CM11 Abstract Book
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Case of Calciphylaxis with an Unfavorable Outcome
CASE LETTER 671 However, the present patient exhibited the peculiarity References of an intense inflammatory infiltrate in the dermis rarely seen previously. According to this case, an atypical intense 1. Sitaru C, Zillikens D. Mechanisms of blister induction by autoan- inflammation could be a distinct histopathological feature tibodies. Exp Dermatol. 2005;14:861---75. of trauma-induced pemphigus. Further research is neces- 2. Sagi L, Trau H. The Koebner phenomenon. Clin Dermatol. sary to ascertain if greater inflammation in dermis is more 2011;29:231---6. related to trauma-induced pemphigus as opposed to those 3. Jang HW, Chun SH, Lee JM, Jeon J, Hashimoto T, Kim IH. Radiotherapy-induced pemphigus vulgaris. J Dermatol. not related to trauma. 2014;41:851---2. In conclusion, this report describes a presumably new 4. Daneshpazhooh M, Fatehnejad M, Rahbar Z, Balighi K, case of trauma-induced pemphigus. To the author’s knowl- Ghandi N, Ghiasi M, et al. Trauma-induced pemphigus: a edge, there are no prior reports of pemphigus involving case series of 36 patients. J Dtsch Dermatol Ges. 2016;14: predominantly the breasts with such a peculiar dispo- 166---71. sition. It is proposed that a hypothetical continuous 5. Balighi K, Daneshpazhooh M, Azizpour A, Lajevardi V, trauma with the bra could explain this unique loca- Mohammadi F, Chams-Davatchi C. Koebner phenomenon tion. in pemphigus vulgaris patients. JAAD Case Rep. 2016;2: 419---21. Financial support Fernando Garcia-Souto None declared. Department of Dermatology, Valme University Hospital, Seville, Spain Author’s contributions E-mail: [email protected] Received 14 November 2019; accepted 5 March 2020 Fernando Garcia-Souto: Conception and planning of the manuscript; writing and critical revision of the manuscript; https://doi.org/10.1016/j.abd.2020.03.010 approval of the final version. -
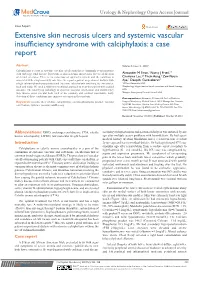
Extensive Skin Necrosis Ulcers and Systemic Vascular Insufficiency Syndrome with Calciphylaxis: a Case Report
Urology & Nephrology Open Access Journal Case Report Open Access Extensive skin necrosis ulcers and systemic vascular insufficiency syndrome with calciphylaxis: a case report Abstract Volume 5 Issue 4 - 2017 Calciphylaxis is a part of systemic vascular calcification that is commonly seen in patients 1 2,3 with end stage renal disease. It presents as skin ischemia and necrosis due to calcification Alexander M Swan, Nancy J Fried, 2,3 2 of dermal arterioles. There is no consensus on optimal treatment and the condition is Charisma Lee, Thein Aung, Zaw Nyein associated with a high mortality rate. Here we report a patient on peritoneal dialysis with Aye,2 Deepthi Gunasekaran2 a high calcium-phosphorus product and extensive calciphylaxis involving the extremities, 1Wilkes University, USA back and scalp. We used a multi-interventional approach to treat this patient with a good 2Nephrology Hypertension Renal transplant and Renal Therapy, outcome. The underlying pathology of systemic vascular calcification and insufficiency USA 3 may involve other vascular beds such as the coronary and cerebral vasculature. Early Rutgers New Jersey Medical School, USA detection of these conditions may improve outcomes in these patents. Correspondence: Alexander M Swan, AA Prof of Medicine, Keywords: necrotic ulcer of skin, calciphylaxis, calcium-phosphorus product, vascular Rutgers New Jersey Medical School, 185 S Orange Ave, Newark, calcification, systemic vascular insufficiency NJ 07103, President, Garden State Kidney Center, 345 Main Street, Woodbridge, NJ 07095, USA, Tel 732-750-5555, Fax 732- 750-5550, Email Received: November 10, 2017 | Published: October 26, 2017 Abbreviations: ESRD, end-stage renal disease; CUA, calcific secondary to hypertension and peritoneal dialys is was initiated 5years uremic arterilopathy; LMWH, low molecular weight heparin ago after multiple access problems with hemodialysis. -

Double Line Image Rotation Amir Hossein Ashtari, Member, IEEE,Mdjannordin,Member, IEEE, and Seyed Mostafa Mousavi Kahaki, Member, IEEE
3370 IEEE TRANSACTIONS ON IMAGE PROCESSING, VOL. 24, NO. 11, NOVEMBER 2015 Double Line Image Rotation Amir Hossein Ashtari, Member, IEEE,MdJanNordin,Member, IEEE, and Seyed Mostafa Mousavi Kahaki, Member, IEEE Abstract— This paper proposes a fast algorithm for rotating rotation transformation has been expressed in (2). The direct images while preserving their quality. The new approach rotates determination of the rotated points is a one-pass method. images based on vertical or horizontal lines in the original image and their rotated equation in the target image. The proposed xr cos α − sin α xt method is a one-pass method that determines a based-line = . (2) yr sin α cos α yt equation in the target image and extracts all corresponding pixels on the base-line. Floating-point multiplications are performed Determining the rotated point directly using a single to calculate the base-line in the target image, and other line function such as (2) is a one-pass technique, whereas cal- coordinates are calculated using integer addition or subtraction and logical justifications from the base-line pixel coordinates in culating the rotated point using multiple functions such the target image. To avoid a heterogeneous distance between as (3), (4), and (5) is a multi-pass technique. Compared with rotated pixels in the target image, each line rotates to two multi-pass methods, one-pass methods are simple and usually adjacent lines. The proposed method yields good performance more accurate [2], [5]. However, although one-pass methods in terms of speed and quality according to the results of an are accurate, they are still inefficient because multiple analysis of the computation speed and accuracy. -

AACE Annual Meeting 2021 Abstracts Editorial Board
June 2021 Volume 27, Number 6S AACE Annual Meeting 2021 Abstracts Editorial board Editor-in-Chief Pauline M. Camacho, MD, FACE Suleiman Mustafa-Kutana, BSC, MB, CHB, MSC Maywood, Illinois, United States Boston, Massachusetts, United States Vin Tangpricha, MD, PhD, FACE Atlanta, Georgia, United States Andrea Coviello, MD, MSE, MMCi Karel Pacak, MD, PhD, DSc Durham, North Carolina, United States Bethesda, Maryland, United States Associate Editors Natalie E. Cusano, MD, MS Amanda Powell, MD Maria Papaleontiou, MD New York, New York, United States Boston, Massachusetts, United States Ann Arbor, Michigan, United States Tobias Else, MD Gregory Randolph, MD Melissa Putman, MD Ann Arbor, Michigan, United States Boston, Massachusetts, United States Boston, Massachusetts, United States Vahab Fatourechi, MD Daniel J. Rubin, MD, MSc Harold Rosen, MD Rochester, Minnesota, United States Philadelphia, Pennsylvania, United States Boston, Massachusetts, United States Ruth Freeman, MD Joshua D. Safer, MD Nicholas Tritos, MD, DS, FACP, FACE New York, New York, United States New York, New York, United States Boston, Massachusetts, United States Rajesh K. Garg, MD Pankaj Shah, MD Boston, Massachusetts, United States Staff Rochester, Minnesota, United States Eliza B. Geer, MD Joseph L. Shaker, MD Paul A. Markowski New York, New York, United States Milwaukee, Wisconsin, United States CEO Roma Gianchandani, MD Lance Sloan, MD, MS Elizabeth Lepkowski Ann Arbor, Michigan, United States Lufkin, Texas, United States Chief Learning Officer Martin M. Grajower, MD, FACP, FACE Takara L. Stanley, MD Lori Clawges The Bronx, New York, United States Boston, Massachusetts, United States Senior Managing Editor Allen S. Ho, MD Devin Steenkamp, MD Corrie Williams Los Angeles, California, United States Boston, Massachusetts, United States Peer Review Manager Michael F. -

Management of the Incidental Renal Mass on CT: a White Paper of the ACR Incidental Findings Committee
ORIGINAL ARTICLE Management of the Incidental Renal Mass on CT: A White Paper of the ACR Incidental Findings Committee Brian R. Herts, MDa, Stuart G. Silverman, MDb, Nicole M. Hindman, MDc, Robert G. Uzzo, MDd, Robert P. Hartman, MDe, Gary M. Israel, MD f, Deborah A. Baumgarten, MD, MPHg, Lincoln L. Berland, MDh, Pari V. Pandharipande, MD, MPHi Abstract The ACR Incidental Findings Committee (IFC) presents recommendations for renal masses that are incidentally detected on CT. These recommendations represent an update from the renal component of the JACR 2010 white paper on managing incidental findings in the adrenal glands, kidneys, liver, and pancreas. The Renal Subcommittee, consisting of six abdominal radiologists and one urologist, developed this algorithm. The recommendations draw from published evidence and expert opinion and were finalized by informal iterative consensus. Each flowchart within the algorithm describes imaging features that identify when there is a need for additional imaging, surveillance, or referral for management. Our goal is to improve quality of care by providing guidance for managing incidentally detected renal masses. Key Words: Kidney, renal, small renal mass, cyst, Bosniak classification, incidental finding J Am Coll Radiol 2017;-:---. Copyright Ó 2017 American College of Radiology OVERVIEW OF THE ACR INCIDENTAL Findings Committee (IFC) generated its first white paper FINDINGS PROJECT in 2010, addressing four algorithms for managing inci- The core objectives of the Incidental Findings Project are dental pancreatic, adrenal, kidney, and liver findings [1]. to (1) develop consensus on patient characteristics and imaging features that are required to characterize an THE CONSENSUS PROCESS: THE INCIDENTAL incidental finding, (2) provide guidance to manage such RENAL MASS ALGORITHM findings in ways that balance the risks and benefits to The current publication represents the first revision of the patients, (3) recommend reporting terms that reflect the IFC’s recommendations on incidental renal masses. -

How to Win Back America's Transit Riders
Who’sDrew to add cover On Board 11 Charts done 2019 How to Win Back America’s Transit Riders TransitCenter works to improve public transit in ways that make cities more just, environmentally sustainable, and economically vibrant. We believe that fresh thinking can change the transportation landscape and improve the overall livability of cities. We commission and conduct research, convene events, and produce publications that inform and improve public transit and urban transportation. For more information, please visit www.transitcenter.org. Publication Date: February 2019 1 Whitehall Street, 17th Floor, New York, NY 10004 www.TransitCenter.org @transitcenter Facebook.com/transitctr Who’s On Board 2019 How to Win Back America’s Transit Riders Acknowledgments Steven Higashide and Mary Buchanan of TransitCenter are the authors of this report. David Bragdon and Tabitha Decker provided additional writing and editorial review. The authors are grateful for thoughtful review from Evelyn Blumenberg, Nicholas Klein, Alan Lehto, Tom Mills, Michelle Poyourow, Jarrett Walker, Aaron Weinstein, and TransitCenter’s Jon Orcutt and Hayley Richardson. Resource Systems Group (RSG) served as the lead research consultant, conducting focus groups, developing the survey questionnaire, and analyzing survey results. The authors gratefully acknowledge RSG’s project manager Ben Cummins. Greg Spitz and Alex Levin of RSG and Jed Lam of Aeffect also contributed to the research. The authors thank Emily Drexler of the Chicago Transit Authority for assistance with recruiting for focus groups, as well as Linda Young and Preeti Shankar of the Center for Neighborhood Technology for providing AllTransit data. Contents Executive Summary 1 All Transit Ridership is Local 6 Findings 14 1. -

A Cross Sectional Study Ofrenal Involvement in Tuberous Sclerosis
480 Med Genet 1996;33:480-484 A cross sectional study of renal involvement in tuberous sclerosis J Med Genet: first published as 10.1136/jmg.33.6.480 on 1 June 1996. Downloaded from J A Cook, K Oliver, R F Mueller, J Sampson Abstract There are two characteristic types of renal Renal disease is a frequent manifestation involvement in persons with TSC. (1) An- oftuberous sclerosis (TSC) and yet little is giomyolipomas. These are benign neoplasms known about its true prevalence or natural composed of mature adipose tissue, thick history. We reviewed the notes of 139 walled blood vessels, and smooth muscle in people with TSC, who had presented with- varying proportions. In the general population out renal symptoms, but who had been they are a rare finding affecting predominantly investigated by renal ultrasound. In- women (80%) in the third to fifth decade. formation on the frequency, type, and About 50% of people with angiomyolipomas symptomatology of renal involvement was have no stigmata of TSC and usually have retrieved. a large, single angiomyolipoma.6 In TSC the The prevalence ofrenal involvement was angiomyolipomas tend to be small, multiple, 61%. Angiomyolipomas were detected in and bilateral.7 Stillwell et al7 suggested that 49%, renal cysts in 32%, and renal car- there was an increase in the prevalence of cinoma in 2-2%. The prevalence of an- angiomyolipomas with age but only a limited giomyolipoma was positively correlated number of persons with TSC were studied. with age, compatible with a two hit aeti- (2) Renal cysts. These have a characteristic ology. -

ACR Appropriateness Criteria: Indeterminate Renal Mass
Revised 2020 American College of Radiology ACR Appropriateness Criteria® Indeterminate Renal Mass Variant 1: Indeterminate renal mass. No contraindication to either iodinated CT contrast or gadolinium- based MR intravenous contrast. Initial imaging. Procedure Appropriateness Category Relative Radiation Level US abdomen with IV contrast Usually Appropriate O MRI abdomen without and with IV contrast Usually Appropriate O CT abdomen without and with IV contrast Usually Appropriate ☢☢☢☢ US kidneys retroperitoneal May Be Appropriate O MRI abdomen without IV contrast May Be Appropriate O CT abdomen with IV contrast May Be Appropriate ☢☢☢ CT abdomen without IV contrast May Be Appropriate ☢☢☢ CTU without and with IV contrast May Be Appropriate ☢☢☢☢ Arteriography kidney Usually Not Appropriate ☢☢☢ Radiography intravenous urography Usually Not Appropriate ☢☢☢ Biopsy renal mass Usually Not Appropriate Varies MRU without and with IV contrast Usually Not Appropriate O Variant 2: Indeterminate renal mass. Contraindication to both iodinated CT and gadolinium-based MR intravenous contrast. Initial imaging. Procedure Appropriateness Category Relative Radiation Level US abdomen with IV contrast Usually Appropriate O US kidneys retroperitoneal Usually Appropriate O MRI abdomen without IV contrast Usually Appropriate O CT abdomen without IV contrast May Be Appropriate ☢☢☢ Arteriography kidney Usually Not Appropriate ☢☢☢ Radiography intravenous urography Usually Not Appropriate ☢☢☢ Biopsy renal mass Usually Not Appropriate Varies MRI abdomen without and with IV contrast Usually Not Appropriate O MRU without and with IV contrast Usually Not Appropriate O CT abdomen with IV contrast Usually Not Appropriate ☢☢☢ CT abdomen without and with IV contrast Usually Not Appropriate ☢☢☢☢ CTU without and with IV contrast Usually Not Appropriate ☢☢☢☢ ACR Appropriateness Criteria® 1 Indeterminate Renal Mass Variant 3: Indeterminate renal mass. -

National Assessment of Urban Rail Noise
, REPORT NO UMTA-MA-06-0099-79-2 JJ DEPARTMENT OF NATIONAL ASSESSMENT OF TRANSPORTATION URBAN RAIL NOISE J UN 6 */9/y Gregory Ch i s holm LIBRARY Herbert Boge n Michael Di nn i ng Michael Prim eggi a . of T ra ns port a t i o n U S . department Research and Special P rogr ams Admi n i s t r a t i o n Transportati on Sys terns Cen ter i 021 42 Cambr dge , MA Of TRaa. MARC H 1979 FINAL REPORT DOCUMENT IS AVAILABLE TO THE U.S. PUBLIC THROUGH THE NATIONAL TECHNICAL INFORMATION SERVICE, SPRINGFIELD, VIRGINIA 22161 Prepared for U.S. DEPARTMENT OF TRANSPORTATION URBAN MASS TRANSPORTATION ADMINISTRATION Office of Technology Development and Deployment Office of Rail and Construction Technology Washington DC 20590 NOTICE This document is disseminated under the sponsorship of the Department of Transportation in the interest of information exchange. The United States Govern- ment assumes no liability for its contents or use thereof. NOTICE The United States Government does not endorse pro- ducts or manufacturers. Trade or manufacturers' names appear herein solely because they are con- sidered essential to the object of this report. Technico! Report Documentation Pag 1 . Report N o 2 Government Accession No. 3. Recipient s Cotolog No. UMTA-MA-06-0Q9 9-7 9-2 S 5. Report Date natioVal assessment OF URBAN RAIL NOISE March 1979 6. Performing Orgomzotion Code 8. Performing Orgoni zotion Report No 7. Author s' Gregory Chisholm, et al. DOT-TSC-UMTA-7 9-10 9. Performing Orgom lotion Nome and Address 10 Work Unit No IT RAIS) U.S. -

East-West Corridor High Capacity Transit Plan Rapid Transit Evaluation Results
East-West Corridor High Capacity Transit Plan Rapid Transit Evaluation Results About the Corridor The AECOM consultant team conducted a high-level analysis of commuter rail, light rail transit (LRT), streetcar and bus rapid transit (BRT) to determine the most appropriate mode for the East- West Corridor. Based on the corridor fit, ridership capacity, cost per mile to build/operate and available right-of-way, BRT will move forward for more detailed analysis. This fact sheet provides, in more detail, how BRT and LRT compared and why BRT was determined to be the best fit. BRT with LRT Screening Results Below are the similarities and differences between bus rapid transit (BRT) and light rail transit (LRT). Features Bus Rapid Transit (BRT) Light Rail Transit (LRT) Service Frequency Frequent service during peak hrs. (5–15 min.) Frequent service during peak hrs. (5–15 min.) Typical Corridor Length 5–25 mi. 10–20 mi. Range of Operating Speed 25–55 MPH 30–55 MPH Right-of-Way Dedicated lanes and/or mixed traffic Dedicated lanes with overhead electrical systems Typical Station Spacing ½ and one mile apart One mile apart, outside of downtowns Level boarding at high-quality stations Level boarding at high-quality stations Vehicle Types 40- or 60-ft. buses that have multiple doors 1–3 car trains; low floor vehicles Technology Traffic signal priority Traffic signal priority Real-time passenger info Real-time passenger info Off-board fare payment Off-board fare payment Typical Operating Cost per Hr. $100–$200 $200–$400 Typical Capital Cost per Mi. $2.5 million–$20 million $140 million+ Ridership Capacity by Mode Best Poor Current East-West Corridor Ridership (6.9k–8.7k riders) Modern Streetcar Light Rail Transit (1.5k–6k riders) (20k–90k riders) Bus Rapid Transit (4k–15k riders) Commuter Rail (3k–20k riders) Ridership Mode Capacity by 0 5,000 10,000 15,000 20,000 25,000 30,000 35,000 40,000 45,000 50,000 The chart above demonstrates that BRT and commuter rail both have the needed capacity to meet ridership needs. -
Understanding Calcinosis and Calciphylaxis
PRACTICE DEVELOPMENT Understanding calcinosis and calciphylaxis KEY WORDS Calcinosis cutis is a rare cause of non-healing leg ulceration. There are many factors Calcinosis cutis that can delay the healing of venous leg ulceration and the deposition of calcium in Calciphylaxis the skin known as calcinosis cutis is one of these factors. There are five distinct forms: Warfarin-induced skin dystrophic calcification, metastatic calcification, idiopathic calcification, iatrogenic necrosis calcification and calciphylaxis. Warfarin skin necrosis has common clinical features with calciphylaxis and is therefore included in this article, which describes the types of calcinosis cutis, their clinical presentations and limited treatment options. The aim is to highlight these unusual causes and to assist healthcare professionals when faced with a non-healing ulcer. eg ulceration can be defined as a defect in neurotransmission and the blood coagulation the dermis located on the leg (Franks et al, pathway. At a cellular level, it is implicated in 2016). Leg ulceration is a significant clinical cell-to-cell communication (Walshe and Fairley, Lproblem with the majority attributing venous 1995). In the skin, it is specifically concerned with hypertension as the underlying disease process with keratinocyte proliferation, differentiation and venous leg ulceration affecting 1% of the population adhesion (Smith and Yamada, 2002). in the western world (Posnett et al, 2009). However, The level of serum calcium is closely there is a multitude of causative factors of leg ulcers, controlled by the parathyroid hormone. with the term leg ulcer purely signifying the clinical Regardless of this regulation, it is possible for manifestation and not the underlying aetiology. -

95F325afe6daa80601f51b046b3
D.M. DEGREE EXAMINATIONEPHROLOGY-PAPER - I Basic Sciences And Applied Nephrology 30 m 1) Discuss renal acid handling and pathomechanism of renal tubular acidosis 2) Discuss the role of ‘Klotho – FGF 23 complex’ in health and chronic kidney disease 3) Enumerate causes for hypokalemia and describe in detail about potassium homeostasis 4) The ageing kidney 5) Discuss the role of complement in renal disease 6) Discuss in detail the pathogenesis of membranous glomerulonephritis and its management 7) Discuss the etiopathogenesis of the syndrome of inappropriate secretion of anti diuretic hormone. How can it be recognized and managed? 8) Describe Nephron dosing and its clinical relevance 9) Discuss the relevant physiological changes of pregnancy and pathogenesis of toxemia of Pregnancy 10) Discuss in brief Physiology of Vitamin D, vitamin D analogues and their role in nephrology practice 11) Discuss the pathogenesis, evaluation and management of disorders of micturition 12) Discuss in brief embryological development of the kidney and its clinical relevance 13) Discuss renal handling of sodium and diagnostic approach to hyponatremia 14) Discuss aetiology, pathogenesis, clinical features and management of hepato renal syndrome 15) Discuss the etiopathogenesis of the syndrome of inappropriate secretion of anti diuretic hormone. How can it be recognized and managed? 16) Describe the etiology, clinical manifestations, diagnosis & management of metabolic alkalosis 17) Describe the mechanism and types of proteinuria. What are the therapeutic interventions that may be used to reduce proteinuria 18) Describe the renin-angiotensin system and its physiologic role. Discuss its role in the pathophysiology of renal disease 19) Discuss pathophysiology of proteinuria, classify proteinuria, name diseases which produces different types of proteinuria.