Poliomyelitis in 1953
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Statute of the Office of the United Nations High Commissioner for Refugees
s t a t u t e of the office of the united nations high commissioner Published by: for refugees UNHCR Communications and Public Information Service P.O. Box 2500 1211 Geneva 2 Switzerland www.unhcr.org For information and inquiries, please contact: Communications and Public Information Service [email protected] General Assembly Resolution 428 (V) of 14 December 1950 statute of the office of the united nations high commissioner for refugees with an Introductory Note by the Office of the United Nations High Commissioner for Refugees s t a t u t e o f t h e o f f i c e o f t h e u n h c r 1 introductory note by the Office of the United Nations High Commissioner for Refugees (UNHCR) In ResolutIon 319 (IV) , of 3 December 1949, the United Nations General Assembly decided to establish a High Commissioner’s Office for Refugees as of 1 January 1951. The Statute of the Office of the United Nations High Commissioner for Refugees was adopted by the General Assembly on 14 December 1950 as Annex to Resolution 428 (V).n I this Resolution, reproduced on page 4, the Assembly also called upon the Governments to cooperate with the High Com- missioner in the performance of his or her functions concerning refugees fall- ing under the competence of the Office. In accordance with the Statute, the work of the High Commissioner is humanitarian and social and of an entirely non-political character. The functions of the High Commissioner are defined in the Statute and in various Resolutions subsequently adopted by the General Assembly. -

1953 the Text of the GATT Selected GATT
FIRST EDITION GATT BIBLIOGRAPHY 1947 - 1953 The text of the GATT Selected GATT publications A chronological list of references to the GATT GATT Secretariat Palais des Nations Gene va Switzerland March 1954 MGT/7/54 GATT BIBLIOGRAPHY This bibliography is a list of books, pamphlets, articles in periodicals, newspaper reports and editorials, and miscellaneous items including texts of lectures, which refer to the General Agreement on Tariffs and Trade. It covers a period of approximately seven years. For six of these years - from the beginning of 1948 - the GATT has been in operation. The purpose of the list is a practical one: to provide sources of reference for historians, researchers and students. The list, it must be emphasized, is limited to the formation and operation of the GATT; for œasons •»f length, the history of the Havana Charter and its preparation and references to the proposed International Trade Organization, which has not been brought into being, have been somewhat rigidly excluded, while emphasis has been put en references that show the operational aspects of the GATT. The bibliography is divided into the following sections: 1. the text of the GATT and governmental publications; 2. selected GATT publications; (the full list of GATT publications is .obtainable from the secretariat on request) 3. a chronological listing of references to the GATT. This has been subdivided into the following periods, the references being listed alphabetically in each period: 1947 including the Geneva tariff negotiations (April- August) and -

How Has Your State Pension Age Changed?
Increase in state pension age Pensions Act 2011 WOMEN Pensions Act 2011 Date of Birth Old pension date New pension date Delay on 1995 Act 06 April 1953 to 05 May 1953 06 May 2016 06 July 2016 2 months 06 May 1953 to 05 June 1953 06 July 2016 06 November 2016 4 months 06 June 1953 to 05 July 1953 06 September 2016 06 March 2017 6 months 06 July 1953 to 05 August 1953 06 November 2016 06 July 2017 8 months 06 August 1953 to 05 September 1953 06 January 2017 06 November 2017 10 months 06 September 1953 to 05 October 1953 06 March 2017 06 March 2018 1 year 06 October 1953 to 05 November 1953 06 May 2017 06 July 2018 1 yr 2 months 06 November 1953 to 05 December 1953 06 July 2017 06 November 2018 1 yr 4 months 06 December 1953 to 05 January 1954 06 September 2017 06 March 2019 1 yr 6 months 06 January 1954 to 05 February 1954 06 November 2017 06 May 2019 1yr 6 months 06 February 1954 to 05 March 1954 06 January 2018 06 July 2019 1yr 6 months 06 March 1954 to 05 April 1954 06 March 2018 06 September 2019 1yr 6 months 06 April 1954 to 05 May 1954 06 May 2018 06 November 2019 1yr 6 months 06 May 1954 to 05 June 1954 06 July 2018 08 January 2020 1yr 6 months 06 June 1954 to 05 July 1954 06 September 2018 06 March 2020 1yr 6 months 06 July 1954 to 05 August 1954 06 November 2018 06 May 2020 1yr 6 months 06 August 1954 to 05 September 1954 06 January 2019 06 July 2020 1yr 6 months 06 September 1954 to 05 October 1954 06 March 2019 06 September 2020 1yr 6 months 06 October 1954 to 05 November 1954 06 May 2019 66th birthday at least 1 yr 5 months 06 -

GATT Bibliography, 1947-1953
FIRST EDITION GATT BIBLIOGRAPHY- 1947 - 1953 The text of the GATT Selected GATT publications A chronological list of references to the GATT GATT Secretariat Palais des Nations Geneva Switzerland March 1954 MGT/7/54 GATT BIBLIOGRAPHY This bibliography is a list of books, pamphlets, articles in periodicals, newspaper reports and editorials, and miscellaneous items including texts of lectures, which refer to the General Agreement on Tariffs and Trade. It covers a period of approximately seven years. For six of these years - from the beginning of 1948 - the GATT has been in operation. The purpose of the list is a practical one: to provide sources of reference for historians, researchers and students. The list, it must be emphasized, is limited to the formation and operation of the GATT; for masons *f length, the history of the Havana Charter and its preparation and references to the proposed International Trade Organization,'which has not been brought into being, have been somewhat rigidly excluded, while emphasis has been put on references that show the operational aspects of the GATT. The bibliography is divided into the following sections: 1. • the text' of the GATT and governmental publications; 2. selected GATT publications; (the full list of GATT publications is .obtainable from the secretariat on request) 3. a chronological listing of references to the GATT. This has been subdivided into the following periods, the references being listed alphabetically in each period: 1947 including the Geneva tariff negotiations (April- August), and the completion of the GATT 1948 including the first two sessions of the GATT (March at Havana, and August-September at Geneva) 1949 ,... -

UWOMJ Volume 23, Number 1, January 1953 Western University
Western University Scholarship@Western University of Western Ontario Medical Journal Digitized Special Collections 1-1953 UWOMJ Volume 23, Number 1, January 1953 Western University Follow this and additional works at: https://ir.lib.uwo.ca/uwomj Part of the Medicine and Health Sciences Commons Recommended Citation Western University, "UWOMJ Volume 23, Number 1, January 1953" (1953). University of Western Ontario Medical Journal. 140. https://ir.lib.uwo.ca/uwomj/140 This Book is brought to you for free and open access by the Digitized Special Collections at Scholarship@Western. It has been accepted for inclusion in University of Western Ontario Medical Journal by an authorized administrator of Scholarship@Western. For more information, please contact [email protected], [email protected]. University of Western Ontario , MEDICAL JOURNAL Pt~blish•J Q~~Mtn/1 b1 The Hippocratic Society of the .. University of Western Ontario Medical School Authorized a.s Second Oa.ss Mail by the Post Office Departmeot at Ottawa 'U o~ . J.. ?J - rq6"?J STAFF Editors-in-Chief: J. D . PRouD, B.A., '53 J. E. TwELVES, B.A., '53 Editor: E. ]. PRoKIPCHUK1 '54 Assi.rtant Editor: ]. MoRRISON, B.A., '55 Managing Editor: L. J. LoEB, B.Sc., M.Sc., '54 Circulation and Subscription Managers: R. BENNETf, '54 A. BURNETI, B.A., '54 K. McKNIGHT, B.A., '55 Exchange Editor: MARION DENNIS, B.A., '53 Book Review Editor: BARBARA GARWOOD, '56 Abstract Editor: FAYE AltUNDBLL, '55 Alumni Correspondent: E. GusPIN, B.A., '55 Consulting Editors: R. G. E. MURRAY, M.D.C.M., M.A. E. M. WATSON, M.D., M.Sc., F.R.C.P., F.R.C.P. -

Business Conditions: January 1956
A review by the Federal Reserve Bank of Chicago Business Conditions 1956 January Contents The economic consequences of the baby boom 4 The price picture, pressures building up? 8 What they’re saying — about farm prospects, 1956 12 The Trend of Business 2-4 Digitized for FRASER http://fraser.stlouisfed.org/ Federal Reserve Bank of St. Louis the Trend OF BUSINESS R ising business activity during 1955 re having unemployment at less than 1.5 per cent. quired steady additions to the nation’s work Interestingly, the only two cities in the force. During the fourth quarter an average District considered to have a substantial labor of about 51 million persons were on business surplus are South Bend and Terre Haute. These payrolls—almost 1.8 million more than a year cities are located in the same state as Indian earlier and a new record. As a result, in many apolis, Fort Wayne and the Gary-Hammond areas pockets of unemployment continued to portion of the Chicago metropolitan area, all melt through the year. of which report very tight labor markets. This Early in 1956 a seasonal reversal in the situation reflects the tendency for jobs and employment upswing is inevitable. Just as workers to get out of balance in local areas and December almost invariably records the em the reluctance of workers to seek work at a ployment high for the year, as hirings rise to distance from their homes and former jobs. accommodate Christmas business, so do Jan In November some types of manufacturers uary and February mark low points. -
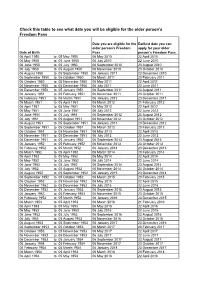
Copy of Age Eligibility from 6 April 10
Check this table to see what date you will be eligible for the older person's Freedom Pass Date you are eligible for the Earliest date you can older person's Freedom apply for your older Date of Birth Pass person's Freedom Pass 06 April 1950 to 05 May 1950 06 May 2010 22 April 2010 06 May 1950 to 05 June 1950 06 July 2010 22 June 2010 06 June 1950 to 05 July 1950 06 September 2010 23 August 2010 06 July 1950 to 05 August 1950 06 November 2010 23 October 2010 06 August 1950 to 05 September 1950 06 January 2011 23 December 2010 06 September 1950 to 05 October 1950 06 March 2011 20 February 2011 06 October 1950 to 05 November 1950 06 May 2011 22 April 2011 06 November 1950 to 05 December 1950 06 July 2011 22 June 2011 06 December 1950 to 05 January 1951 06 September 2011 23 August 2011 06 January 1951 to 05 February 1951 06 November 2011 23 October 2011 06 February 1951 to 05 March 1951 06 January 2012 23 December 2011 06 March 1951 to 05 April 1951 06 March 2012 21 February 2012 06 April 1951 to 05 May 1951 06 May 2012 22 April 2012 06 May 1951 to 05 June 1951 06 July 2012 22 June 2012 06 June 1951 to 05 July 1951 06 September 2012 23 August 2012 06 July 1951 to 05 August 1951 06 November 2012 23 October 2012 06 August 1951 to 05 September 1951 06 January 2013 23 December 2012 06 September 1951 to 05 October 1951 06 March 2013 20 February 2013 06 October 1951 to 05 November 1951 06 May 2013 22 April 2013 06 November 1951 to 05 December 1951 06 July 2013 22 June 2013 06 December 1951 to 05 January 1952 06 September 2013 23 August 2013 06 -

GENERAL AGREEMENT on • ^ TARIFFS and TRADE 3 February 1953 Limited Distribution
T5TP PJTTÎT C TRD GENERAL AGREEMENT ON • ^ TARIFFS AND TRADE 3 February 1953 Limited Distribution REPORT ON THE FINANCIAL SITUATION AS AT 31 JANUARY 1953 The statements attached give information on the actual inoome and expenditure for the financial year 1952, on the outstanding contributions as at 31 January 1953 and on current contributions reoeived before 31 January. A table showing the actual expenditure of ICITO/GATT from 1948 onwards is also attached. Report on the Financial Situation as at 31 January 1953 (in U^S. dollars) CD ro Preliminary actual income and expenditure of the financial year 1952 Total Incoes 0 398,114,78 Tctal Expenditure " 262.045.23 Disposable Surplus transferred to Reserve g 136.069.55 Outstanding ocntribut:ons for previous years - g 28.596.33 a) Contracting Parties: Tîtal cf contributions Country 1948-49 1950 1951 1952 outstanding China 3,750,- 10,601.72 14,351.72 Peru 2,687.25 2,669.25 5,356.50 Syria 2.653.43 2.687.25 5.337.68 Tctal 3.750.- 13.252.15 5.374.50 2.669.25 25.545.90 b) Acceding Governments: Total of contributions Country 1948-49 1950 1951 1952 outstanding Uruguay 900.- 2.650.43 3.550.43 T^tal 900.- 2.650.43 3.550.43 Statement of contributions received and contributions outstanding as at 31 January 1953 a) 1953 contributions received as at 31 January 1053' 0 71,788,33 = 21,.45% b) 1953 contributions of Contracting Parties outstanding as at 31 January 1953 0 270,211.67 = 76.98% c) contributions becoming due ca. -

Country Term # of Terms Total Years on the Council Presidencies # Of
Country Term # of Total Presidencies # of terms years on Presidencies the Council Elected Members Algeria 3 6 4 2004 - 2005 December 2004 1 1988 - 1989 May 1988, August 1989 2 1968 - 1969 July 1968 1 Angola 2 4 2 2015 – 2016 March 2016 1 2003 - 2004 November 2003 1 Argentina 9 18 15 2013 - 2014 August 2013, October 2014 2 2005 - 2006 January 2005, March 2006 2 1999 - 2000 February 2000 1 1994 - 1995 January 1995 1 1987 - 1988 March 1987, June 1988 2 1971 - 1972 March 1971, July 1972 2 1966 - 1967 January 1967 1 1959 - 1960 May 1959, April 1960 2 1948 - 1949 November 1948, November 1949 2 Australia 5 10 10 2013 - 2014 September 2013, November 2014 2 1985 - 1986 November 1985 1 1973 - 1974 October 1973, December 1974 2 1956 - 1957 June 1956, June 1957 2 1946 - 1947 February 1946, January 1947, December 1947 3 Austria 3 6 4 2009 - 2010 November 2009 1 1991 - 1992 March 1991, May 1992 2 1973 - 1974 November 1973 1 Azerbaijan 1 2 2 2012 - 2013 May 2012, October 2013 2 Bahrain 1 2 1 1998 - 1999 December 1998 1 Bangladesh 2 4 3 2000 - 2001 March 2000, June 2001 2 Country Term # of Total Presidencies # of terms years on Presidencies the Council 1979 - 1980 October 1979 1 Belarus1 1 2 1 1974 - 1975 January 1975 1 Belgium 5 10 11 2007 - 2008 June 2007, August 2008 2 1991 - 1992 April 1991, June 1992 2 1971 - 1972 April 1971, August 1972 2 1955 - 1956 July 1955, July 1956 2 1947 - 1948 February 1947, January 1948, December 1948 3 Benin 2 4 3 2004 - 2005 February 2005 1 1976 - 1977 March 1976, May 1977 2 Bolivia 3 6 7 2017 - 2018 June 2017, October -

JACKSON, CD: Records
DWIGHT D. EISENHOWER LIBRARY ABILENE, KANSAS JACKSON, C.D.: Records, 1953-54 Pre-Accession Processed by: KR, BM Date Complete: October 22, 1980 Linear feet of shelf space occupied: 3 Approximate number of pages: 6000 Approximate number of items: 3400 Literary rights in these records are in the public domain. These records were reviewed under provisions of the instrument of gift of Dwight D. Eisenhower signed April 13, 1960. Under terms of the instrument of gift the following classes of documents are withheld from research use: 1. Papers that are security-classified until such classification shall be removed. 2. Papers the use of which may be prejudicial to the maintenance of good relations with foreign nations. 3. Papers containing statements made in confidence unless the reason for confidentiality no longer exists. 4. Papers relating to family or private business affairs. 5. Papers containing statements which might be used to injure, harass, or damage any living person. SCOPE AND CONTENT NOTE The records of C.D. (Charles Douglas) Jackson were generated, with a very few exceptions, during his tenure as Special Assistant to the President, February 16, 1953 to March 31, 1954. His area responsibility was loosely defined as international affairs, cold war planning, and psychological warfare. His main function was the coordination of activities aimed at interpreting world situations to the best advantage of the United States and her allies and exploiting incidents which reflected negatively on the Soviet Union, Communist China and other enemies in the Cold War. Jackson’s background in psychological warfare during World War II (see finding aid to the C.D. -

Inventory Dep.288 BBC Scottish
Inventory Dep.288 BBC Scottish National Library of Scotland Manuscripts Division George IV Bridge Edinburgh EH1 1EW Tel: 0131-466 2812 Fax: 0131-466 2811 E-mail: [email protected] © Trustees of the National Library of Scotland Typescript records of programmes, 1935-54, broadcast by the BBC Scottish Region (later Scottish Home Service). 1. February-March, 1935. 2. May-August, 1935. 3. September-December, 1935. 4. January-April, 1936. 5. May-August, 1936. 6. September-December, 1936. 7. January-February, 1937. 8. March-April, 1937. 9. May-June, 1937. 10. July-August, 1937. 11. September-October, 1937. 12. November-December, 1937. 13. January-February, 1938. 14. March-April, 1938. 15. May-June, 1938. 16. July-August, 1938. 17. September-October, 1938. 18. November-December, 1938. 19. January, 1939. 20. February, 1939. 21. March, 1939. 22. April, 1939. 23. May, 1939. 24. June, 1939. 25. July, 1939. 26. August, 1939. 27. January, 1940. 28. February, 1940. 29. March, 1940. 30. April, 1940. 31. May, 1940. 32. June, 1940. 33. July, 1940. 34. August, 1940. 35. September, 1940. 36. October, 1940. 37. November, 1940. 38. December, 1940. 39. January, 1941. 40. February, 1941. 41. March, 1941. 42. April, 1941. 43. May, 1941. 44. June, 1941. 45. July, 1941. 46. August, 1941. 47. September, 1941. 48. October, 1941. 49. November, 1941. 50. December, 1941. 51. January, 1942. 52. February, 1942. 53. March, 1942. 54. April, 1942. 55. May, 1942. 56. June, 1942. 57. July, 1942. 58. August, 1942. 59. September, 1942. 60. October, 1942. 61. November, 1942. 62. December, 1942. 63. January, 1943. -

Communique, November 1954
University of Montana ScholarWorks at University of Montana Communique, 1953-2020 Journalism 11-1954 Communique, November 1954 Montana State University (Missoula, Mont.). School of Journalism Follow this and additional works at: https://scholarworks.umt.edu/communique Let us know how access to this document benefits ou.y Recommended Citation Montana State University (Missoula, Mont.). School of Journalism, "Communique, November 1954" (1954). Communique, 1953-2020. 47. https://scholarworks.umt.edu/communique/47 This Newsletter is brought to you for free and open access by the Journalism at ScholarWorks at University of Montana. It has been accepted for inclusion in Communique, 1953-2020 by an authorized administrator of ScholarWorks at University of Montana. For more information, please contact [email protected]. ARCHIVES Bue Is Acting J-School Dean; NY Times Reprints Scanlan Gets MSPA Post; Reinemer Article Dorothy Johnson Joins Staff “A Southern '...City Debates Prof. O. J. Bue has been ap In addition to the regular staff Nonsegregation,’’ a short article Secretary of Army Speaks pointed acting dean of the MSU members, Ray Wight and Ed Du by Vic Reinemer, appeared in School of Journalism, replacing gan, Miss Dorothy Johnson, secre the September 26 issue of the The election of Robert J. Scan of MSPA. Other officers included' Dr. James L. C. Ford. Dr. Ford tary of the State Press associa New York Times magazine sec lan, Miles City Daily Star, as R. E. Morrison, Missoulian-Sen- continues as a professor of journ tion, is teaching a magazine tion. president of Montana State Press tinel, second vice-president; Mel alism.