Restoring Sensation in Human Upper Extremity Amputees Using Chronic Peripheral Nerve Interfaces
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prosthetics, Exoskeletons, and Rehabilitation
Prosthetics, Exoskeletons, and Rehabilitation Now and for the Future BY BRIAN DELLON AND YOKY MATSUOKA n the near future, the need for assistive robotic devices will increase. During the 1950s, only 4.9% of the world’s population was over the age of 65. Today, almost 20% is over 65 and this © iSWOOP, COREL CORP. figure is predicted to exceed 35% by 2050. This demographic shift in world population will impose a large burden of care to treat the health risks associated with aging. Robotic solu- tions will help tackle these issues and enable the elderly to regain their independence and Imaintain an enriching, fulfilling lifestyle. The benefits of robotic systems are not limited to healthcare. Applying these technologies to military applications allows soldiers to carry more and walk further. However, the style of recent wars creates additional needs for robotic assistance: while the death toll has been dramatically reduced (10% of injured died in Iraq compared to 30% in World War II), 6% of injury survivors required amputation (compared to 3% in previous wars) and 20% of injury survivors will need permanent assistance for the rest of their lives. Robotic systems for assistance and rehabilitation focus on providing missing movements and sensing, providing safer environments, and providing environments that make regaining move- ment-related function easier and faster. Robotic prosthetics and exoskeletons will provide dex- terity, natural mobility, and sense of touch to missing or paralyzed limbs. Individuals suffering from hip or knee conditions can use a robotically intelligent walker or wheelchair to help pre- vent common accidents like slipping. -

Continuous Vocalization Control of a Full-Scale Assistive Robot
The Fourth IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics Roma, Italy. June 24-27, 2012 Continuous Vocalization Control Of A Full-Scale Assistive Robot Mike Chung*, Eric Rombokas*, Qi An, Yoky Matsuoka and Jeff Bilmes Abstract— We present a physical robotic arm performing real-world tasks using continuous non-verbal vocalizations for control. Vocalization control provides fewer degrees of control freedom than are necessary to directly control complex robotic platforms. To bridge this gap, we evaluated three control methods: direct joint angle control of a selectable subset of joints, inverse kinematics control of the end effector, and control in a reduced-dimensionality synergy space. The synergy method is inspired by neural solutions to biological body redundancy problems. We conducted several evaluations of the three methods involving the real-world tasks of water bottle recycling and grocery bag moving. Users with no prior exposure to the system were able to perform these tasks effectively and Fig. 1. Experimental setup for the two real-world tasks. (a) In the pick- were able to learn to be more efficient. This study demonstrates and-place task, users move water bottles into a trash can. (b) In the bag the feasibility of continuous non-verbal vocalizations for control moving task, users pick up a grocery bag by the handles and move it to the of a full-scale assitive robot in a realistic context. specified region of another table. In the United States, there are over a quarter million individuals with spinal cord injuries, 47% of which are rely heavily on robotic autonomy in human-environments, quadriplegic [1] (i.e., with restricted use of their upper limbs which is still an unsolved research problem [4], [5]. -

The Handbook of Information Security for Advanced Neuroprosthetics, ISBN 978-0-692-50161-0, Indianapolis: Synthypnion Academic, 2015, Pp
Chapter 4, "An Information Security Device Ontology for Advanced Neuroprosthetics," an excerpt from Gladden, Matthew E., The Handbook of Information Security for Advanced Neuroprosthetics, ISBN 978-0-692-50161-0, Indianapolis: Synthypnion Academic, 2015, pp. 107-27. Introduction to the ontology In order to create an effective information security framework for neuro- prosthetics, it is necessary to first develop an appropriate ontology for such devices. Such an ontology should define the range of possible values for rele- vant characteristics that are critical for information security and whose values can vary across the universe of neuroprosthetic devices. The ontology should include both the physical characteristics, processes, and contexts and rela- tionships possessed by such devices; it thus differs from (and is necessary for the effective development of) security configuration checklists1 that would be used to configure particular neuroprosthetic devices for secure operation in their individual human hosts. Scholars and device manufacturers have made efforts to create general on- tologies for robotic systems2 and mobile devices,3 however there has not yet been developed an ontology that focuses on the information security charac- teristics of neuroprosthetic devices. In part, the lack of creation of such for- mal tools is an effect of the relatively low level of interaction and collabora- tion between the fields of information security and biomedical engineering.4 By synthesizing information gathered from a review of current literature and practice in the fields of neuroprosthetics, implantable computing, and information security, we develop one such ontology within this chapter. Note that because many neuroprosthetic devices are also computers, mobile de- vices, or implantable medical devices, any generalized information security ontology that is applicable to computers, mobile devices, or IMDs will also 1 NIST SP 800-70, Rev. -

Determination of the Arm Orientation for Brain-Machine Interface Prosthetics
2005 IEEE International Workshop on Robots and Human Interactive Communication Determination of the Arm Orientation for Brain-Machine Interface Prosthetics Sam Clanton Joseph Laws Yoky Matsuoka Robotics Institute / School of Medicine Electrical and Computer Engineering The Robotics Institute CMU / Univ. of Pittsburgh Carnegie Mellon University Carnegie Mellon University Pittsburgh,PA, USA, 15213 Pittsburgh,PA, USA, 15213 Pittsburgh,PA, USA, 15213 [email protected] [email protected] [email protected] Controlling prosthetics with brain-machine injury. The substantial prevalence of these disorders, in interface will soon become the most natural way to combination with their severity, makes it imperative that restore limb function to those who suffer from satisfactory therapies for these conditions are developed. neurodegenerative disease or injury. Here, we first Current therapies for these patients include both various discuss the development of neural signal processing attempts at repair or reconnection of the dysfunctional systems for brain-machine interfaces which provide neuromuscular systems, as well as the use of artificial control within the Cartesian (extrinsic) frames of devices to replace the function of the defunct motion. Then we justify the development of systems extremities. that provide control using the kinematic (intrinsic) While some success has been made in regeneration frames of motion of the manipulator prosthetic of neuromuscular systems to restore the previous device. An experiment to create a general model of function of the body, our work focuses on the goal of natural arm motion is presented, along with its replacing the deficient motor system with a prosthetic application to brain-machine interfaces. system which attempts to reproduce the capabilities of the original. -

Neurobotics for Women Recruitment and Retention
日 本 ロ ボ ッ ト学 会 誌VoL24No.J.pp.585-587.2006 585 解 説 Neurobotics for Women Recruitment and Retention Yoky Matsuoka* *The Robotics Institute, Carnegie Mellon University scientific understanding of the human body and using 1. Introduction it to rehabilitate arid assist people through robotic de- Girls and women often try to stay as far away as pos- vices. Because of its societal ramifications. Neurobotics sible from being associated with the word •grobot•h for can both be used to recruit women who want a career a good reason. Socially, boys with sophisticated robots that mixes technology and humans and to retain women may become popular, while girls with robots may be la- who want a career that is worth having even if it means beled as geeks [1]. In college, women who are capable of that the time is spent away from their own children be- performing equally with men may purposely do worse cause they are also helping and changing other people's in math and engineering when a stereotype threat ex- lives. ists [2] . Even if women overcome these stereotype issues 2. Neurobotics and pursue robotics research, a male dominant work- place is awaiting to make the already difficult tasks of The field of Neurobotics focuses on the algorithms balancing career and family an even harder task. For and designs of a robot-human closed loop system to these reasons, there are very few women in the field of alter the neural control of movement as aaway to reha- robotics; and because of the lack of role models, it makes bilitate, assist, and enhance human motor control and it even more intimidating for women to enter the field. -

Plug-And-Play Supervisory Control Using Muscle and Brain Signals for Real-Time Gesture and Error Detection
Plug-and-Play Supervisory Control Using Muscle and Brain Signals for Real-Time Gesture and Error Detection Joseph DelPreto∗, Andres F. Salazar-Gomez∗, Stephanie Gil∗, Ramin M. Hasaniy, Frank H. Guentherz, and Daniela Rus∗ Abstract—Control of robots in safety-critical tasks and situa- tions where costly errors may occur is paramount for realizing the vision of pervasive human-robot collaborations. For these cases, the ability to use human cognition in the loop can be key for recuperating safe robot operation. This paper combines two streams of human biosignals, electrical muscle and brain activity via EMG and EEG, respectively, to achieve fast and accurate human intervention in a supervisory control task. In particular, this paper presents an end-to-end system for continuous rolling- window classification of gestures that allows the human to actively correct the robot on demand, discrete classification of Error-Related Potential signals (unconsciously produced by the human supervisor’s brain when observing a robot error), and a framework that integrates these two classification streams for fast and effective human intervention. The system also allows “plug-and-play” operation, demonstrating accurate performance even with new users whose biosignals have not been used for Fig. 1: A user supervises and controls an autonomous robot using training the classifiers. The resulting hybrid control system for brain signals to detect mistakes and muscle signals to select targets.1 safety-critical situations is evaluated with 7 untrained human subjects in a supervisory control scenario where an autonomous robot performs a multi-target selection task. Despite their potential, both biosignals have significant shortcomings as reliable sources of fast human-robot com- I. -

Conference Digest
2012 IEEE International Conference on Robotics and Biomimetics (ROBIO 2012) Conference Digest December 11-14, 2012 Guangzhou, China Sponsored by IEEE Robotics and Automation Society (RAS) South China University of Technology (SCUT) National Natural Science Foundation of China (NSFC) State Key Laboratory of Robotics and System, HIT IEEE Systems, Man, and Cybernetics Society (SMC) Robotics Society of Japan (RSJ) Japan Society of Mechanical Engineering (JSME) Guangdong Mechanical Engineering Society (GDMES) ROBIO 2012 PROCEEDINGS Additional copies may be ordered from: IEEE Sevice Center 445 Hoes Lane P.O. Box 1331 Piscataway, NJ 08855-1331 USA. IEEE Catalog Number: CFP12581-ART ISBN: 978-1-4673-2127-3 IEEE Catalog Number (USB drive): CFP12581-USB Copyright and Reprint Permission: Abstracting is permitted with credit to the source. Libraries are permitted to pho- tocopy beyond the limit of U.S. copyright law for private use of patrons those articles in this volume that carry a code at the bottom of the first page, provided the per-copy fee indicated in the code is paid through Copyright Clearance Center, 222 Rosewood Drive, Danvers, MA 01923. For other copying, reprint or republication permission, write to IEEE Copyrights Manager, IEEE Operations Center, 445 Hoes Lane, P.P. Box 1331, Piscataway, NJ 08855-1331. All rights reserved. Copyright ©2012 by the Institute of Electrical and Electronics Engineers, Inc. The Institute of Electrical and Electronics Engineers, Inc Welcome Message On behalf of the IEEE ROBIO 2012 Organizing Committee, we would like to extend a warm welcome to you all to the 2012 IEEE International Conference on Robotics and Biomimetics. -
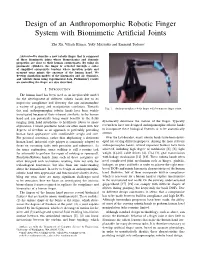
Design of an Anthropomorphic Robotic Finger System with Biomimetic Artificial Joints
Design of an Anthropomorphic Robotic Finger System with Biomimetic Artificial Joints Zhe Xu, Vikash Kumar, Yoky Matsuoka and Emanuel Todorov Abstract—We describe a new robotic finger that is composed of three biomimetic joints whose biomechanics and dynamic properties are close to their human counterparts. By using six pneumatic cylinders, the finger is actuated through a series of simplified antagonistic tendons whose insertion points and moment arms mimic the anatomy of the human hand. We develop simulation models of the kinematics and air dynamics, and validate them using experimental data. Preliminary results on controlling the finger are also described. I. INTRODUCTION The human hand has been used as an irreplaceable model for the development of different robotic hands due to its impressive compliance and dexterity that can accommodate a variety of gasping and manipulation conditions. Towards Fig. 1. Anthropomorphic robotic finger with biomimetic finger joints. this end, anthropomorphic robotic hands have been widely investigated because of their inherent similarity to the human hand and can potentially bring many benefits to the fields ranging from hand prosthetics to healthcare robots to space dynamically determine the motion of the finger. Typically exploration. Current prosthetic hands are often made with few researchers have not designed anthropomorphic robotic hands degrees of freedom as an approach to preferably providing to incorporate these biological features or to be anatomically human hand appearance with comfortable weight and size. correct. For personal assistance, rather than duplicating a dexterous Over the last decades, many robotic hands have been devel- human hand, industrial style gripper is commonly adopted to oped for serving different purposes. -

Springer Tracts in Advanced Robotics
Springer Tracts in Advanced Robotics Volume 95 Series editors B. Siciliano, Napoli, Italy O. Khatib, Stanford, USA Editorial Advisory Board O. Brock, Berlin, Germany H. Bruyninckx, Leuven, Belgium R. Chatila, Toulouse, France H. Christensen, Atlanta, USA P. Corke, Kelvin Grove, Australia P. Dario, Pisa, Italy R. Dillmann, Karlsruhe, Germany K. Goldberg, Berkeley, USA J. Hollerbach, Salt Lake City, USA M. Kaneko, Osaka, Japan L. Kavraki, Houston, USA V. Kumar, Philadelphia, USA S. Lee, Seoul, South Korea F. Park, Seoul, South Korea T. Salcudean, Vancouver, Canada R. Siegwart, Zurich, Switzerland G. Sukhatme, Los Angeles, USA S. Thrun, Stanford, USA Y. Xu, Hong Kong, People’s Republic of China S. Yuta, Tsukuba, Japan For further volumes: http://www.springer.com/series/5208 STAR (Springer Tracts in Advanced Robotics) has been promoted under the auspices of EURON (European Robotics Research Network) Ravi Balasubramanian • Veronica J. Santos Editors The Human Hand as an Inspiration for Robot Hand Development 123 Editors Ravi Balasubramanian Veronica J. Santos Oregon State University Mechanical and Aerospace Engineering Corvallis Arizona State University USA Tempe USA ISSN 1610-7438 ISSN 1610-742X (electronic) ISBN 978-3-319-03016-6 ISBN 978-3-319-03017-3 (eBook) DOI 10.1007/978-3-319-03017-3 Springer Cham Heidelberg New York Dordrecht London Library of Congress Control Number: 2013957707 Ó Springer International Publishing Switzerland 2014 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. -

A New Electrode Technology for Neuro-Robotic Interfaces Alik Sunil Widge CMU-RI-TR-07-03
Self-Assembled Monolayers of Polythiophene “Molecular Wires”: A New Electrode Technology for Neuro-Robotic Interfaces Alik Sunil Widge CMU-RI-TR-07-03 Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Robotics The Robotics Institute and Center for the Neural Basis of Cognition Carnegie Mellon University Pittsburgh, Pennsylvania 15213 January 3rd, 2007 Dr. Yoky Matsuoka, Thesis Committee Chair Dr. Kaigham Gabriel, Co-advisor Dr. Xinyan ”Tracy” Cui, University of Pittsburgh (external) Dr. Carl Lagenaur, University of Pittsburgh (external) Dr. Lee Weiss Copyright 2007 by Alik Widge. All rights reserved. Alik Sunil Widge Self-Assembled Monolayers of Polythiophene “Molecular Wires”: A New Electrode Technology for Neuro-Robotic Interfaces Abstract This thesis presents the proof of concept of a new type of electrode for inter- faces between living nervous systems and electronic devices (“neuro-robotic interfaces”). Such interfaces have long been pursued due to their high clin- ical and scientific value. However, progress has been hindered by inade- quate performance of the implanted electrodes that bridge biological, ion- based electricity and analog/digital electronics. These electrodes provoke inflammatory reactions in surrounding tissue and often cause detrimental effects when stimulating neurons to deliver information. The most promis- ing approach to improving electrode biocompatibility involves electrically polymerizing conductive polymers with biomolecules on metal electrodes. These coatings improve -

Brain Waves, a Cultural History: Oscillations of Neuroscience, Technology, Telepathy, and Transcendence Caitlin Shure Submitted
Brain Waves, A Cultural History: Oscillations of Neuroscience, Technology, Telepathy, and Transcendence Caitlin Shure Submitted in partial fulfillment of the requirements for the degree of Doctorate of Philosophy under the Executive Committee of the Graduate School of Arts and Sciences COLUMBIA UNIVERSITY 2018 © 2018 Caitlin Shure All rights reserved ABSTRACT Brain Waves, A Cultural History: Oscillations of Neuroscience, Technology, Telepathy, and Transcendence Caitlin Shure This project proceeds from a narrow question: What, if anything, is a brain wave? Beguiling in its simplicity, this question prompts a cultural-historical investigation that spans over 150 years of science, technology, and society. Proposed in 1869, the original theory of brain waves cites etheric undulations to explain reports of apparent thought transference. Though most modern thinkers no longer believe in outright telepathy, I argue that dreams of thought transmission and other mental miracles subtly persist—not in obscure and occult circles, but at the forefront of technoscience. A hybrid of science and fiction, brain waves represent an ideal subject through which to explore the ways in which technical language shrouds spiritual dreams. Today, the phrase “brain waves” often function as shorthand for electrical changes in the brain, particularly in the context of technologies that purport to “read” some aspect of mental function, or to transmit neural data to a digital device. While such technologies appear uniquely modern, the history of brain waves reveals that they are merely the millennial incarnation of a much older hope—a hope for transmission and transcendence via the brain’s emanations. TABLE OF CONTENTS LIST OF FIGURES AND PHOTOGRAPHS .................................................................. -

Security in Brain-Computer Interfaces: State-Of-The-Art, Opportunities, and Future Challenges
Security in Brain-Computer Interfaces: State-Of-The-Art, Opportunities, and Future Challenges SERGIO LÓPEZ BERNAL, University of Murcia - Departamento de Ingeniería de la Información y las Comunicaciones ALBERTO HUERTAS CELDRÁN, Waterford Institute of Technology - Telecommunication Software and Systems Group, and University of Zurich - Department of Informatics GREGORIO MARTÍNEZ PÉREZ, University of Murcia - Departamento de Ingeniería de la Información y las Comunicaciones MICHAEL TAYNNAN BARROS, University of Essex - School of Computer Science and Electronic Engineering, and Tampere University - CBIG/BioMediTech in the Faculty of Medicine and Health Technology SASITHARAN BALASUBRAMANIAM, Waterford Institute of Technology - Telecommunication Software and Systems Group, and RCSI University of Medicine and Health Sciences - FutureNeuro, the SFI Research Centre for Chronic and Rare Neurological Diseases Brain-Computer Interfaces (BCIs) have significantly improved the patients’ quality of life by restoring damaged hearing, sight, and movement capabilities. After evolving their application scenarios, the current trend of BCI is to enable new innovative brain-to-brain and brain-to-the-Internet communication paradigms. This technological advancement generates opportunities for attackers since users’ personal information and physical integrity could be under tremendous risk. This work presents the existing versions of the BCI life-cycle and homogenizes them in a new approach that overcomes current limitations. After that, we offer a qualitative