Guinea-Bissau (P163954)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin
Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin April 2021 This research was made possible through the Reach Alliance, a partnership between the University of Toronto’s Munk School of Global Affairs & Public Policy and the Mastercard Center for Inclusive Growth. Research was also funded by the Ralph and Roz Halbert Professorship of Innovation at the Munk School of Global Affairs & Public Policy. We express our gratitude and appreciation to those we met and interviewed. This research would not have been possible without the help of Dr. Paul Milligan from the London School of Hygiene and Tropical Medicine, ACCESS-SMC, Catholic Relief Services, the Government of Guinea and other individuals and organizations in providing and publishing data and resources. We are also grateful to Dr. Kovana Marcel Loua, director general of the National Institute of Public Health in Guinea and professor at the Gamal Abdel Nasser University of Conakry, Guinea. Dr. Loua was instrumental in the development of this research — advising on key topics, facilitating ethics board approval in Guinea and providing data and resources. This research was vetted by and received approval from the Ethics Review Board at the University of Toronto. Research was conducted during the COVID-19 pandemic in compliance with local public health measures. MASTERCARD CENTER FOR INCLUSIVE GROWTH The Center for Inclusive Growth advances sustainable and equitable economic growth and financial inclusion around the world. Established as an independent subsidiary of Mastercard, we activate the company’s core assets to catalyze action on inclusive growth through research, data philanthropy, programs, and engagement. -

Coversheet for Thesis in Sussex Research Online
A University of Sussex DPhil thesis Available online via Sussex Research Online: http://sro.sussex.ac.uk/ This thesis is protected by copyright which belongs to the author. This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the Author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the Author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given Please visit Sussex Research Online for more information and further details The Route of the Land’s Roots: Connecting life-worlds between Guinea-Bissau and Portugal through food-related meanings and practices Maria Abranches Doctoral Thesis PhD in Social Anthropology UNIVERSITY OF SUSSEX 2013 UNIVERSITY OF SUSSEX PhD in Social Anthropology Maria Abranches Doctoral Thesis The Route of the Land’s Roots: Connecting life-worlds between Guinea-Bissau and Portugal through food-related meanings and practices SUMMARY Focusing on migration from Guinea-Bissau to Portugal, this thesis examines the role played by food and plants that grow in Guinean land in connecting life-worlds in both places. Using a phenomenological approach to transnationalism and multi-sited ethnography, I explore different ways in which local experiences related to food production, consumption and exchange in the two countries, as well as local meanings of foods and plants, are connected at a transnational level. One of my key objectives is to deconstruct some of the binaries commonly addressed in the literature, such as global processes and local lives, modernity and tradition or competition and solidarity, and to demonstrate how they are all contextually and relationally entwined in people’s life- worlds. -

The Double-Sided Effects of Mycobacterium Bovis Bacillus Calmette–Guérin Vaccine ✉ ✉ Junli Li 1,2,3,4, Lingjun Zhan1,2,3,4 and Chuan Qin 1,2,3,4
www.nature.com/npjvaccines REVIEW ARTICLE OPEN The double-sided effects of Mycobacterium Bovis bacillus Calmette–Guérin vaccine ✉ ✉ Junli Li 1,2,3,4, Lingjun Zhan1,2,3,4 and Chuan Qin 1,2,3,4 Bacillus Calmette–Guérin (BCG), the only vaccine proven to be effective against tuberculosis (TB), is the most commonly used vaccine globally. In addition to its effects on mycobacterial diseases, an increasing amount of epidemiological and experimental evidence accumulated since its introduction in 1921 has shown that BCG also exerts non-specific effects against a number of diseases, such as non-mycobacterial infections, allergies and certain malignancies. Recent Corona Virus Disease 2019 (COVID-19) outbreak has put BCG, a classic vaccine with significant non-specific protection, into the spotlight again. This literature review briefly covers the diverse facets of BCG vaccine, providing new perspectives in terms of specific and non-specific protection mechanisms of this old, multifaceted, and controversial vaccine. npj Vaccines (2021) 6:14 ; https://doi.org/10.1038/s41541-020-00278-0 INTRODUCTION infections observed in children after receiving BCG vaccina- 17–20 Bacillus Calmette–Guérin (BCG), a live-attenuated bacterial tion . Clinical evidence also suggests that BCG may be 1234567890():,; effective against infections caused by viral pathogens, such as vaccine derived from Mycobacterium bovis was originally – 1 respiratory syncytial virus21,22, human papilloma virus23 25,and isolated in 1902 from a cow with tuberculosis (TB) .Theisolate 26 was cultured continuously for >230 generations for 13 years herpes simplex virus . Moreover, an increasing number of (1908–1921) to generate a mutant strain with weakened animal studies using mouse models have demonstrated the virulence but with high immunogenicity2. -
Weekly Bulletin on Outbreaks
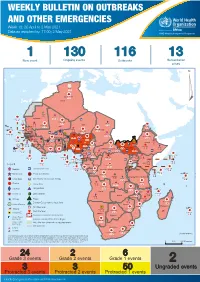
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 18: 26 April to 2 May 2021 Data as reported by: 17:00; 2 May 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 130 116 13 New event Ongoing events Outbreaks Humanitarian crises 64 0 122 522 3 270 Algeria ¤ 36 13 612 0 5 901 175 Mauritania 7 2 13 915 489 110 0 7 0 Niger 18 448 455 Mali 3 671 10 567 0 6 0 2 079 4 4 828 170 Eritrea Cape Verde 40 433 1 110 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 24 368 224 1 069 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 258 384 3 726 0 165 167 2 063 Guinea 13 319 157 12 3 736 67 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 556 5 6 188 15 Sierra Leone Togo 3 473 296 52 14 Ghana 70 607 1 064 6 411 88 Côte d'Ivoire 10 583 115 14 484 479 65 0 40 0 Liberia 17 0 South Sudan Central African Republic 1 029 2 49 0 97 17 25 0 22 333 268 46 150 287 92 683 779 Cameroon 7 0 28 676 137 843 20 3 1 160 422 2 763 655 2 91 0 123 12 6 1 488 6 4 057 79 13 010 7 694 112 Equatorial Guinea Uganda 1 0 542 8 Sao Tome and Principe 32 11 2 066 85 41 973 342 Kenya Legend 7 821 99 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 310 35 25 253 337 Measles 23 075 139 Democratic Republic of the Congo 11 016 147 Burundi 4 046 6 Monkeypox Ebola virus disease Seychelles 29 965 768 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 191 0 5 941 26 509 21 Cholera Yellow fever 63 1 6 257 229 26 993 602 cVDPV2 Dengue fever 91 693 1 253 Comoros Angola Malawi COVID-19 Leishmaniasis 34 096 1 148 862 0 3 840 146 Zambia 133 -
BCG Coverage and Barriers to BCG Vaccination In
Thysen et al. BMC Public Health 2014, 14:1037 http://www.biomedcentral.com/1471-2458/14/1037 RESEARCH ARTICLE Open Access BCG coverage and barriers to BCG vaccination in Guinea-Bissau: an observational study Sanne Marie Thysen1,2*, Stine Byberg1,2, Marie Pedersen1,2, Amabelia Rodrigues1, Henrik Ravn2,3, Cesario Martins1, Christine Stabell Benn2,3, Peter Aaby1,2,3 and Ane Bærent Fisker1,2 Abstract Background: BCG vaccination is recommended at birth in low-income countries, but vaccination is often delayed. Often 20-dose vials of BCG are not opened unless at least ten children are present for vaccination (“restricted vial-opening policy”). BCG coverage is usually reported as 12-month coverage, not disclosing the delay in vaccination. Several studies show that BCG at birth lowers neonatal mortality. We assessed BCG coverage at different ages and explored reasons for delay in BCG vaccination in rural Guinea-Bissau. Methods: Bandim Health Project (BHP) runs a health and demographic surveillance system covering women and their children in 182 randomly selected village clusters in rural Guinea-Bissau. BCG coverage was assessed for children born in 2010, when the restricted vial-opening policy was universally implemented, and in 2012–2013, where BHP provided BCG to all children at monthly visits in selected intervention regions. Factors associated with delayed BCG vaccination were evaluated using logistic regression models. Coverage between intervention and control regions were evaluated in log-binomial regression models providing prevalence ratios. Results: Among 3951 children born in 2010, vaccination status was assessed for 84%. BCG coverage by 1 week of age was 11%, 38% by 1 month, and 92% by 12 months. -

Water Diseases: Dynamics of Malaria and Gastrointestinal Diseases in the Tropical Guinea-Bissau (West Africa) Sandra Cristina De Oliveira Alves M 2018
MESTRADO SAÚDE PÚBLICA Water diseases: dynamics of malaria and gastrointestinal diseases in the tropical Guinea-Bissau (West Africa) Sandra Cristina de Oliveira Alves M 2018 Water diseases: dynamics of malaria and gastrointestinal diseases in the tropical Guinea-Bissau (West Africa) Master in Public Health || Thesis || Sandra Cristina de Oliveira Alves Supervisor: Prof. Doutor Adriano A. Bordalo e Sá Institute Biomedical Sciences University of Porto Porto, September 2018 ACKNOWLEDGMENTS I would like to show, in first place, my thankfulness to my supervisor Professor Adriano Bordalo e Sá, for “opening the door” to this project supplying the logbook raw data of Bolama Regional Hospital as well as meteorological data from the Serviço de Meterologia of Bolama, for is orientation and scientific support. The Regional Director of the Meteorological survey in Bolama, D. Efigénia, is thanked for supplying the values precipitation and temperature, retrieved from manual spread sheets. My gratitude also goes to all the team of the Laboratory Hydrobiology and Ecology, ICBAS-UP, who received me in a very friendly way, and always offers me their help (and cakes). An especial thanks to D. Lurdes Lima, D. Fernanda Ventura, Master Paula Salgado and Master Ana Machado (Ana, probable got one or two wrinkles for truly caring), thank you. Many many thanks to my friends, and coworkers, Paulo Assunção and Ana Luísa Macedo, who always gave me support and encouragement. Thank you to my biggest loves, my daughter Cecilia and to the ONE Piero. Thank you FAMILY, for the shared DNA and unconditional love. Be aware for more surprises soon. Marisa Castro, my priceless friend, the adventure never ends! This path would have been so harder and lonely without you. -

EPI-NEWS NATIONAL SURVEILLANCE of COMMUNICABLE DISEASES Editor: Peter Henrik Andersen Dept
EPI-NEWS NATIONAL SURVEILLANCE OF COMMUNICABLE DISEASES Editor: Peter Henrik Andersen Dept. of Epidemiology Tel.: +45 3268 3268 • Fax: +45 3268 3874 Statens Serum Institut • 5 Artillerivej • DK 2300 Copenhagen S www.ssi.dk • [email protected] • ISSN: 1396-4798 DANISH HEALTH RESEARCH IN GUINEA-BISSAU No. 34, 2006 In one of the world’s poorest years, the BHP has been the focus of yields 70% protection against countries, Guinea-Bissau in West 22 PhD theses, mainly Danish, and rotavirus diarrhoea, and 52% Africa, the Bandim Health Project nine doctoral dissertations. protection against reinfection during (BHP) has been engaged in epide- the first year following the initial miological research since 1978 Research focus areas infection. This high protection rate focussing on infection, vaccination Two-dose measles vaccination suggests that a rotavirus vaccine and the long-term effects of health strategy: would be an effective means to intervention. Infection with measles before the reduce the incidence of acute The BHP is a collaboration between WHO recommended vaccination age diarrhoea with dehydration and Statens Serum Institut and the at 9 months is a growing problem in associated deaths. Guinea-Bissau Ministry of Health. the developing countries. This is For further information on the BHP, Child mortality in Guinea-Bissau due, among others, to increasing please contact project secretary ranks among the highest worldwide: urbanisation and an increase in the Christina Rasmussen, [email protected]. > 200 per 1000 live born infants share of mothers who were them- (P. Valentiner-Branth, K. Mølbak, during the first three years of life. selves measles vaccinated at a young Dept. -

Annex A: Characteristics of Included Articles
Systematic review of the non-specific effects of BCG, DTP and measles containing vaccines ANNEX A: CHARACTERISTICS OF INCLUDED ARTICLES Article group Birth dates Vaccines Details of the included article Total number of administered (type, children Ref ID (citation) Study period strain, reason) described/analysed Region Follow up Effect Modifier (Additional references)1 Algeria Birth dates: 1935 BCG vaccinated vs. BCG Quasi-randomised controlled trial conducted in a Muslim population in Algeria where Total number of children unvaccinated (Institute children born in 1935 were allocated to BCG (given orally) or unvaccinated at birth. Children described: 41,307 #9283(1) Study period: May Pasteur, orally revaccinated at ages 1, 3, 7 and 15 years were followed up for up to 6 months after vaccine. 1935 to December 1947 Total number of children Algiers, periurban, administered, research Inclusion Criteria: Participants were newborns from Algerian Muslim families with very low analysed: 39,259 suburban and rural Follow up: ≤ 12 years purpose) socioeconomic status. areas No modifier reported Exclusion Criteria: Not clearly stated Vaccine ascertainment: Recorded at point of vaccination Mortality ascertainment: Routine home visits Bangladesh A Birth dates: born BCG vs. no BCG Observational cohort reporting all-cause child mortality from 70 villages within the Maternal Total number of children before 1 January 2000 Child Health And Family Planning programme area participating in the Health And described: 39,625 #797(2) DPT vs. no DPT Demographic Surveillance -

WEEKLY BULLETIN on OUTBREAKS and OTHER EMERGENCIES Week 12: 16 - 22 March 2020 Data As Reported By: 17:00; 22 March 2020
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 12: 16 - 22 March 2020 Data as reported by: 17:00; 22 March 2020 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 7 95 91 11 New events Ongoing events Outbreaks Humanitarian crises 201 17 Algeria 1 0 91 0 2 0 Gambia 1 0 1 0 Mauritania 14 7 20 0 9 0 Senegal 304 1 1 0Eritrea Niger 2 410 23 Mali 67 0 1 0 3 0 Burkina Faso 41 7 1 0 Cabo Verdé Guinea Chad 1 251 0 75 3 53 0 4 0 4 690 18 4 1 22 0 21 0 Nigeria 2 0 Côte d’Ivoire 1 873 895 15 4 0 South Sudan 917 172 40 0 3 970 64 Ghana16 0 139 0 186 3 1 0 14 0 Liberia 25 0 Central African Benin Cameroon 19 0 4 732 26 Ethiopia 24 0 Republic Togo 1 618 5 7 626 83 352 14 1 449 71 2 1 Uganda 36 16 Democratic Republic 637 1 169 0 9 0 15 0 Equatorial of Congo 15 5 202 0 Congo 1 0 Guinea 6 0 3 453 2 273 Kenya 1 0 253 1 Legend 3 0 6 0 38 0 37 0 Gabon 29 981 384 Rwanda 21 0 Measles Humanitarian crisis 2 0 4 0 4 998 63 Burundi 7 0 Hepatitis E 8 0 Monkeypox 8 892 300 3 294 Seychelles 30 2 108 0 Tanzania Yellow fever 12 0 Lassa fever 79 0 Dengue fever Cholera Angola 547 14 Ebola virus disease Rift Valley Fever Comoros 129 0 2 0 Chikungunya Malawi 218 0 cVDPV2 2 0 Zambia Leishmaniasis Mozambique 3 0 3 0 COVID-19 Plague Zimbabwe 313 13 Madagascar Anthrax Crimean-Congo haemorrhagic fever Namibia 286 1 Malaria 2 0 24 2 12 0 Floods Meningitis 3 0 Mauritius Cases 7 063 59 1 0 Deaths Countries reported in the document Non WHO African Region Eswatini N WHO Member States with no reported events W E 3 0 Lesotho4 0 402 0 South Africa 20 0 S South Africa Graded events † 40 15 1 Grade 3 events Grade 2 events Grade 1 events 39 22 20 31 Ungraded events ProtractedProtracted 3 3 events events Protracted 2 events ProtractedProtracted 1 1 events event Health Emergency Information and Risk Assessment Overview This Weekly Bulletin focuses on public health emergencies occurring in the WHO Contents African Region. -

Too Many Chefs in Africa Blocked Completely
ORIGINAL ARTICLE Yet, uncertain data like this forms basis for donations to the health sector, and DC that are not able to demonstrate a reduction in child mortality will experience that donations are withheld or are Too many chefs in Africa blocked completely. Nevertheless, data from longitudinal demo- graphic health surveillance research sites in DC follow child popula- – secondary publication tions that are large enough to capture even smaller changes in child mortality [2]. Morten Sodemann, Senior Researcher On the contrary, donors have excluded long-term involvement with rapid diminishing resources for development aid, demands for short-term goals and lacking support of valid mortality data [3]. In Statens Serum Institut, Bandim Health project. an editorial in The Lancet 2004 it is concluded that biomedical re- Correspondence: Morten Sodemann, Bandim Health project, Statens Serum search has failed to tackle the massive health problems in DC [4]. Institut, Artellerivej 5, 2300 København S, Denmark. E-mail: [email protected] ABSTINENCE AND RELUCTANCE The 2015 goals are a political manifest and should be seen in that Dan Med Bull 2007;54:52-4 context. There are urgent health problems that are not mentioned in the millennium goals. The significance of persistently low quality of ABSTRACT care in DC health sectors as well as the poor dissemination of exist- Available interventions could prevent six out of ten million deaths in chil- ing well proven health interventions like child immunizations are dren younger than five years of age every year. The health sector and donor examples of this. A decline in maternal mortality is bound up with agencies bear responsibility for not using these interventions. -

UNICEF GUINEA-BISSAU Review of Malnutrition Prevention and Management Project
UNICEF GUINEA-BISSAU Review of Malnutrition Prevention and Management Project March 2018 Table of Contents Table of Figures ............................................................................................................................................................. 1 Executive Summary ....................................................................................................................................................... 2 Acknowledgements ....................................................................................................................................................... 4 Introduction ................................................................................................................................................................... 5 Objectives ...................................................................................................................................................................... 5 Key definitions ............................................................................................................................................................... 5 Background and Context ............................................................................................................................................... 6 Evaluation ...................................................................................................................................................................... 8 Challenges and Suggestions for the Future ................................................................................................................ -
How Can the Health Systems of Guinea, Sierra Leone and Liberia Be Improved?
How can the health systems of Guinea, Sierra Leone and Liberia be improved? Results of three Open Space Conferences with participants from government and civil society, healthcare providers and users, community health volunteers and traditional practitioners, donors and aid organization Table of Content Executive summary 4 1. – Introduction 5 2. – Methodology of the Open Space Conference 6 3. – Similarities in discussion of topics and solutions 7 4. – Differences in the discussions 9 5. – Operational research and support needs 10 6. – Conclusion 11 Annex A: Guinea – Detailed results 12 A 1. – The Conference in Guinea 13 A 2. – topics raised and discussed 14 a. Improvement of health care facilities and management 14 b. Health workers and human resource management 14 c. Referral systems 15 d. Infection Prevention & Control and early warning systems 16 e. Reasons and aftermath of the Ebola crisis 17 F. Nutrition and food security 17 A 3. – Aspects relating to vulnerable groups 18 a. Women 18 b. Infants and children under 5 years 19 c. Persons living with disabilities or chronic illnesses 19 A 4. – Community involvement 19 A 5. – Top 7 Community Action Priorities 20 Annex B: Liberia – Detailed results 22 B 1. – The Conference in Liberia 23 B 2. – topics raised and discussed 24 a. Better health through water, sanitation and environment 24 b. Improvement of health care facilities and management 24 c. Referral systems for better health care 24 d. Infection Prevention & Control and early warning systems 25 e. Health workers and human resource management 25 f. Traditional medicine 27 g. Reasons and aftermath of the Ebola crisis 27 B 3.