are, how they are named, and what functions they serve. – Name and describe the four major classes of joints. – Describe the three types of fibrous joints and give an example of each. – Distinguish between the three types of sutures. – Describe the two types of cartilaginous joints and give an example of each. – Name some joints that become synostoses as they age. 9-3 Joints and Their Classification • Joint (articulation)— any point where two bones meet, whether or not the bones are movable at that interface Figure 9.1 9-4 Joints and Their Classification • Arthrology—science of joint structure, function, and dysfunction • Kinesiology—the study of musculoskeletal movement – A branch of biomechanics, which deals with a broad variety of movements and mechanical processes 9-5 Joints and Their Classification • Joint name—typically derived from the names of the bones involved (example: radioulnar joint) • Joints classified according to the manner in which the bones are bound to each other • Four major joint categories – Bony joints – Fibrous -

Synovial Joints • Typically Found at the Ends of Long Bones • Examples of Diarthroses • Shoulder Joint • Elbow Joint • Hip Joint • Knee Joint
Chapter 8 The Skeletal System Articulations Lecture Presentation by Steven Bassett Southeast Community College © 2015 Pearson Education, Inc. Introduction • Bones are designed for support and mobility • Movements are restricted to joints • Joints (articulations) exist wherever two or more bones meet • Bones may be in direct contact or separated by: • Fibrous tissue, cartilage, or fluid © 2015 Pearson Education, Inc. Introduction • Joints are classified based on: • Function • Range of motion • Structure • Makeup of the joint © 2015 Pearson Education, Inc. Classification of Joints • Joints can be classified based on their range of motion (function) • Synarthrosis • Immovable • Amphiarthrosis • Slightly movable • Diarthrosis • Freely movable © 2015 Pearson Education, Inc. Classification of Joints • Synarthrosis (Immovable Joint) • Sutures (joints found only in the skull) • Bones are interlocked together • Gomphosis (joint between teeth and jaw bones) • Periodontal ligaments of the teeth • Synchondrosis (joint within epiphysis of bone) • Binds the diaphysis to the epiphysis • Synostosis (joint between two fused bones) • Fusion of the three coxal bones © 2015 Pearson Education, Inc. Figure 6.3c The Adult Skull Major Sutures of the Skull Frontal bone Coronal suture Parietal bone Superior temporal line Inferior temporal line Squamous suture Supra-orbital foramen Frontonasal suture Sphenoid Nasal bone Temporal Lambdoid suture bone Lacrimal groove of lacrimal bone Ethmoid Infra-orbital foramen Occipital bone Maxilla External acoustic Zygomatic -

Module Two: Anatomy of the Athlete
Module Two: Anatomy of the Athlete INTRODUCTION The Level One course provided you with basic information about the skeletal and muscular systems of the body. This module studies these systems in more depth, applies this knowledge to the analysis of human movement, and looks at the application of analysis results to the development of conditioning programmes for athletes. Upon completion of this module, you will be able to: EXPLAIN THE STRUCTURE AND FUNCTIONS OF THE SKELETAL SYSTEM UNDERSTAND THE STRUCTURE OF JOINTS AND THE MOVEMENTS POSSIBLE AT SYNOVIAL JOINTS EXPLAIN THE STRUCTURE AND FUNCTIONS OF THE MUSCULAR SYSTEM EXPLAIN MUSCLE ACTION IN THE HUMAN BODY APPLY YOUR KNOWLEDGE OF THE SKELETAL AND MUSCULAR SYSTEMS TO ANALYSE MUSCLE ACTION EXPLAIN THE STRUCTURE AND FUNCTIONS OF THE SKELETAL SYSTEM THE SKELETAL SYSTEM The framework of the human body is made up of just over 200 bones, which vary considerably in size and shape. Bones are often thought of as dry, inert structures, similar to a bone which has been dug up in the garden by the neighbour’s dog! However, bone is not a dead structure. It is made up of living bone tissue, which is a type of connective tissue, the hardest of all connective tissues found in the body. FUNCTIONS OF THE SKELETON The skeleton has five important functions in the body: 1. Protection The bones protect internal organs by forming strong protective enclosures, e.g. skull, ribs, spine. 2. Support The skeleton gives rigidity to the body. Without the support of the skeleton, we would be shapeless lumps. 3. -
Functional Morphology of a Highly Specialised Pivot Joint in the Cranio
Contributions to Zoology, 84 (1) 13-23 (2015) Functional morphology of a highly specialised pivot joint in the cranio-cervical complex of the minute lizard Ablepharus kitaibelii in relation to feeding ecology and behaviour Nikolay Natchev1, 2, 7, Nikolay Tzankov3, Vladislav Vergilov4, Stefan Kummer5, Stephan Handschuh5, 6 1 Department Integrative Zoology, University of Vienna, Althanstrasse 14, 1090 Vienna, Austria 2 Faculty of Natural Science, Shumen University, Universitetska 115/313, 9700 Shumen, Bulgaria 3 Section Vertebrates, National Museum of Natural History, Bulgarian Academy of Sciences, Tzar Osvoboditel 1, 1000 Sofia, Bulgaria 4 Department of Anthropology and Zoology, Sofia University, Dragan Tzankov 8, 1164 Sofia, Bulgaria 5 VetCore Facility for Research, University of Veterinary Medicine Vienna, Veterinärplatz 1, 1210 Vienna, Austria 6 Department of Theoretical Biology, University of Vienna, Althanstrasse 14, 1090 Vienna, Austria 7 E-mail: [email protected] Key words: evolution, feeding, neck, odontoid, parallel, skink, µCT Abstract Morphology of the cranio-cervical-joint ...................................... 17 Discussion .................................................................................................................. 17 The snake-eyed skink Ablepharus kitaibelii is one of the small- Analysis of diet ............................................................................................... 17 est European lizards, but despite its minute size it is able to feed Feeding kinematics and morphology