ASMMR Newsletter Vol 3 Issue 3
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Vysoké Učení Technické V Brně Automobilové Soutěže
VYSOKÉ UČENÍ TECHNICKÉ V BRNĚ BRNO UNIVERSITY OF TECHNOLOGY FAKULTA STROJNÍHO INŽENÝRSTVÍ ÚSTAV AUTOMOBILNÍHO A DOPRAVNÍHO INŽENÝRSTVÍ FACULTY OF MECHANICAL ENGINEERING INSTITUTE OF AUTOMOTIVE ENGINEERING AUTOMOBILOVÉ SOUTĚŽE A POUŽÍVANÁ TECHNIKA VČETNĚ SERIÁLU WRC RALLYE CHAMPIONSCHIPS AND USED ENGINEERING INCLUDING WRC SERIES BAKALÁŘSKÁ PRÁCE BACHELOR´S THESIS AUTOR PRÁCE PAVEL NOVÁK AUTHOR VEDOUCÍ PRÁCE ING. PAVEL RAMÍK SUPERVISOR BRNO 2010 ABSTRAKT Obsahem bakalářské práce je přehled současného stavu techniky používané v automobilových soutěžích se zaměřením na seriál WRC. Práce je rozdělena do pěti částí. V první části jsou uvedeny soudobé automobilové soutěže a federace FIA. Druhá část je zaměřená na specifikaci vozů WRC. Třetí část seznamuje se způsobem organizace šampionátu WRC. Jsou představeny posádky se svými týmy, jejich výsledky v šampionátu a v poháru konstruktérů. Největší pozornost je věnována čtvrté a páté části, které jsou zaměřeny na soudobou techniku používanou ve WRC a vývojové trendy v této oblasti. Jsou zde uvedeny způsoby virtuálního navrhování, počítačové simulace a testování.V závěru práce jsou zmíněny příklady vývoje vozů WRC a řešení převzaté na sériové vozy z techniky WRC. Klíčová slova: Rallye, FIA, WRC, karoserie, podvozek, tlumič, motor, převodovka, diferenciál, brzda, pneumatika, testování, rekuperace ABSTRACT The content of the bachelor thesis is an overview of the current condition of technics used in the car racing competitions focused on the WRC serial. The thesis is diveded into five parts. The first part introduces the contemporary car competitions and FIA federation. The second part is focused on specification of the WRC cars. The third part familiarizes with the organization process of the WRC championship. There are introduced crews with their teams and their results in the constructor cup. -

PRESS RELEASE FIM Grand Prix World Championship
PRESS RELEASE MIES, 29/05/2020 FOR MORE INFORMATION: ISABELLE LARIVIÈRE COMMUNICATIONS MANAGER [email protected] TEL +41 22 950 95 68 FIM Grand Prix World Championship 2020 Calendar, UPDATE 29 MAY British and Australian Grands Prix cancelled The FIM, IRTA and Dorna Sports regret to announce the cancellation of the British and Australian Grands Prix. The ongoing coronavirus outbreak and resulting calendar changes have obliged the cancellation of both events. The British Grand Prix was set to take place from 28 to 30 August at the classic Silverstone Circuit. Silverstone hosted the first Grands Prix held on the British mainland from 1977, and MotoGP™ returned to the illustrious track ten years ago. 2020 will now sadly mark the first year MotoGP™ sees no track action in the British Isles for the first time in the Championship’s more than 70-year history. The Australian Motorcycle Grand Prix was set to take place at the legendary Phillip Island Grand Prix Circuit from 23 to 25 October. Phillip Island hosted the very first Australian Motorcycle Grand Prix in 1989 and since 1997 has been the only home of MotoGP™ Down Under - with its unique layout providing some of the greatest battles ever witnessed on two wheels. The cancellation of the British Grand Prix also obliges the cancellation of the corresponding British Talent Cup track activity at the same event. Stuart Pringle, Silverstone Managing Director: “We are extremely disappointed about the cancellation of the British MotoGP event, not least as the cancelled race in 2018 is still such a recent memory, but we support the decision that has had to be taken at this exceptional time. -
Aussie Racing Cars Entry List
V8 Supercars Coates Hire Sydney 500 I Welcome/Contents 3 COATES HIRE SYDNEY 500 Contents DECEMBER 4 - 6, 2015 IN EVERY ISSUE! EDITOR IN CHIEF: Gordon Lomas 3 WELCOME/CONTENTS 28 CARUSO/MOFFAT 7 CIRCUIT GUIDE 29 BRIGHT/COULTHARD JOURNALIST: 9 V8 SUPERCARS ENTRY LIST 30 WOOD/MCLAUGHLIN Tom Howard 10 PREVIOUS WINNERS 31 WALL/PYE 13 TV TIMES 32 GISBERGEN DESIGN: 14 2015 V8 SUPERCARS CALENDAR 34 V8 SUPERCAR CHAMPIONS Kirstie Fuentes 15 WHINCUP/LOWNDES 38 DUNLOP SERIES ENTRY LIST 16 TANDER/COURTNEY 39 F4 ENTRY LIST SALES/MARKETING: 18 SLADE/HOLDSWORTH 40 V8 UTES ENTRY LIST Leisa Emberson 20 BLANCHARD/PERCAT 43 STADIUM SUPER TRUCKS 22 WALSH/W.DAVISON ENTRY LIST PARTNERS: 23 WINTERBOTTOM/WATERS 44 AUSSIE RACING CARS ENTRY LIST SUBSCRIBE AND NEVER Armor All 25 REYNOLDS/HEIMGARTNER 45 SCHEDULE OF EVENTS MISS A COPY! Castrol Edge 27 T.KELLY/R.KELLY Pirtek Coates Hire Crimsafe Dunlop Tata Motors Apex Jobstop GearWrench STATS DID YOU KNOW SUpercheap Auto CHAMPIONSHIP Craig Lowndes will start his 250th round this weekend, equalling Russell Ingall for STANDINGS the most starts in Australian Touring Car/V8 36 4 Supercars Championship history... Frosty’s career defining moment fter 33 races spanning the length and breadth circuit’s punishing nature and often changeable weather of Australia, the scene is now set to crown a conditions. new V8 Supercars champion. As a result, Lowndes has a slim since of pulling off one of A Two protagonists remain following an the most impressive title fightback having been 423 points eventful Phillip Island Super Sprint which has adrift following Sandown. -

PRESS RELEASE FIM Grand Prix World Championship
PRESS RELEASE MIES, 19/08/2021 FOR MORE INFORMATION: ISABELLE LARIVIÈRE COMMUNICATIONS MANAGER [email protected] TEL +41 22 950 95 68 FIM Grand Prix World Championship 2021 calendar, UPDATE 19 August Malaysian GP cancelled and replaced by a Grand Prix at Misano World Circuit Marco Simoncelli The FIM, IRTA and Dorna Sports regret to announce the cancellation of the Malaysia Motorcycle Grand Prix, which was set to take place at Sepang International Circuit from the 22nd to the 24th of October. The ongoing Covid-19 pandemic and the resulting entry restrictions for Malaysia oblige the cancellation of the event. The FIM MotoGP™ World Championship looks forward to returning to Sepang in 2022 to race in front of our dedicated Malaysian fans. The FIM, IRTA and Dorna Sports are pleased to confirm that MotoGP™ will return to Misano World Circuit Marco Simoncelli from the 22nd to the 24th of October, the weekend previously scheduled for the Malaysian GP, for a second Grand Prix at the classic Italian track. The name of this event will be announced in due course. The date for the Gran Premio Octo di San Marino e della Riviera di Rimini remains unchanged. 11 ROUTE DE SUISSE TEL +41 22 950 95 00 CH – 1295 MIES FAX +41 22 950 95 01 [email protected] FOUNDED 1904 WWW.FIM-MOTO.COM Revised calendar Date Grand Prix Venue 28 March Qatar* Losail International Circuit 04 April Qatar* Losail International Circuit 18 April Portugal Algarve International Circuit 02 May Spain Circuito de Jerez 16 May France Le Mans 30 May Italy Autodromo del Mugello 06 June -

Stewards Summary of Judicial Outcomes
STEWARDS SUMMARY OF JUDICIAL OUTCOMES Event Document: 45 2020 INTERNATIONAL VIRGIN AUSTRALIA SUPERCARS CHAMPIONSHIP RACES 16, 17 & 18 “CORESTAFF DARWIN SUPERSPRINT” Hidden Valley Raceway, Darwin, Northern Territory 21st to 23rd August 2020 STEWARDS SUMMARY OF JUDICIAL OUTCOMES, Update Final: Issued Sunday 23rd August 2020 at 1730hrs. Sunday 23rd August 2020 Matters from Race 18: Race Director Incident Determinations During the Race the RD conducted an investigation at the request of Triple Eight Race Engineering into an Incident at Turn 4 on Lap 35 when Car #18, Mark Winterbottom, overtook Car #97, Shane van Gisbergen, and contact occurred between the two Cars. After reviewing broadcast footage of the Incident and consulting the DSA, the RD determined that there was no evidence of a breach of the Rules by the Driver of Car #18. Stewards’ Decisions – Penalties imposed The Stewards imposed a 5 second Time Penalty on Car #12, Fabian Coulthard, for a breach of Article 2.1.1 of Schedule B2 (Careless Driving) following contact between Car #12 and Car #2, Bryce Fullwood, at Turn 14 on Lap 15 as a result of which Car #2 was pushed wide and Car #12 gained a position. Matters from Race 17: Race Director Incident Determinations There were no determinations. Stewards’ Decisions – Penalties imposed The Stewards issued the following Penalties during the Race in each case for a breach of Article 2.1.1 of Shcedule B2 (Careless Driving): - A 5 second Time Penalty on Car #55, Jack le Broq, arising out of an Incident at Turn 6 on Lap 23 when Car #55 locked brakes attempting to overtake Car #15, Rick Kelly, causing contact with Car #15 as a result of which Car #55 gained a position; - A 15 second Time Penalty on Car #25, Chaz Mostert, arising out of an Incident at Turn 1 on Lap 34 when Car #25 made contact with Car #8, Nick Percat, as a result of which Car #8 spun and lost positions; - A 15 second Time Penalty on Car #35, Garry Jacobson, arising out of an Incident at Turn 1 on Lap 37 when Car #35 made contact with Car #3, Macauley Jones, which caused Car #3 to spin. -
R Race CLASSIFICATION
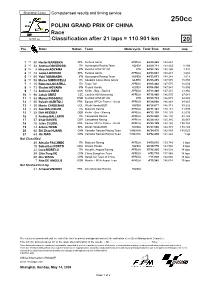
Shanghai Circuit Computerised results and timing service 250cc POLINI GRAND PRIX OF CHINA Race 5281 m. Classification after 21 laps = 110.901 km 20 Pos Rider Nation Team Motorcycle Total Time Km/h Gap 1 25 80 Hector BARBERA SPA Fortuna Aprilia APRILIA 44'49.445 148.448 2 20 34 Andrea DOVIZIOSO ITA Humangest Racing Team HONDA 44'49.711 148.433 0.266 3 16 4 Hiroshi AOYAMA JPN Red Bull KTM GP 250 KTM 44'52.765 148.265 3.320 4 13 48 Jorge LORENZO SPA Fortuna Aprilia APRILIA 44'53.047 148.249 3.602 5 11 55 Yuki TAKAHASHI JPN Humangest Racing Team HONDA 44'53.063 148.248 3.618 6 10 58 Marco SIMONCELLI ITA Squadra Corse Metis Gilera GILERA 45'05.295 147.578 15.850 7 9 15 Roberto LOCATELLI ITA Team Toth APRILIA 45'05.448 147.570 16.003 8 8 73 Shuhei AOYAMA JPN Repsol Honda HONDA 45'06.000 147.540 16.555 9 7 14 Anthony WEST AUS Kiefer - Bos - Racing APRILIA 45'11.305 147.251 21.860 10 6 96 Jakub SMRZ CZE Cardion AB Motoracing APRILIA 45'16.486 146.970 27.041 11 5 54 Manuel POGGIALI RSM Red Bull KTM GP 250 KTM 45'23.734 146.579 34.289 12 4 50 Sylvain GUINTOLI FRA Equipe GP De France - Scrab APRILIA 45'24.008 146.564 34.563 13 3 36 Martin CARDENAS COL Wurth Honda BQR HONDA 45'28.677 146.313 39.232 14 2 25 Alex BALDOLINI ITA Matteoni Racing APRILIA 45'31.141 146.181 41.696 15 1 28 Dirk HEIDOLF GER Kiefer - Bos - Racing APRILIA 45'32.138 146.128 42.693 16 8 Andrea BALLERINI ITA Campetella Racing APRILIA 45'32.593 146.104 43.148 17 57 Chaz DAVIES GBR Campetella Racing APRILIA 45'46.112 145.385 56.667 18 16 Jules CLUZEL FRA Equipe GP De France - Scrab -

Rally of Great Britain Day Results
RMS 16/09/12 16:44 FIA WORLD RALLY CHAMPIONSHIP RALLY OF GREAT BRITAIN ROUND: 10 OF 13 (13 - 16 SEPTEMBER) ITINERARY ENTRIES START LISTS QUALIFYING STAGE TIMES PENALTIES RETIREMENTS DAY RESULTS DAY RESULTS FINAL CLASSIFICATION Diff Driver Stage Total Pos No Nat Vehicle Class Penalties Fastest Eligibility Co-Driver Time Time (Prev) Jari-Matti LATVALA FIN **:**.* 1 3 FORD FIESTA RS WRC WRC 3:03:40.3 3:03:40.3 C, M Miikka ANTTILA FIN **:**.* Sebastien LOEB FRA +27.8 2 1 CITROEN DS3 WRC WRC 3:04:08.1 3:04:08.1 C, M Daniel ELENA FRA +27.8 Petter SOLBERG NOR +28.7 3 4 FORD FIESTA RS WRC WRC 3:04:09.0 3:04:09.0 C, M Chris PATTERSON GBR +0.9 Mads OSTBERG NOR +1:10.6 4 10 FORD FIESTA RS WRC WRC 3:04:50.9 3:04:50.9 C, M Jonas ANDERSSON SWE +41.9 Mikko HIRVONEN FIN +1:29.5 5 2 CITROEN DS3 WRC WRC 3:05:09.8 3:05:09.8 C, M Jarmo LEHTINEN FIN +18.9 Evgeny NOVIKOV RUS +3:37.0 6 6 FORD FIESTA RS WRC WRC 3:07:17.3 3:07:17.3 C, M Ilka MINOR AUT +2:07.5 Thierry NEUVILLE BEL +4:11.9 7 8 CITROEN DS3 WRC WRC 3:07:52.2 3:07:52.2 C, M Nicolas GILSOUL BEL +34.9 Matthew WILSON GBR +6:00.4 8 15 FORD FIESTA RS WRC WRC 3:09:40.7 3:09:40.7 C Scott MARTIN GBR +1:48.5 Martin PROKOP CZE +6:58.9 9 21 FORD FIESTA RS WRC WRC 3:10:39.2 3:10:39.2 C Zdenek HRUZA CZE +58.5 Nasser AL-ATTIYAH QAT +9:32.1 10 7 CITROEN DS3 WRC WRC 3:13:12.4 3:13:12.4 C, M Giovanni BERNACCHINI ITA +2:33.2 Chris ATKINSON AUS +9:37.0 11 12 MINI JOHN COOPER WORKS WRC WRC 3:13:17.3 3:13:17.3 C, M Stephane PREVOT BEL +4.9 Sebastien OGIER FRA +9:44.0 12 22 SKODA FABIA S2000 2 3:13:24.3 3:13:24.3 C Julien -

50 Ans De Volkswagen Motorsport 13 Septembre 2016 V16/29F
• presse • news • prensa • tisk • imprensa • prasa • stampa • pers • 50 ans de Volkswagen Motorsport 13 septembre 2016 V16/29F Une exposition spéciale interactive célébrant les 50 ans de Volkswagen Motorsport a officiellement ouvert ses portes à Berlin au DRIVE. Volkswagen Group Forum, au croisement des rues Friedrichstrasse 84 / Unter den Linden. L’accent est mis sur la présentation de véhicules uniques dont la Golf à double moteur conçue pour l’iconique course de côte du Pikes Peak, le Race Touareg 3 que Gottschalk et Nasser Al-Attiyah (Q) ont mené à la victoire au Dakar 2011 et l’actuelle Polo R WRC victorieuse en Championnat du Monde des Rallyes. Cette exposition interactive se déroulera jusqu’au 30 octobre. Pour plus d’informations, visitez le site: http://www.drive-volkswagen-group.com/en/. Ci-après, vous trouverez le dossier complet sur les 50 ans de Volkswagen Motorsport en anglais. s.a. D’Ieteren n.v. Press relations Contact Maliestraat 50, Rue du Mail T. : 02/536.50.72 1050 Brussel/Bruxelles [email protected] BTW/TVA BE0403.448.140 www.volkswagen-press.be RPR Brussel / RPM Bruxelles Motorsport Information Information Package 50 Years of Volkswagen Motorsport Contents 02 Contents Gallery 03 Introduction 08 Time Bar Interview Jost Capito 13 Background Formula Vee and 21 Formula 3 Background One-Make Cup 28 Background 33 Endurance Races Background Dakar Rally 39 Background 45 WRC Background Rallycross 51 History 57 Facts and Figures Volkswagen Motorsport For Media 60 Gallery 03 Formula Vee “Born in the USA” – and -

CCNT V8 Supercars Luncheon 2018 (NT News Courtesy: Phil Timney Hon
The Carbiner “For sport and for good fellowship” THE OFFICIAL NEWSLETTER OF THE CARBINE CLUB EDITION 8 of 2018 – 29 June, 2018 Launch of the Carbine Club of Tokyo! NT- V8 Supercars Luncheon Carbiners in the News Vale Gary Balkin, CCQLD FOR THE DIARY-COMING EVENTS The Carbiner is also available on the Club website at www.thecarbineclub.org All contributions to The Carbiner welcomed – place your event & news on the record! Contact Merv Hill at [email protected] THE CARBINE CLUB of TOKYO – Inaugural Luncheon Exciting news with the addition of another Club to the ranks – the Carbine Club of Tokyo will hold its first luncheon on 13 July. We look forward to news from the latest addition to Club ranks! 1 | P a g e CARBINER 8- 2018 CCNT V8 Supercars Luncheon 2018 (NT news courtesy: Phil Timney Hon. Sec. CCNT) This major luncheon on the Carbine Club of NT calendar broke with tradition in 2018 with the function being held at the newly renovated Pee Wee’s at the Point Restaurant overlooking the Darwin Harbour. In excess of 200 members and guests attended the luncheon for an afternoon of high octane entertainment to coincide with the Crownbet Darwin Triple Crown round of the V8 Supercars Championship held at Hidden Valley racetrack. CC NT Committee with the Crownbet V8 Grid Girls Our resident MC and Life Member Andy Bruyn took no time in warming up the gathering with his unique and colourful repertoire before introducing our guests of honour, V8 Supercar drivers Dave Reynolds from the Holden Erebus Motorsport team, Lee Holdsworth, Holden Charlie Schwerkolt Racing and Todd Hazelwood from the Ford Matt Stone Racing team. -

Wales Rally GB 14/11/2017, 14�24
Wales Rally GB 14/11/2017, 14)24 WALES RALLY GB FIA World Rally Championship 2017 Combined classification After Stage SS21 Brenig 2 (Power Stage) Stage Overall Pos Nr Entry Pri. Time Diff 1st Diff Prev Pos Nr Entry Class Pri. Pen. Time Diff 1st Diff Prev 1 5 Thierry NEUVILLE 1 4:01.2 1 3 Elfyn EVANS RC1 1 2:57:00.6 2 9 Kris MEEKE 1 4:02.7 +1.5 +1.5 2 5 Thierry NEUVILLE RC1 1 0:10 2:57:37.9 +37.3 +37.3 3 10 Jari-Matti LATVALA 1 4:02.8 +1.6 +0.1 3 1 Sébastien OGIER RC1 1 2:57:45.8 +45.2 +7.9 4 1 Sébastien OGIER 1 4:03.1 +1.9 +0.3 4 6 Andreas MIKKELSEN RC1 1 2:57:50.4 +49.8 +4.6 5 6 Andreas MIKKELSEN 1 4:03.2 +2.0 +0.1 5 10 Jari-Matti LATVALA RC1 1 2:57:50.9 +50.3 +0.5 6 8 Craig BREEN 1 4:03.2 +2.0 +0.0 6 2 Ott TÄNAK RC1 1 2:58:02.9 +1:02.3 +12.0 7 12 Esapekka LAPPI 1 4:05.7 +4.5 +2.5 7 9 Kris MEEKE RC1 1 2:58:21.1 +1:20.5 +18.2 8 3 Elfyn EVANS 1 4:07.0 +5.8 +1.3 8 4 Hayden PADDON RC1 1 2:59:16.9 +2:16.3 +55.8 9 16 Dani SORDO 1 4:07.5 +6.3 +0.5 9 12 Esapekka LAPPI RC1 1 2:59:47.1 +2:46.5 +30.2 10 4 Hayden PADDON 1 4:07.6 +6.4 +0.1 10 16 Dani SORDO RC1 1 3:00:51.1 +3:50.5 +1:04.0 11 14 Mads OSTBERG 1 4:08.1 +6.9 +0.5 11 31 Pontus TIDEMAND RC2 2 3:07:12.2 +10:11.6 +6:21.1 12 2 Ott TÄNAK 1 4:12.7 +11.5 +4.6 12 32 Eric CAMILLI RC2 2 0:10 3:09:06.6 +12:06.0 +1:54.4 13 33 Ole Christian VEIBY 2 4:13.6 +12.4 +0.9 13 41 Tom CAVE RC2 2 3:09:15.5 +12:14.9 +8.9 14 34 Teemu SUNINEN 2 4:13.8 +12.6 +0.2 14 49 David BOGIE RC2 2 3:09:48.3 +12:47.7 +32.8 15 51 Kalle ROVANPERÄ 2 4:14.1 +12.9 +0.3 15 8 Craig BREEN RC1 1 3:09:59.3 +12:58.7 +11.0 16 81 Marius AASEN -
The Chequered Flag
THE CHEQUERED March 2016 Issue 1 FLAG F101 MR322G £100 MR191 £295 1985 British Lewis Hamilton Truck Grand signed Formula 1 Prix Silverstone photo, our choice programme. Signed inside by two-time Moto GP World Champion Barry Sheene who later turned to Truck Racing, plus tickets MR225 £295 Pedro Rodriguez De La Vega signed ticket MR273 £100 Patrick Head, Adrian Newey, and Ross Brawn signed 2010 Sixty Years of Formula One Silverstone cover, they were all engineers MR322F £150 1987 Truck Prix signed official MR238 £350 Brands Hatch Graham Hill signed 4 x 6 photo programme. mounted onto card Signed inside by Rod Chapman (7x European Truck Champ) Barry Sheene (2x Moto GP Champ) Davina Galica (F1), Barry Lee (4x Truck World Champ), plus tickets MR117A £175 01303 278137 Michael EMAIL: [email protected] Schumacher signed photo, our choice Buckingham Covers, Warren House, Shearway Road, Folkestone, Kent CT19 4BF 1 Tel 01303 278137 Fax 01303 279429 Email [email protected] SIGNED SILVERSTONE 2010 - 60 YEARS OF F1 Occassionally going round fairs you would find an odd Silverstone Motor Racing cover with a great signature on, but never more than one or two and always hard to find. They were only ever on sale at the circuit, and were sold to raise funds for things going on in Silverstone Village. Being sold on the circuit gave them access to some very hard to find signatures, as you can see from this initial selection. MR261 £30 MR262 £25 MR77C £45 Father and son drivers Sir Jackie Jody Scheckter, South African Damon Hill, British Racing Driver, and Paul Stewart. -

Video Name Track Track Location Date Year DVD # Classics #4001
Video Name Track Track Location Date Year DVD # Classics #4001 Watkins Glen Watkins Glen, NY D-0001 Victory Circle #4012, WG 1951 Watkins Glen Watkins Glen, NY D-0002 1959 Sports Car Grand Prix Weekend 1959 D-0003 A Gullwing at Twilight 1959 D-0004 At the IMRRC The Legacy of Briggs Cunningham Jr. 1959 D-0005 Legendary Bill Milliken talks about "Butterball" Nov 6,2004 1959 D-0006 50 Years of Formula 1 On-Board 1959 D-0007 WG: The Street Years Watkins Glen Watkins Glen, NY 1948 D-0008 25 Years at Speed: The Watkins Glen Story Watkins Glen Watkins Glen, NY 1972 D-0009 Saratoga Automobile Museum An Evening with Carroll Shelby D-0010 WG 50th Anniversary, Allard Reunion Watkins Glen, NY D-0011 Saturday Afternoon at IMRRC w/ Denise McCluggage Watkins Glen Watkins Glen October 1, 2005 2005 D-0012 Watkins Glen Grand Prix Festival Watkins Glen 2005 D-0013 1952 Watkins Glen Grand Prix Weekend Watkins Glen 1952 D-0014 1951-54 Watkins Glen Grand Prix Weekend Watkins Glen Watkins Glen 1951-54 D-0015 Watkins Glen Grand Prix Weekend 1952 Watkins Glen Watkins Glen 1952 D-0016 Ralph E. Miller Collection Watkins Glen Grand Prix 1949 Watkins Glen 1949 D-0017 Saturday Aternoon at the IMRRC, Lost Race Circuits Watkins Glen Watkins Glen 2006 D-0018 2005 The Legends Speeak Formula One past present & future 2005 D-0019 2005 Concours d'Elegance 2005 D-0020 2005 Watkins Glen Grand Prix Festival, Smalleys Garage 2005 D-0021 2005 US Vintange Grand Prix of Watkins Glen Q&A w/ Vic Elford 2005 D-0022 IMRRC proudly recognizes James Scaptura Watkins Glen 2005 D-0023 Saturday