Mapping Maternal and Newborn Healthcare Access in West African Countries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin
Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin April 2021 This research was made possible through the Reach Alliance, a partnership between the University of Toronto’s Munk School of Global Affairs & Public Policy and the Mastercard Center for Inclusive Growth. Research was also funded by the Ralph and Roz Halbert Professorship of Innovation at the Munk School of Global Affairs & Public Policy. We express our gratitude and appreciation to those we met and interviewed. This research would not have been possible without the help of Dr. Paul Milligan from the London School of Hygiene and Tropical Medicine, ACCESS-SMC, Catholic Relief Services, the Government of Guinea and other individuals and organizations in providing and publishing data and resources. We are also grateful to Dr. Kovana Marcel Loua, director general of the National Institute of Public Health in Guinea and professor at the Gamal Abdel Nasser University of Conakry, Guinea. Dr. Loua was instrumental in the development of this research — advising on key topics, facilitating ethics board approval in Guinea and providing data and resources. This research was vetted by and received approval from the Ethics Review Board at the University of Toronto. Research was conducted during the COVID-19 pandemic in compliance with local public health measures. MASTERCARD CENTER FOR INCLUSIVE GROWTH The Center for Inclusive Growth advances sustainable and equitable economic growth and financial inclusion around the world. Established as an independent subsidiary of Mastercard, we activate the company’s core assets to catalyze action on inclusive growth through research, data philanthropy, programs, and engagement. -
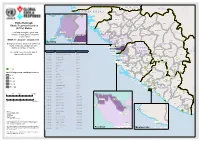
Etc Status with 21Confcase 1.Pdf
SE N E G A L M A L I GU IN EA -B IS SA U Koundara Mali ETC"-GIN-003 Koubia Gaoual Lelouma Dinguiraye Siguiri Ebola Outbreak: Labe Tougue Ebola Treatment Centres Telimele (ETCs) Status Dalaba Kouroussa Boke This Map shows the status and ETC"-GIN-012 Pita Mandiana Boffa Dabola location of each Ebola Treatment Mamou Fria Center (ETC). ETC"-GIN-001 ETC"-GIN-018 Dubreka Kindia Faranah ETC-GIN-015 WEEK 17: 20 April - 26 April 2015 " Kankan Conakry Copyright:© 2014 Esri Background colour show new confirmed Koinadugu ETC-GIN-00C3 oyah G U I N E A " Bombali cases for the last 21 days for each ConakryETC-GIN-012 district, prefecture or county. ETC"-EGT"ICN"-G00IN1-018 S I E R R A Kissidougou CÔ TE ETC-GIN-017 ETC CODE Site Name Country Forecariah " L E O N E Kerouane D' IV OI R E The number over the ETC sign is ETC-GIN-001 Conakry Region Guinea Beyla Freetownreferenced in the table. ETC-GIN-003 Kindia Region, Coyah Prefecture Guinea Kambia ETC"-SLE-034 ETC-SLE-008 ETC-GIN-007 Nzérékoré Region Guinea " Kono Gueckedou ETC-GIN-009 Nzérékoré Region Guinea Port Loko EETTCC--SSLLEE--00002571 ETC-SLE-022 "" " ETC-GIN-009 ETC-GIN-010 Nzérékoré Region Guinea ETC-SLE-031 " " ETC-GIN-010 Western " ETC-GIN-011 ETC-GIN-011 Nzérékoré Region Guinea Area Urban ETECT-SCL-SEL-0E2-4028 Tonkolili " ETC-LBR-011 ETC-GIN-012 Conakry Region Guinea "E"ETTC"C--SSLLEE--00121375 ETECT"-CS-LSEL-E0-2303226 " ETC-GIN-015 Kindia Guinea ET"C"-SLE-0116 Lofa Macenta Western " " ETC-SLE-009 ETC-GIN-017 Forecariah Guinea Area Rural " ETC-GIN-018 Conakry Guinea ETC-SLE-004 Nzerekore -
PRADD II Guinea Impact Evaluation Design Report
EVALUATION, RESEARCH AND COMMUNICATION (ERC) Property Rights and Artisanal Diamond Development Project II (PRADD II) Impact Evaluation Design Report AUGUST 2014 This document was produced for review by the United States Agency for International Development. It was prepared by Cloudburst Consulting Group, Inc. for the Evaluation, Research, and Communication (ERC) Task Order under the Strengthening Tenure and Resource Rights (STARR) IQC. Written and prepared by Heather Huntington, Michael McGovern, and Darrin Christensen. Prepared for the United States Agency for International Development, USAID Contract Number AID- OAA-TO-13-00019, Evaluation, Research and Communication (ERC) Task Order under Strengthening Tenure and Resource Rights (STARR) IQC No. AID-OAA-I-12-00030. Implemented by: Cloudburst Consulting Group, Inc. 8400 Corporate Drive, Suite 550 Landover, MD 20785-2238 EVALUATION, RESEARCH AND COMMUNICATION (ERC) Property Rights and Artisanal Diamond Development Project II (PRADD II) Impact Evaluation Design Report AUGUST 2014 DISCLAIMER The authors' views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. CONTENTS 36T36TCONTENTS36T36T ............................................................................................................................ 4 36T36TACRONYMS AND ABBREVIATIONS36T36T ..................................................................................... 5 36T36T1.0 INTRODUCTION36T36T .............................................................................................................. -

Culture and Mental Health in Liberia: a Primer 2017
WHO/MSD/MER/17.3 Culture and Mental Health in Liberia: A Primer 2017 Culture and Mental Health in Liberia: A Primer WHO/MSD/MER/17.3 © World Health Organization 2017 Some rights reserved. This work is available under the CC BY-NC-SA 3.0 IGO licence. Publications of the World Health Organization are available on the WHO website (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for non-commercial distribution – should be addressed to WHO Press through the WHO website (www.who.int/about/licensing/copyright_form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. -

Risk Factors Associated with the Contraction of Ebola Virus Disease in Liberia Beyan Yancy Sana Walden University
Walden University ScholarWorks Walden Dissertations and Doctoral Studies Walden Dissertations and Doctoral Studies Collection 2019 Risk Factors Associated with the Contraction of Ebola Virus Disease in Liberia Beyan Yancy Sana Walden University Follow this and additional works at: https://scholarworks.waldenu.edu/dissertations Part of the Medicine and Health Sciences Commons This Dissertation is brought to you for free and open access by the Walden Dissertations and Doctoral Studies Collection at ScholarWorks. It has been accepted for inclusion in Walden Dissertations and Doctoral Studies by an authorized administrator of ScholarWorks. For more information, please contact [email protected]. Walden University College of Health Sciences This is to certify that the doctoral study by Beyan Y. Sana has been found to be complete and satisfactory in all respects, and that any and all revisions required by the review committee have been made. Review Committee Dr. Srikanta Banerjee, Committee Chairperson, Public Health Faculty Dr. Jirina Foltysova, Committee Member, Public Health Faculty Dr. German Gonzalez, University Reviewer, Public Health Faculty Chief Academic Officer Eric Riedel, Ph.D. Walden University 2019 Abstract Risk Factors Associated with the Contraction of Ebola Virus Disease in Liberia by Beyan Y. Sana MPH, Walden University, 2016 BS, University of Maryland School of Medicine, 2008 BS, University of Liberia, 2001 Doctoral Study Proposal Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Public Health Walden University May 2019 Abstract Ebola virus disease (EVD) is a highly transmittable disease with high mortality rate. The purpose of this study was to examine risk factors associated with the contraction of EVD in Liberia. -

GUINEA Ebola Situation Report
GUINEA Ebola Situation Report 25 February 2015 HIGHLIGHTS SITUATION IN NUMBERS The total number of confirmed cases of Ebola went up to 2,762 in week As of 22 FEBRUARY 2015 eight, according to WHO’s Epidemiological Situation Report. The total number of confirmed, suspected and probable cases rose to 3,155. The number of deaths resulting from confirmed cases of Ebola climbed to 3,155 1,704 and the total number of deaths to 2,091. Cases of Ebola (2,762 confirmed) After the outbreak of measles in Gaoual and Koundara health districts in the Boke region, UNICEF supported a six-day immunization campaign 2,091 in Gaoual. After four days of vaccinations, 17,910 children aged Deaths (1,704 confirmed) between 6 months and 10 years had been immunized against measles. The total vaccination target is 59,555 children. 529 UNICEF launched a survey in Macenta to gauge opinions about the Confirmed cases among children role the Community Transit Centre (CTCom) should play after the 0-17 Ebola response is over. Staff at health facilities, members of the local community and other partners were asked to participate. 312 UNICEF constructed seven new water points this week in the Faranah Deaths of children and youth and N’Zérékoré regions, bringing the total number of water points built there since the start of the outbreak to 124 and the total number of aged 0-17 (confirmed) people with improved access to water to more than 37,200. UNICEF and partners distributed 12,439 household WASH kits 4,105,926 benefitting 87, 073 people in Ebola-affected areas. -

Coversheet for Thesis in Sussex Research Online
A University of Sussex DPhil thesis Available online via Sussex Research Online: http://sro.sussex.ac.uk/ This thesis is protected by copyright which belongs to the author. This thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the Author The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the Author When referring to this work, full bibliographic details including the author, title, awarding institution and date of the thesis must be given Please visit Sussex Research Online for more information and further details The Route of the Land’s Roots: Connecting life-worlds between Guinea-Bissau and Portugal through food-related meanings and practices Maria Abranches Doctoral Thesis PhD in Social Anthropology UNIVERSITY OF SUSSEX 2013 UNIVERSITY OF SUSSEX PhD in Social Anthropology Maria Abranches Doctoral Thesis The Route of the Land’s Roots: Connecting life-worlds between Guinea-Bissau and Portugal through food-related meanings and practices SUMMARY Focusing on migration from Guinea-Bissau to Portugal, this thesis examines the role played by food and plants that grow in Guinean land in connecting life-worlds in both places. Using a phenomenological approach to transnationalism and multi-sited ethnography, I explore different ways in which local experiences related to food production, consumption and exchange in the two countries, as well as local meanings of foods and plants, are connected at a transnational level. One of my key objectives is to deconstruct some of the binaries commonly addressed in the literature, such as global processes and local lives, modernity and tradition or competition and solidarity, and to demonstrate how they are all contextually and relationally entwined in people’s life- worlds. -

PDF File Generated From
OCCASION This publication has been made available to the public on the occasion of the 50th anniversary of the United Nations Industrial Development Organisation. DISCLAIMER This document has been produced without formal United Nations editing. The designations employed and the presentation of the material in this document do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations Industrial Development Organization (UNIDO) concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries, or its economic system or degree of development. Designations such as “developed”, “industrialized” and “developing” are intended for statistical convenience and do not necessarily express a judgment about the stage reached by a particular country or area in the development process. Mention of firm names or commercial products does not constitute an endorsement by UNIDO. FAIR USE POLICY Any part of this publication may be quoted and referenced for educational and research purposes without additional permission from UNIDO. However, those who make use of quoting and referencing this publication are requested to follow the Fair Use Policy of giving due credit to UNIDO. CONTACT Please contact [email protected] for further information concerning UNIDO publications. For more information about UNIDO, please visit us at www.unido.org UNITED NATIONS INDUSTRIAL DEVELOPMENT ORGANIZATION Vienna International Centre, P.O. Box 300, 1400 Vienna, Austria Tel: (+43-1) 26026-0 · www.unido.org · [email protected] 201./-qq • INTER-AFRICAN MANUFACTURING AND TRADING IN THE ALUMINIUM INDUSTRY TECHNICAL REPORT SPONSORED BY THE UNITED NATIONS INDUSTRIAL DEVELOPMENT ORGANIZATION (UNIDO) AND THE UNITED NATIONS ECONOMIC COMMISSION FOR AFRICA (UNECA) Prepared By ENG. -

Establishing National Multisectoral Coordination and Collaboration
Agbo et al. One Health Outlook (2019) 1:4 One Health Outlook https://doi.org/10.1186/s42522-019-0004-z RESEARCH Open Access Establishing National Multisectoral Coordination and collaboration mechanisms to prevent, detect, and respond to public health threats in Guinea, Liberia, and Sierra Leone 2016–2018 Serge Agbo1, Lionel Gbaguidi1, Chethana Biliyar1, Seydou Sylla2, Mukeh Fahnbulleh3, John Dogba4, Sakoba Keita5, Sarian Kamara6, Amara Jambai6, Albert Harris4, Tolbert Nyenswah7, Mane Seni8, Sow Bhoye9, Sambe Duale10 and Andrew Kitua11* Abstract Background: The governments of Guinea, Liberia, and Sierra Leone have acknowledged that weak health systems and poor coordination of efforts hampered effectiveness of the 2014–2016 Ebola outbreak response. The bitter experience of the Ebola outbreak response served as an important catalyst for increased efforts to comply with World Health Organization (WHO) International Health Regulations (IHR 2005), Performance of Veterinary Services (PVS) Pathway capacities, and Global Health Security Agenda (GHSA) goals. In November 2016, an interministerial meeting held in Dakar, Senegal, resulted in formalized commitments from the three nations to strengthen resilience to health threats by establishing a Regional Strategic Roadmap to institutionalize the One Health approach. Since then, each country has made significant progress towards establishing National One Health Platforms to coordinate health security interventions, in collaboration with international partners. This paper outlines the methodology and -

The Road to Recovery: Rebuilding Liberia's Health System
a report of the csis global health policy center The Road to Recovery rebuilding liberia’s health system 1800 K Street, NW | Washington, DC 20006 Author Tel: (202) 887-0200 | Fax: (202) 775-3199 Richard Downie E-mail: [email protected] | Web: www.csis.org August 2012 CHARTING our future a report of the csis global health policy center The Road to Recovery rebuilding liberia’s health system Author Richard Downie August 2012 CHARTING our future About CSIS—50th Anniversary Year For 50 years, the Center for Strategic and International Studies (CSIS) has developed practical solutions to the world’s greatest challenges. As we celebrate this milestone, CSIS scholars continue to provide strategic insights and bipartisan policy solutions to help decisionmakers chart a course toward a better world. CSIS is a bipartisan, nonprofit organization headquartered in Washington, D.C. The Center’s 220 full-time staff and large network of affiliated scholars conduct research and analysis and de- velop policy initiatives that look into the future and anticipate change. Since 1962, CSIS has been dedicated to finding ways to sustain American prominence and prosperity as a force for good in the world. After 50 years, CSIS has become one of the world’s pre- eminent international policy institutions focused on defense and security; regional stability; and transnational challenges ranging from energy and climate to global development and economic integration. Former U.S. senator Sam Nunn has chaired the CSIS Board of Trustees since 1999. John J. Hamre became the Center’s president and chief executive officer in 2000. CSIS was founded by David M. -
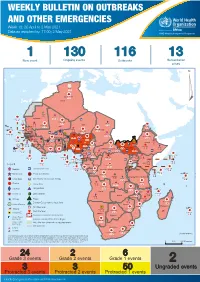
Weekly Bulletin on Outbreaks
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 18: 26 April to 2 May 2021 Data as reported by: 17:00; 2 May 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 130 116 13 New event Ongoing events Outbreaks Humanitarian crises 64 0 122 522 3 270 Algeria ¤ 36 13 612 0 5 901 175 Mauritania 7 2 13 915 489 110 0 7 0 Niger 18 448 455 Mali 3 671 10 567 0 6 0 2 079 4 4 828 170 Eritrea Cape Verde 40 433 1 110 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 24 368 224 1 069 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 258 384 3 726 0 165 167 2 063 Guinea 13 319 157 12 3 736 67 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 556 5 6 188 15 Sierra Leone Togo 3 473 296 52 14 Ghana 70 607 1 064 6 411 88 Côte d'Ivoire 10 583 115 14 484 479 65 0 40 0 Liberia 17 0 South Sudan Central African Republic 1 029 2 49 0 97 17 25 0 22 333 268 46 150 287 92 683 779 Cameroon 7 0 28 676 137 843 20 3 1 160 422 2 763 655 2 91 0 123 12 6 1 488 6 4 057 79 13 010 7 694 112 Equatorial Guinea Uganda 1 0 542 8 Sao Tome and Principe 32 11 2 066 85 41 973 342 Kenya Legend 7 821 99 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 310 35 25 253 337 Measles 23 075 139 Democratic Republic of the Congo 11 016 147 Burundi 4 046 6 Monkeypox Ebola virus disease Seychelles 29 965 768 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 191 0 5 941 26 509 21 Cholera Yellow fever 63 1 6 257 229 26 993 602 cVDPV2 Dengue fever 91 693 1 253 Comoros Angola Malawi COVID-19 Leishmaniasis 34 096 1 148 862 0 3 840 146 Zambia 133 -

COVID-19 Promising Practice Liberia
ENSURING ACCESS TO ROUTINE AND ESSENTIAL SERVICES DURING COVID-19 THROUGH COMMUNITY- BASED SERVICES IN LIBERIA C O V I D - 1 9 P R O M I S I N G P R A C T I C E S E X E C U T I V E S U M M A R Y LIBERIA PHC AT A GLANCE Liberia is a low-income country in the process of strengthening their health system through the establishment of essential and routine services in the community through its National Community Health Assistant Program. P o p u l a t i o n : 4 . 8 2 M In 2014, the country suffered from an Ebola G D P / C a p i t a : $ 6 7 7 . 3 2 ( c u r r e n t U S D ) H u m a n D e v e l o p m e n t I n d e x : 0 . 4 7 outbreak which led to 25,515 cases and 10,572 L i f e E x p e c t a n c y a t B i r t h : 6 3 . 7 Y e a r s deaths. This outbreak disrupted essential health services, and weakened the health system’s overall Liberia’s health system has been in the process of capacity recovery from past civil conflict that lasted a few decades and ended in 2003, at which point only 30 The first local case of COVID-19 in Liberia was physicians remained in Liberia and 83% of the public confirmed in March 2020, and led to the activation health facilities were non-functional.