Cholera Outbreak
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MINMAP Région Du Centre SERVICES DECONCENTRES REGIONAUX ET DEPARTEMENTAUX
MINMAP Région du Centre SERVICES DECONCENTRES REGIONAUX ET DEPARTEMENTAUX N° Désignation des MO/MOD Nbre de Marchés Montant des Marchés N° page 1 Services déconcentrés Régionaux 19 2 278 252 000 4 Département de la Haute Sanaga 2 Services déconcentrés départementaux 6 291 434 000 7 3 COMMUNE DE BIBEY 2 77 000 000 8 4 COMMUNE DE LEMBE YEZOUM 8 119 000 000 8 5 COMMUNE DE MBANDJOCK 3 50 000 000 10 6 COMMUNE DE MINTA 5 152 500 000 10 7 COMMUNE DE NANGA-EBOKO 12 139 500 000 11 8 COMMUNE DE NKOTENG 5 76 000 000 13 9 COMMUNE DE NSEM 1 27 000 000 13 TOTAL 42 932 434 000 Département de la Lekié 10 Services déconcentrés départementaux 8 268 357 000 14 11 COMMUNE DE BATCHENGA 2 35 000 000 15 12 COMMUNE DE LOBO 8 247 000 000 15 13 COMMUNE DE MONATELE 11 171 500 000 16 14 COMMUNE DE SA'A 16 384 357 000 18 15 COMMUNE D'ELIG-MFOMO 7 125 000 000 20 16 COMMUNE D'EVODOULA 9 166 250 000 21 17 COMMUNE D'OBALA 14 223 500 000 22 18 COMMUNE D'OKOLA 22 752 956 000 24 19 COMMUNE D’EBEBDA 6 93 000 000 27 TOTAL 103 2 466 920 000 Département du Mbam et Inoubou 20 Services déconcentrés départementaux 4 86 000 000 28 21 COMMUNE DE BAFIA 5 75 500 000 28 22 COMMUNE DE BOKITO 12 213 000 000 29 23 COMMUNE DE KIIKI 4 134 000 000 31 24 COMMUNE DE KONYAMBETA 6 155 000 000 32 25 COMMUNE DE DEUK 2 77 000 000 33 26 COMMUNE DE MAKENENE 3 17 000 000 33 27 COMMUNE DE NDIKINIMEKI 4 84 000 000 34 28 COMMUNE D'OMBESSA 5 91 000 000 34 29 COMMUNE DE NITOUKOU 6 83 000 000 35 TOTAL 51 1 015 500 000 MINMAP/DIVISION DE LA PROGRAMMATION ET DU SUIVI DES MARCHES PUBLICS Page 1 de 88 N° Désignation -

Dictionnaire Des Villages Du Fako : Village Dictionary of Fako Division
OFFICE DE LA RECHERCHE SCIENTIFIOUE ET TECHNIOUE OUTRE· MER Il REPUBLIQUE UNIE DU CAMEROUN DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION SECTION DE GEOGRAPHIE 1 OFFICE DE LA RECHERCHE SCIm~TIFIQUE REPUBLIQUE UNIE ET TECmUQUE OUTRE-lViER DU CAlvŒROUN UNITED REPUBLIC OF CANEROON CENTRE O.R.S.T.O.N DE YAOUNDE DICTIONNAIRE DES VILLAGES DU FAKO VILLAGE DICTIONARY OF FAKO DIVISION Juillet 1973 July 1973 COPYRIGHT O.R.S.T.O.M 1973 TABLE DES NATIERES CONTENTS i l j l ! :i i ~ Présentation •••••.•.•.....••....•.....•....••••••.••.••••••.. 1 j Introduction ........................................•• 3 '! ) Signification des principaux termes utilisés •.............• 5 î l\lIeaning of the main words used Tableau de la population du département •...••.....•..•.•••• 8 Population of Fako division Département du Fako : éléments de démographie •.•.... ..••.•• 9 Fako division: demographic materials Arrondissements de Muyuka et de Tiko : éléments de . démographie 0 ••••••••••••••••••••••••••••••••••••••• 10 11uyul{a and Tileo sl)..bdivisions:demographic materials Arrondissement de Victoria: éléments de démographie •••.••• 11 Victoria subdivision:demographic materials Les plantations (12/1972) •••••••••••.•••••••••••••••••••••• 12 Plantations (12/1972) Liste des villages par arrondissement, commune et graupement 14 List of villages by subdivision, area council and customary court Signification du code chiffré •..•••...•.•...•.......•.•••.• 18 Neaning of the code number Liste alphabétique des villages ••••••.••••••••.•.•..•••.•.• 19 -

Shelter Cluster Dashboard NWSW052021
Shelter Cluster NW/SW Cameroon Key Figures Individuals Partners Subdivisions Cameroon 03 23,143 assisted 05 Individual Reached Trend Nigeria Furu Awa Ako Misaje Fungom DONGA MANTUNG MENCHUM Nkambe Bum NORD-OUEST Menchum Nwa Valley Wum Ndu Fundong Noni 11% BOYO Nkum Bafut Njinikom Oku Kumbo Belo BUI Mbven of yearly Target Njikwa Akwaya Jakiri MEZAM Babessi Tubah Reached MOMO Mbeggwi Ngie Bamenda 2 Bamenda 3 Ndop Widikum Bamenda 1 Menka NGO KETUNJIA Bali Balikumbat MANYU Santa Batibo Wabane Eyumodjock Upper Bayang LEBIALEM Mamfé Alou OUEST Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Fontem Nguti KOUPÉ HNO/HRP 2021 (NW/SW Regions) Toko MANENGOUBA Bangem Mundemba SUD-OUEST NDIAN Konye Tombel 1,351,318 Isangele Dikome value Kumba 2 Ekondo Titi Kombo Kombo PEOPLE OF CONCERN Abedimo Etindi MEME Number of PoC Reached per Subdivision Idabato Kumba 1 Bamuso 1 - 100 Kumba 3 101 - 2,000 LITTORAL 2,001 - 13,000 785,091 Mbongé Muyuka PEOPLE IN NEED West Coast Buéa FAKO Tiko Limbé 2 Limbé 1 221,642 Limbé 3 [ Kilometers PEOPLE TARGETED 0 15 30 *Note : Sources: HNO 2021 PiN includes IDP, Returnees and Host Communi�es The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations Key Achievement Indicators PoC Reached - AGD Breakdouwn 296 # of Households assisted with Children 27% 26% emergency shelter 1,480 Adults 21% 22% # of households assisted with core 3,769 Elderly 2% 2% relief items including prevention of COVID-19 21,618 female male 41 # of households assisted with cash for rental subsidies 41 Households Reached Individuals Reached Cartegories of beneficiaries reported People Reached by region Distribution of Shelter NFI kits integrated with COVID 19 KITS in Matoh town. -

GEF Prodoc TRI Cameroon 28 02 18
International Union for the Conservation of Nature Country: Cameroon PROJECT DOCUMENT Project Title: Supporting Landscape Restoration and Sustainable Use of local plant species and tree products (Bambusa ssp, Irvingia spp, etc) for Biodiversity Conservation, Sustainable Livelihoods and Emissions Reduction in Cameroon BRIEF DESCRIPTION OF THE PROJECT The Republic of Cameroon has a diverse ecological landscape, earning her the title “Africa in Miniature”. The southern portions of Cameroon’s forests are part of the Congo Basin forest ecosystem, the second largest remaining contiguous block of rainforest on Earth, after the Amazon. In addition to extensive Mangrove belts, Cameroon also holds significant portions of the Lower Guinea Forest Ecosystems and zones of endemism extending into densely settled portions of the Western Highlands and Montagne forests. The North of the country comprising the Dry Sudano-Sahelian Savannah Zones is rich in wildlife, and home to dense human and livestock populations. Much of the population residing in these areas lives in extreme poverty. This diversity in biomes makes Cameroon one of the most important and unique hotspots for biodiversity in Africa. However, human population growth, migrations, livelihoods strategies, rudimentary technologies and unsustainable land use for agriculture and small-scale forestry, energy and livestock, are contributing to biodiversity loss and landscape degradation in Cameroon. Despite strong institutional frameworks, forest and environmental policies/legislation, and a human resource capital, Cameroon’s network of biomes that include all types of forests, tree-systems, savannahs, agricultural mosaics, drylands, etc., are progresively confronted by various forms of degradation. Degradation, which is progressive loss of ecosystem functions (food sources, water quality and availability, biodversity, soil fertility, etc), now threatens the livelihoods of millions of Cameroonians, especially vulnerable groups like women, children and indigenous populations. -
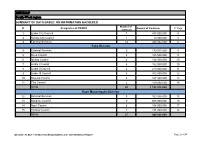
MINMAP South-West Region
MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Number of N° Designation of PO/DPO Amount of Contracts N° Page contracts 1 Limbe City Council 7 475 000 000 4 2 Kumba City Council 1 10 000 000 5 3 External Services 14 440 032 000 6 Fako Division 4 External Services 9 179 015 000 8 5 Buea Council 5 125 500 000 9 6 Idenau Council 4 124 000 000 10 7 Limbe I Council 4 152 000 000 10 8 Limbe II Council 4 219 000 000 11 9 Limbe III Council 6 102 500 000 12 10 Muyuka Council 6 127 000 000 13 11 Tiko Council 5 159 000 000 14 TOTAL 43 1 188 015 000 Kupe Muanenguba Division 12 External Services 5 100 036 000 15 13 Bangem Council 9 605 000 000 15 14 Nguti Council 6 104 000 000 17 15 Tombel Council 7 131 000 000 18 TOTAL 27 940 036 000 MINMAP / PUBLIC CONTRACTS PROGRAMMING AND MONITORING DIVISION Page 1 of 34 MINMAP South-West region SUMMARY OF DATA BASED ON INFORMATION GATHERED Lebialem Division 16 External Services 5 134 567 000 19 17 Alou Council 9 144 000 000 19 18 Menji Council 3 181 000 000 20 19 Wabane Council 9 168 611 000 21 TOTAL 26 628 178 000 Manyu Division 18 External Services 5 98 141 000 22 19 Akwaya Council 6 119 500 000 22 20 Eyomojock Council 6 119 000 000 23 21 Mamfe Council 5 232 000 000 24 22 Tinto Council 6 108 000 000 25 TOTAL 28 676 641 000 Meme Division 22 External Services 5 85 600 000 26 23 Mbonge Council 7 149 000 000 26 24 Konye Council 1 27 000 000 27 25 Kumba I Council 3 65 000 000 27 26 Kumba II Council 5 83 000 000 28 27 Kumba III Council 3 84 000 000 28 TOTAL 24 493 600 000 MINMAP / PUBLIC CONTRACTS -

Dictionnaire Des Villages Du Mbam P
OFFICE DE LA RECHERCHE REPUBliQUE FEDERALE SCIENTIFIQUE ET TECHNIQUE DU OUT,RE·MER CAMEROUN CENTRE OR5TOM DE YAOUNDE DICTIONNAIRE DES _VILLAGES DU MBAM D'après la documentation réunie par ~la Section de Géographie de l'I.R.CAM.3 REPERTQIRE GEOGRAPHIQUE DU CAMEROUN FASCICULE n° 1 1 rR-GAM 8. P. '9J SH. n° 31 YAOUNDÉ Mai 1966 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fasc. Tableau de la population du Cameroun, 68 p. Fév. 1965 SH, N° 17 Fasc. 2 Dictionnaire des villages du Dia et Lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 53 p. Août 1965 SH. N° 23 Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, 49 p. Octobre 1965 SH. N° 24 Fasc. 5 Dictionnaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du Ntem 126 p. Décembre 1965 SH. N° 26 Fasc. 7 Dictionnaire- des villages de la Mefou 108 p. Janvier 1966 SH. N° 27 Fasc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 SH. N° 28 Fasc. 9 Dictionnaire des villages de la Lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam P. 60 Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko (en préparation) Fasc. 13 ùictionnaire des villages de Lom-et-Diérem (en préparation! omCE DE LA RECHERCHE SCIENTIFIQUE RERJBLlQUE FEDERALE ET TECHNI~E OUmE-MER ID CAMEROUN _ • _cee- -- - CENTRE ORSTOM DE YAOUNDE DICTIONNAIRE ~ VILLAGES DU ...........M B A M MAI 1!66 S.R. -

Centre Region Classifications
Centre Region Classifications Considering the World Bank list of economies (June 2020) OTHM centres have been classified into three separate regions: • Region 1: High income economies; • Region 2: Upper middle income economies; and • Region 3: Lower middle income and low income economies. Centres in the United Kingdom falls into Region 1 along with other high-income economies – (normal fees apply for all Region 1 Centres). Prospective centres and learners should visit www.othm.org.uk to find which region their centre falls into and pay the appropriate fees. Economy Income group Centre class Afghanistan Low income Region 3 Albania Upper middle income Region 2 Algeria Lower middle income Region 3 American Samoa Upper middle income Region 2 Andorra High income Region 1 Angola Lower middle income Region 3 Antigua and Barbuda High income Region 1 Argentina Upper middle income Region 2 Armenia Upper middle income Region 2 Aruba High income Region 1 Australia High income Region 1 Austria High income Region 1 Azerbaijan Upper middle income Region 2 Bahamas, The High income Region 1 Bahrain High income Region 1 Bangladesh Lower middle income Region 3 Barbados High income Region 1 Belarus Upper middle income Region 2 Belgium High income Region 1 Belize Upper middle income Region 2 Benin Lower middle income Region 3 Bermuda High income Region 1 Bhutan Lower middle income Region 3 Bolivia Lower middle income Region 3 Bosnia and Herzegovina Upper middle income Region 2 Botswana Upper middle income Region 2 Brazil Upper middle income Region 2 British -

Dictionnaire Des Villages De La Haute Sanaga a Été Entièrement Remise À Jour Et Corrigée En Fonction Des Derniers Renseignements Que Nous Possédons
OFFICE DE LA RECHERCHE REPUBLIQUE FEDEIlA~ SCIENTIFIQUE ET TECHNIQUE DU OUTRE-MER CAMEROUN CENTRE ORSTOM DE YAOUNDE DICTIONNAIR'E DES VILLAGES DE LA HAUTE SANAGA (2ème Editan) ~aprèS la documentation réunie ~-:-l ~ection de Géographie de l' ORST~ "~fUTOJkGEOGRAPHIQUE DU CAMEROUN FASCICULE N° 3 B. P. 193 SH. n° 50 YAOUNDE Août 1968 REPERTOIRE GEOGRAPHIQUE DU CAMEROUN Fasc. Tableau de la population du Cameroun, 68 p. Fév. 1965 SH. N° 17 Fasc. 2 Dictionnaire des villages du Dia et lobo, 89 p. Juin 1965 SH. N° 22 Fasc. 3 Dictionnaire des villages de la Haute-Sanaga, 44 p. Août 1968 SH. N° 50 (2éme édition) Fasc. 4 Dictionnaire des villages du Nyong et Mfoumou, 49 p. Octobre 1965 SH. N° 24 ~: Fasc. 5 Dictio~riaire des villages du Nyong et Soo 45 p. Novembre 1965 SH. N° 25 Fasc. 6 Dictionnaire des villages du Ntem 102 p. Juin 1968 SH. N° 46 (2ème édition) Fasc. 7 Dictionnaire des villages de la Mefou 108 p. Janvier 1966 SH. N° 27 Fa sc. 8 Dictionnaire des villages du Nyong et Kellé 51 p. Février 1966 SH. N° 28 Fa sc. 9 Dictionnaire des villages de la lékié 71 p. Mars 1966 SH. N° 29 Fasc. 10 Dictionnaire des villages de Kribi P. Mars 1966 SH. N° 30 Fasc. 11 Dictionnaire des villages du Mbam 60 P. Mai 1966 SH. N° 31 Fasc. 12 Dictionnaire des villages de Boumba Ngoko 34 p. Juin 1966 SH. 39 Fasc. 13 Dictionnaire des villages de lom-et-Djérem 35 p. Juillet 1967 SH. 40 Fasc. 14 Dictionnaire des villages de la Kadei 52 p. -
Approved by the Ministry of the Environment and Forests
Project of Independent Observation in Support of Forest Law Enforcement in Cameroon Approved by the Ministry of the Environment and Forests Report No. 027 En Joint Mission: Central Control Unit – Independent Observer ------------------------------- Title: None Location: Central Province Mission date: September 20-21, 2002 Company: GCI Nyanzom, IBC Independent Observer (Global Witness): Mr. Stuart Wilson, Project Director Mr. Owada Jean Cyrille, Technical Assistant Mr. Tangyie Ché Célestine, Driver TABLE OF CONTENTS 1. SUMMARY ............................................................................................................. 1 2. RESOURCES USED ............................................................................................. 2 3. COMPOSITION OF THE MISSION................................................................ 2 4. CONSTRAINTS ..................................................................................................... 2 5. RESULTS OF THE MISSION............................................................................ 2 5.1. Summary of the case ............................................................................................. 2 5.2. Meetings with IBC representatives and various external services representatives 2 5.3. Official hearing of the Ombessa forest law enforcement official ......................... 3 6. CONCLUSIONS AND RECOMMENDATIONS......................................... 4 Appendix ......................................................................................................................... -

MINMAP Région Du Littoral
MINMAP Région du Littoral SYNTHESE DES DONNEES SUR LA BASE DES INFORMATIONS RECUEILLIES Nbre de Montant des N° Désignation des MO/MOD N° Page Marchés Marchés 1 Communauté Urbaine d'Edéa 6 1 747 550 008 3 2 Services déconcentrés Régionaux 10 534 821 000 4 TOTAL 16 2 282 371 008 Département du Wouri 3 Services déconcentrés départementaux 6 246 700 000 5 4 Commune de Douala 1 9 370 778 000 5 5 Commune de Douala 2 9 752 778 000 6 6 Commune de Douala 3 12 273 778 000 8 7 Commune de Douala 4 10 278 778 000 9 8 Commune de Douala 5 10 204 605 268 10 9 Commune de Douala 6 10 243 778 000 11 TOTAL 66 2 371 195 268 Département du Moungo 10 Services déconcentrés départementaux 10 159 560 000 12 11 Commune de Bare Bakem 9 234 893 804 13 12 Commune de Bonalea 11 274 397 840 14 13 Commune de Dibombari 11 267 278 000 15 14 Commune de Loum 12 228 397 903 16 15 Commune de Manjo 8 160 940 286 18 16 Commune de Mbanga 10 228 455 858 19 17 Commune de Melong 17 291 778 000 20 18 Commune de Njombe Penja 17 427 728 000 21 19 Commune d'Ebone 10 190 778 000 23 20 Commune de Mombo 9 163 878 000 24 21 Commune de Nkongsamba I 7 161 000 000 25 22 Commune de Nkongsamba II 6 172 768 640 25 23 Commune de Nkongsamba III 9 195 278 000 26 TOTAL 146 3 157 132 331 Département de la Sanaga Maritime 24 Services déconcentrés départementaux 10 214 167 000 27 25 Commune de Dibamba 14 358 471 384 28 26 Commune de Dizangue 13 252 678 000 29 27 Commune de Massock 16 319 090 512 30 28 Commune de Mouanko 9 251 001 000 31 29 Commune de Ndom 17 340 778 000 31 30 Commune de Ngambe 9 235 -

N I G E R I a C H a D Central African Republic Congo
CAMEROON: LOCATIONS OF UNHCR PERSONS OF CONCERN (September 2020) ! PERSONNES RELEVANT DE Maïné-Soroa !Magaria LA COMPETENCE DU HCR (POCs) Geidam 1,951,731 Gashua ! ! CAR REFUGEES ING CurAi MEROON 306,113 ! LOGONE NIG REFUGEES IN CAMEROON ET CHARI !Hadejia 116,409 Jakusko ! U R B A N R E F U G E E S (CENTRAL AFRICAN REPUBLIC AND 27,173 NIGERIAN REFUGEE LIVING IN URBAN AREA ARE INCLUDED) Kousseri N'Djamena !Kano ASYLUM SEEKERS 9,332 Damaturu Maiduguri Potiskum 1,032,942 INTERNALLY DISPLACED PERSO! NS (IDPs) * RETURNEES * Waza 484,036 Waza Limani Magdeme Number of refugees MAYO SAVA Mora ! < 10,000 EXTRÊME-NORD Mokolo DIAMARÉ Biu < 50,000 ! Maroua ! Minawao MAYO Bauchi TSANAGA Yagoua ! Gom! be Mubi ! MAYO KANI !Deba MAYO DANAY < 75000 Kaele MAYO LOUTI !Jos Guider Number! of IDPs N I G E R I A Lafia !Ləre ! < 10,000 ! Yola < 50,000 ! BÉNOUÉ C H A D Jalingo > 75000 ! NORD Moundou Number of returnees ! !Lafia Poli Tchollire < 10,000 ! FARO MAYO REY < 50,000 Wukari ! ! Touboro !Makurdi Beke Chantier > 75000 FARO ET DÉO Tingere ! Beka Paoua Number of asylum seekers Ndip VINA < 10,000 Bocaranga ! ! Borgop Djohong Banyo ADAMAOUA Kounde NORD-OUEST Nkambe Ngam MENCHUM DJEREM Meiganga DONGA MANTUNG MAYO BANYO Tibati Gbatoua Wum BOYO MBÉRÉ Alhamdou !Bozoum Fundong Kumbo BUI CENTRAL Mbengwi MEZAM Ndop MOMO AFRICAN NGO Bamenda KETUNJIA OUEST MANYU Foumban REPUBLBICaoro BAMBOUTOS ! LEBIALEM Gado Mbouda NOUN Yoko Mamfe Dschang MIFI Bandjoun MBAM ET KIM LOM ET DJEREM Baham MENOUA KOUNG KHI KOUPÉ Bafang MANENGOUBA Bangangte Bangem HAUT NKAM Calabar NDÉ SUD-OUEST -

Wildlife Trafficking in Cameroon and Republic of the Congo
Wildlife Traffcking in Cameroon and Republic of the Congo A Scoping Review and Recommendations for Cooperation with China A / Room 032, unit 1, foreign affairs offce building, tower garden, No. 14, South Liangmahe Road, Chaoyang District, Beijing P.C / 100600 T / 86-10-8532-5910 F / 86-10-8532-5038 E / [email protected] http://www.geichina.org Acknowledgement We would like to give special thanks to UK’s Department for International Development (DFID) for its funding support on this project. We are very grateful of Mr. Simon Essissima from the Ministry of Forestry and Wildlife of Cameroon and Mr. Nan Jiang from the Nanjing Forest Police College of China for their invaluable feedbacks and suggestions to the report. We would also like to thank Mme. Jiaman Jin, Executive Director of GEI, Mr. Chun Li, Senior Consultant of GEI, Mr. Peng Ren, Program Manager of Overseas Investment, Trade and the Environment, and Ms. Lin Ji, Executive Secretary of GEI for their guidance, support and participation throughout the research project. Finally, we would like to thank our interns who have contributed to the translation and editing of this report: Ms. Qiuyi Wang, Ms. Qian Zhu, Ms. Diana Gomez. 01 02 Acronyms Introduction ACFAP Congolese Wildlife and Protected Areas Agency [1] Wildlife traffcking is increasingly considered a threat to global conservation efforts. With global momentum to combat international wildlife traffcking, countries along the ANAFOR National Forest Development Support Agency "Congo Basin Forests," Greenpeace supply chain should take collective action to ensure effective disruption of the traffcking CAR Central African Republic USA, accessed August 09, 2019.