Sightsavers Yaoundé - Cameroon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
[email protected] Telephone: (237) 675184310, 697037417 Address: P.O
Website: www.camgew.com or www.camgew.org Email:[email protected]; [email protected] Telephone: (237) 675184310, 697037417 Address: P.O. Box 17 OKU-Bui Division, North West Region, Cameroon CAMGEW’s authorisation number N° 000998/RDA/JO6/ BAPP Report prepared by WIRSIY EMMANUEL BINYUY (CAMGEW Director) with support from Ngum Jai Raymond (CAMGEW Project Officer) and Sevidzem Ernestine Leikeki (CAMGEW Social Project Officer). 1 PREFACE Our world needs creative and innovative actions to make it a better place for all its occupants. The environment needs to be kept healthy for mankind to be healthy. Poverty, hunger and unemployment have stood as major challenges to mankind. The economic, environmental, political and social conditions are not making things better. We have talked about North-South partnership to make things better for the developing countries and we have also promoted south-south cooperation too but things are not changing positively as expected. Our continent- Africa has a lot of natural resources but these natural resources have not been able to help Africans get decent jobs, put food on their tables, meet other daily needs and invest in the future. There is much disparity between the rich and the poor, the able and the disable, the people in power and those being ruled, the land owners and those in need of land, etc. How do we develop an inclusive strategy that will make everyone belonging to the society? We just hope that as the Sustainable Development Goals (SDGs) have been developed to replace the expired MDGs things will be getting better globally. -

Dictionnaire Des Villages Du Fako : Village Dictionary of Fako Division
OFFICE DE LA RECHERCHE SCIENTIFIOUE ET TECHNIOUE OUTRE· MER Il REPUBLIQUE UNIE DU CAMEROUN DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION SECTION DE GEOGRAPHIE 1 OFFICE DE LA RECHERCHE SCIm~TIFIQUE REPUBLIQUE UNIE ET TECmUQUE OUTRE-lViER DU CAlvŒROUN UNITED REPUBLIC OF CANEROON CENTRE O.R.S.T.O.N DE YAOUNDE DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION Juillet 1973 July 1973 COPYRIGHT O.R.S.T.O.M 1973 TABLE DES NATIERES CONTENTS i l j l ! :i i ~ Présentation •••••.•.•.....••....•.....•....••••••.••.••••••.. 1 j Introduction ........................................•• 3 '! ) Signification des principaux termes utilisés •.............• 5 î l\lIeaning of the main words used Tableau de la population du département •...••.....•..•.•••• 8 Population of Fako division Département du Fako : éléments de démographie •.•.... ..••.•• 9 Fako division: demographic materials Arrondissements de Muyuka et de Tiko : éléments de . démographie 0 ••••••••••••••••••••••••••••••••••••••• 10 11uyul{a and Tileo sl)..bdivisions:demographic materials Arrondissement de Victoria: éléments de démographie •••.••• 11 Victoria subdivision:demographic materials Les plantations (12/1972) •••••••••••.•••••••••••••••••••••• 12 Plantations (12/1972) Liste des villages par arrondissement, commune et graupement 14 List of villages by subdivision, area council and customary court Signification du code chiffré •..•••...•.•...•.......•.•••.• 18 Neaning of the code number Liste alphabétique des villages ••••••.••••••••.•.•..•••.•.• 19 -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -
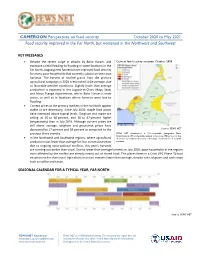
CAMEROON Perspectives on Food Security October 2020 to May 2021 Food Security Improved in the Far North, but Worsened in the Northwest and Southwest
CAMEROON Perspectives on food security October 2020 to May 2021 Food security improved in the Far North, but worsened in the Northwest and Southwest KEY MESSAGES • Despite the recent surge in attacks by Boko Haram, and Current food security situation, October 2020 excessive rainfall leading to flooding in some locations in the Far North, ongoing new harvests have improved food security for many poor households that currently subsist on their own harvests. The harvest of rainfed grains from the primary agricultural campaign in 2020 is estimated to be average, due to favorable weather conditions. Slightly lower than average production is expected in the Logone-et-Chari, Mayo Sava, and Mayo Tsanga departments, where Boko Haram is most active, as well as in locations where harvests were lost to flooding. • Current prices at the primary markets in the Far North appear stable or are decreasing. Since July 2020, staple food prices have increased above typical levels. Sorghum and maize are selling at 46 to 60 percent, and 30 to 47 percent higher (respectively) than in July 2019. Although current prices are still above average, sorghum and groundnut prices have decreased by 17 percent and 18 percent as compared to the Source: FEWS NET previous three months. FEWS NET classification is IPC-compatible (Integrated Phase Classification). IPC-compatible analysis follows key IPC protocols but • In the Northwest and Southwest regions, where agricultural does not necessarily reflect the consensus of national food security production was lower than average for four consecutive years partners. due to ongoing socio-political conflicts, this year's harvests are running out earlier than usual. -
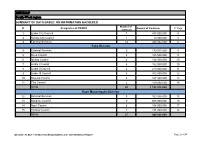
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Limbe City Council 7 475 000 000 4 2 Kumba City Council 1 10 000 000 5 3 External Services 14 440 032 000 6 Fako Division 4 External Services 9 179 015 000 8 5 Buea Council 5 125 500 000 9 6 Idenau Council 4 124 000 000 10 7 Limbe I Council 4 152 000 000 10 8 Limbe II Council 4 219 000 000 11 9 Limbe III Council 6 102 500 000 12 10 Muyuka Council 6 127 000 000 13 11 Tiko Council 5 159 000 000 14 TOTAL 43 1 188 015 000 Kupe Muanenguba Division 12 External Services 5 100 036 000 15 13 Bangem Council 9 605 000 000 15 14 Nguti Council 6 104 000 000 17 15 Tombel Council 7 131 000 000 18 TOTAL 27 940 036 000 MINMAP / PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION Page 1 of 34 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Lebialem Division 16 External Services 5 134 567 000 19 17 Alou Council 9 144 000 000 19 18 Menji Council 3 181 000 000 20 19 Wabane Council 9 168 611 000 21 TOTAL 26 628 178 000 Manyu Division 18 External Services 5 98 141 000 22 19 Akwaya Council 6 119 500 000 22 20 Eyomojock Council 6 119 000 000 23 21 Mamfe Council 5 232 000 000 24 22 Tinto Council 6 108 000 000 25 TOTAL 28 676 641 000 Meme Division 22 External Services 5 85 600 000 26 23 Mbonge Council 7 149 000 000 26 24 Konye Council 1 27 000 000 27 25 Kumba I Council 3 65 000 000 27 26 Kumba II Council 5 83 000 000 28 27 Kumba III Council 3 84 000 000 28 TOTAL 24 493 600 000 MINMAP / PUBLIC CONTRACTS -

(Central Domain of the Cameroon North Equatorial Fold Belt): PT Data
JOURNAL OF THE CAMEROON ACADEMY OF SCIENCES Vol. 8 No. 2/3 (2009) Neoproterozoic metamorphic events in the kekem area (central domain of the Cameroon north equatorial fold belt): P-T data. TCHAPTCHET TCHATO D.c, NZENTI P. a, NJIOSSEU E. L.a, NGNOTUE, T.b, GANNO S.a a Laboratory of Structural Geology and Petrology of Orogenic Domains (LPGS), Department of Earth Sciences, Faculty of Sciences, P.O.Box 812, University of Yaoundé I, Cameroon. b Department of Earth Sciences, Faculty of Sciences, University of Dschang, Cameroon. c Laboratoire d’analyse des matériaux (MIPROMALO), B.P. 2396 Yaoundé. ABSTRACT The Kekem area (southwestern part of the central domain of the Cameroon North Equatorial Fold Belt) is composed of high-grade migmatitic gneisses in which two lithological units are distinguished: (i) a metasedimentary unit (garnet- sillimanite-biotite-gneisses and garnet-biotite-gneisses) interpreted as a continental series; and (ii) meta-igneous rocks comprising mafic pyroxene gneisses, amphibolites, and orthogneisses. These units recrystallised under HT-MP conditions (T=700-800°C, P ≥ 0.5-0.8GPa) and were deformed in relation to a major tangential tectonic event with the NNE-SSW kinematic direction. The lithological association and its tectono-metamorphic evolution show striking similarities with the Banyo and Maham III gneisses, suggesting that the extensional depositional environment envisaged for this formation can be extended farther west. P-T calculations in this contribution provide new data on the Pan-African structural and metamorphic evolution of the metapelites and metabasites in the basement of the Kekem area. The results show two distinct events: (1) crystallization during a Pan-African high temperature metamorphic event and, (2) subsequent deformation and high temperature mylonitization. -

2.3M 1.4M 679K 204K 58.1K
CAMEROON: North-West and South-West Situation Report No. 19 As of 31 May 2020 This report is produced by OCHA Cameroon in collaboration with humanitarian partners. It covers 1 – 31 May 2020. The next report will be issued in July 2020. MAY 2020 HIGHLIGHTS • An estimated 83,557 pupils and students are eligible to sit for end of cycle exams in 2020. • 16 out of the 37 health districts in the North-West and South-West (NWSW) have confirmed cases of COVID-19. • A cholera outbreak is reported in Tiko and Limbe health districts in the South West. • UNICEF supported the establishment of ten in-patient facilities in NWSW for the management of severe acute malnutrition (SAM) cases with complications. • UNHCR and partner have acquired land to build temporal IDP shelter in some locations in the SW. • OCHA and UNICEF supported a joint cluster led training of 81 front- line NGO staff on transmission, signs, symptoms and prevention of COVID-19 in the NW Region. Source: OCHA • IRC constructed 5 boreholes, rehabilitated 20 water distribution The boundaries and names shown and the designations used on systems and constructed 18 tank bases and tap stands, resulting in this map do not imply official endorsement or acceptance by the an 82.4% increase in water supply coverage compared to April. United Nations. 2.3M 1.4M 679K 204K 58.1K affected people targeted for internally displaced (IDP) Returnees (former Cameroonian assistance IDP) Refugees and Asylum seekers in Nigeria Sources: Sources: Sources: Sources: Sources: Humanitarian Need Humanitarian MSNA in -

206 Villages Burnt in the North West and South West Regions
CHRDA Email: [email protected] Website: www.chrda.org Cameroon: The Anglophone Crisis 206 Villages burnt in the North West and South West Regions April 2019 SUMMARY The Center for Human Rights and Democracy in Africa (CHRDA) has analyzed data from local sources and identified 206 villages that have been partially, or completely burnt since the beginning of the immediate crisis in the Anglophone regions. Cameroon is a nation sliding into civil war in Africa. In 2016, English- speaking lawyers, teachers, students and civil society expressed “This act of burning legitimate grievances to the Cameroonian government. Peaceful protests villages is in breach of subsequently turned deadly following governments actions to prevent classical common the expression of speech and assembly. Government forces shot peaceful article 3 to the Four protesters, wounded many and killed several. Geneva Convention 1949 and the To the dismay of the national, regional and international communities, Additional Protocol II the Cameroon government began arresting activists and leaders to the same including CHRDA’s Founder and CEO, Barrister Agbor Balla, the then Convention dealing President of the now banned Anglophone Consortium. Internet was shut with the non- down for three months and all forms of dissent were stifled, forcing international conflicts. hundreds into exile. Also, the burning of In August 2017, President Paul Biya of Cameroon ordered the release of villages is in breach of several detainees, but avoided dialogue, prompting mass protests in national and September 2017 with an estimated 500,000 people on the streets of international human various cities, towns and villages. The government’s response was a rights norms and the brutal crackdown which led to a declaration of independence on October host of other laws” 1, 2017. -
Assessment of Prunus Africana Bark Exploitation Methods and Sustainable Exploitation in the South West, North-West and Adamaoua Regions of Cameroon
GCP/RAF/408/EC « MOBILISATION ET RENFORCEMENT DES CAPACITES DES PETITES ET MOYENNES ENTREPRISES IMPLIQUEES DANS LES FILIERES DES PRODUITS FORESTIERS NON LIGNEUX EN AFRIQUE CENTRALE » Assessment of Prunus africana bark exploitation methods and sustainable exploitation in the South west, North-West and Adamaoua regions of Cameroon CIFOR Philip Fonju Nkeng, Verina Ingram, Abdon Awono February 2010 Avec l‟appui financier de la Commission Européenne Contents Acknowledgements .................................................................................................... i ABBREVIATIONS ...................................................................................................... ii Abstract .................................................................................................................. iii 1: INTRODUCTION ................................................................................................... 1 1.1 Background ................................................................................................. 1 1.2 Problem statement ...................................................................................... 2 1.3 Research questions .......................................................................................... 2 1.4 Objectives ....................................................................................................... 3 1.5 Importance of the study ................................................................................... 3 2: Literature Review ................................................................................................. -

Modele-Mc2-Depliant.Pdf
Pourqoui les MC² • La pauvreté est essentiellement rurale (plus de 60% de la population) ; • Plus de 50% des pauvres (personnes vivant avec moins d’un dollar par jour) vivent en Afrique • Les populations rurales n’ont presque pas accès aux services financiers qui permettraient d’améliorer leurs conditions de vie et développer leur communauté. Le grenier de la communauté • Les zones rurales regorgent d’un grand potentiel en ressources naturelles, agropastorales, etc. encore très peu valorisées Le bien-être de la famille par la femme Listes des MC² opérationnelles au cameroun au 31 octobre 2018 1. MC² de Baham 25. MC² Fongo-Tongo 49. MC² de Baré 73. MC² de Fundong 97. MC² de Mindif 2. MC² de Manjo 26. MC² de Njombé 50. MC² de Bertoua 74. MC² de Tibati 98. MC² Bamenkombo 3. MC² de Melong 27. MC² de Mbankomo 51. MC² de Banyo 75. MC² de Mbang 99. MC² Kedjom Keku 4. MC² Penka-Michel 28. MC² Kribi- Campo 52. MC² de Mokolo 76. MC² de Belo 100. MC² de Ngong 5. MC² de Bandjoun 29. MC² de Loum 53. MC² de Makak 77. MC² de Okola 101. MC² de Bangoua Le modèle MC² 6. MC² de Badjouma 30. MC² Esse-Awae 2 54. MC² de Bangang 78. MC² Tongo Gandima 102. MC² de Tonga 7. MC² de Bafia 31. MC² de Ekondo Titi 55. MC² de Santa 79. MC² Abong-Mbang 103. MC² de Ngoro Une approche endogène 8. MC² de Bamendjou 32. MC² de Kekem 56. MC² de Bamena 80. MC² de Yabassi 104. MC² de Ndziih 9. -

PC19 Inf. 12 (In English and French / En Inglés Y Francés / En Anglais Et Français)
PC19 Inf. 12 (In English and French / en inglés y francés / en anglais et français) CONVENTION ON INTERNATIONAL TRADE IN ENDANGERED SPECIES OF WILD FAUNA AND FLORA CONVENCIÓN SOBRE EL COMERCIO INTERNACIONAL DE ESPECIES AMENAZADAS DE FAUNA Y FLORA SILVESTRES CONVENTION SUR LE COMMERCE INTERNATIONAL DES ESPECES DE FAUNE ET DE FLORE SAUVAGES MENACEES D'EXTINCTION ____________ Nineteenth meeting of the Plants Committee – Geneva (Switzerland), 18-21 April 2011 Decimonovena reunión del Comité de Flora – Ginebra (Suiza), 18-21 de abril de 2011 Dix-neuvième session du Comité pour les plantes – Genève (Suisse), 18 – 21 avril 2011 PRELIMINARY REPORT ON SUSTAINABLE HARVESTING OF PRUNUS AFRICANA (ROSACEAE) IN THE NORTH WEST REGION OF CAMEROON The attached information document has been submitted by the CITES Secretariat1. El documento informativo adjunto ha sido presentado por la Secretaría CITES2. Le document d'information joint est soumis par le Secrétariat CITES3. 1 The geographical designations employed in this document do not imply the expression of any opinion whatsoever on the part of the CITES Secretariat or the United Nations Environment Programme concerning the legal status of any country, territory, or area, or concerning the delimitation of its frontiers or boundaries. The responsibility for the contents of the document rests exclusively with its author. 2 Las denominaciones geográficas empleadas en este documento no implican juicio alguno por parte de la Secretaría CITES o del Programa de las Naciones Unidas para el Medio Ambiente sobre la condición jurídica de ninguno de los países, zonas o territorios citados, ni respecto de la delimitación de sus fronteras o límites. -

“These Killings Can Be Stopped” RIGHTS Government and Separatist Groups Abuses in Cameroon’S WATCH Anglophone Regions
HUMAN “These Killings Can Be Stopped” RIGHTS Government and Separatist Groups Abuses in Cameroon’s WATCH Anglophone Regions “These Killings Can Be Stopped” Abuses by Government and Separatist Groups in Cameroon’s Anglophone Regions Copyright © 2018 Human Rights Watch All rights reserved. Printed in the United States of America ISBN: 978-1-6231-36352 Cover design by Rafael Jimenez Human Rights Watch defends the rights of people worldwide. We scrupulously investigate abuses, expose the facts widely, and pressure those with power to respect rights and secure justice. Human Rights Watch is an independent, international organization that works as part of a vibrant movement to uphold human dignity and advance the cause of human rights for all. Human Rights Watch is an international organization with staff in more than 40 countries, and offices in Amsterdam, Beirut, Berlin, Brussels, Chicago, Geneva, Goma, Johannesburg, London, Los Angeles, Moscow, Nairobi, New York, Paris, San Francisco, Sydney, Tokyo, Toronto, Tunis, Washington DC, and Zurich. For more information, please visit our website: http://www.hrw.org JULY 2018 ISBN: 978-1-6231-36352 “These Killings Can Be Stopped” Abuses by Government and Separatist Groups in Cameroon’s Anglophone Regions Map .................................................................................................................................... i Summary ........................................................................................................................... 1 Recommendations .............................................................................................................