Introduction to Spinal Anatomy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Anklyosed Spine: Fractures in DISH and Anklyosing Spondylitis
The Anklyosed Spine: Fractures in DISH and Anklyosing Spondylitis Lee F. Rogers, MD ACCR, Oct 26, 2012 Dallas, Texas Diffuse idiopathic skeletal hyperostosis (DISH) and ankylosing spondylitis (AS) are the most common diseases associated with spinal ankylosis. While they share the characteristic of ankylosis they are, in fact two separate diseases with distinct clinical, pathologic, and radiologic features. DISH: Diffuse idiopathic skeletal hyperostosis is a disease of older persons characterized by extensive ossification of the paraspinal ligaments anteriorly and laterally, bridging the intervening disc spaces. Bony bridging may be continuous or discontinuous. The anterior cortex of the vertebral body can be seen within the ossification. These findings are much more pronounced in the thoracic and lower cervical spine than in the lumbar area. Minor expressions of this disorder are commonly encountered in the mid-dorsal spine on lateral views of the chest. DISH characteristically spares the SI joints. The SI joints remain patent and clearly visible on radiographs or CT even in the presence of extensive disease in the thoracolumbar and cervical spine. DISH is also characterized by enthesopathy; ossification of ligaments or tendon insertions, forming so-called entheses. These appear as whiskering of the iliac crest, ischial tuberosites and greater trochanters. The radiographic appearance bears a superficial resemblance to that of AS. In DISH the spinal ossification is very irregular and unlike the thin, vertical syndesmophytes see in AS. The relative absence of changes in the lumbosacral spine, the patency of the SI joints, and absence of ankylosis of the facet and costovertebral joints should allow differentiation of DISH from AS. -

Mesenchymal Stem Cells in Combination with Hyaluronic Acid
www.nature.com/scientificreports OPEN Mesenchymal Stem Cells in Combination with Hyaluronic Acid for Articular Cartilage Defects Received: 1 August 2017 Lang Li1, Xin Duan1, Zhaoxin Fan2, Long Chen1,3, Fei Xing1, Zhao Xu4, Qiang Chen2,5 & Accepted: 19 April 2018 Zhou Xiang1 Published: xx xx xxxx Mesenchymal stem cells (MSCs) and hyaluronic acid (HA) have been found in previous studies to have great potential for medical use. This study aimed to investigate the therapeutic efects of bone marrow mesenchymal stem cells (BMSCs) combined with HA on articular cartilage repair in canines. Twenty-four healthy canines (48 knee-joints), male or female with weight ranging from 5 to 6 kg, were operated on to induce cartilage defect model and divided into 3 groups randomly which received diferent treatments: BMSCs plus HA (BMSCs-HA), HA alone, and saline. Twenty-eight weeks after treatment, all canines were sacrifced and analyzed by gross appearance, magnetic resonance imaging (MRI), hematoxylin-eosin (HE) staining, Masson staining, toluidine blue staining, type II collagen immunohistochemistry, gross grading scale and histological scores. MSCs plus HA regenerated more cartilage-like tissue than did HA alone or saline. According to the macroscopic evaluation and histological assessment score, treatment with MSCs plus HA also lead to signifcant improvement in cartilage defects compared to those in the other 2 treatment groups (P < 0.05). These fndings suggested that allogeneic BMSCs plus HA rather than HA alone was efective in promoting the formation of cartilage-like tissue for repairing cartilage defect in canines. Articular cartilage is composed of chondrocyte and extracellular matrix and has an important role in joint move- ment including lubrication, shock absorption and conduction. -

(AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: a Five-Year Follow-Up Prospective Cohort Study
life Communication Autologous Matrix Induced Chondrogenesis (AMIC) Compared to Microfractures for Chondral Defects of the Talar Shoulder: A Five-Year Follow-Up Prospective Cohort Study Filippo Migliorini 1 , Jörg Eschweiler 1, Nicola Maffulli 2,3,4,5,* , Hanno Schenker 1, Arne Driessen 1 , Björn Rath 1,6 and Markus Tingart 1 1 Department of Orthopedics and Trauma Surgery, University Clinic Aachen, RWTH Aachen University Clinic, 52064 Aachen, Germany; [email protected] (F.M.); [email protected] (J.E.); [email protected] (H.S.); [email protected] (A.D.); [email protected] (B.R.); [email protected] (M.T.) 2 School of Pharmacy and Bioengineering, Keele University School of Medicine, Staffordshire ST4 7QB, UK 3 Barts and the London School of Medicine and Dentistry, London E1 2AD, UK 4 Centre for Sports and Exercise Medicine, Queen Mary University of London, Mile End Hospital, London E1 4DG, UK 5 Department of Orthopedics, Klinikum Wels-Grieskirchen, A-4600 Wels, Austria 6 Department of Medicine, Surgery and Dentistry, University of Salerno, 84081 Baronissi, Italy * Correspondence: [email protected] Abstract: Introduction: Many procedures are available to manage cartilage defects of the talus, Citation: Migliorini, F.; Eschweiler, J.; including microfracturing (MFx) and Autologous Matrix Induced Chondrogenesis (AMIC). Whether Maffulli, N.; Schenker, H.; Driessen, AMIC or MFx are equivalent for borderline sized defects of the talar shoulder is unclear. Thus, the A.; Rath, B.; Tingart, M. Autologous present study compared the efficacy of primary isolated AMIC versus MFx for borderline sized Matrix Induced Chondrogenesis focal unipolar chondral defects of the talar shoulder at midterm follow-up. -

Paravertebral Block: Anatomy and Relevant Safety Issues Alberto E Ardon1, Justin Lee2, Carlo D
Paravertebral block: anatomy and relevant safety issues Alberto E Ardon1, Justin Lee2, Carlo D. Franco3, Kevin T. Riutort1, Roy A. Greengrass1 1Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Jacksonville, FL, 2Department of Anesthesiology, Olympia Anesthesia Associates, Providence St. Peter Hospital, Olympia, WA, 3Department of Anesthesiology and Pain Management, John H. Review Article Stroger Jr. Hospital of Cook County, Chicago, IL, USA Korean J Anesthesiol 2020;73(5):394-400 Paravertebral block, especially thoracic paravertebral block, is an effective regional anes- https://doi.org/10.4097/kja.20065 thetic technique that can provide significant analgesia for numerous surgical procedures, pISSN 2005–6419 • eISSN 2005–7563 including breast surgery, pulmonary surgery, and herniorrhaphy. The technique, although straightforward, is not devoid of potential adverse effects. Proper anatomic knowledge and adequate technique may help decrease the risk of these effects. In this brief discourse, we discuss the anatomy and technical aspects of paravertebral blocks and emphasize the im- Received: February 10, 2020 portance of appropriate needle manipulation in order to minimize the risk of complica- Revised: March 5, 2020 tions. We propose that, when using a landmark-based approach, limiting medial and later- Accepted: March 15, 2020 al needle orientation and implementing caudal (rather than cephalad) needle redirection may provide an extra margin of safety when performing this technique. Likewise, recog- Corresponding author: nizing a target that is not in close proximity to the neurovascular bundle when using ultra- Alberto E Ardon, M.D., M.P.H. sound guidance may be beneficial. Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, 4500 Keywords: Anatomy; Paravertebral; Postoperative pain; Regional anesthesia; Safety; Trun- San Pablo Rd, Jacksonville, FL 32224, USA cal nerve block. -

Ligaments of the Costovertebral Joints Including Biomechanics, Innervations, and Clinical Applications: a Comprehensive Review W
Open Access Review Article DOI: 10.7759/cureus.874 Ligaments of the Costovertebral Joints including Biomechanics, Innervations, and Clinical Applications: A Comprehensive Review with Application to Approaches to the Thoracic Spine Erfanul Saker 1 , Rachel A. Graham 2 , Renee Nicholas 3 , Anthony V. D’Antoni 2 , Marios Loukas 1 , Rod J. Oskouian 4 , R. Shane Tubbs 5 1. Department of Anatomical Sciences, St. George's University School of Medicine, Grenada, West Indies 2. Department of Anatomy, The Sophie Davis School of Biomedical Education 3. Department of Physical Therapy, Samford University 4. Neurosurgery, Complex Spine, Swedish Neuroscience Institute 5. Neurosurgery, Seattle Science Foundation Corresponding author: Erfanul Saker, [email protected] Abstract Few studies have examined the costovertebral joint and its ligaments in detail. Therefore, the following review was performed to better elucidate their anatomy, function and involvement in pathology. Standard search engines were used to find studies concerning the costovertebral joints and ligaments. These often- overlooked ligaments of the body serve important functions in maintaining appropriate alignment between the ribs and spine. With an increasing interest in minimally invasive approaches to the thoracic spine and an improved understanding of the function and innervation of these ligaments, surgeons and clinicians should have a good working knowledge of these structures. Categories: Neurosurgery, Orthopedics, Rheumatology Keywords: costovertebral joint, spine, anatomy, thoracic Introduction And Background The costovertebral joint ligaments are relatively unknown and frequently overlooked anatomical structures [1]. Although small and short in size, they are abundant, comprising 108 costovertebral ligaments in the normal human thoracic spine, and they are essential to its stability and function [2-3]. -

Synovial Joints Permit Movements of the Skeleton
8 Joints Lecture Presentation by Lori Garrett © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes 8.1 Contrast the major categories of joints, and explain the relationship between structure and function for each category. 8.2 Describe the basic structure of a synovial joint, and describe common accessory structures and their functions. 8.3 Describe how the anatomical and functional properties of synovial joints permit movements of the skeleton. © 2018 Pearson Education, Inc. Section 1: Joint Structure and Movement Learning Outcomes (continued) 8.4 Describe flexion/extension, abduction/ adduction, and circumduction movements of the skeleton. 8.5 Describe rotational and special movements of the skeleton. © 2018 Pearson Education, Inc. Module 8.1: Joints are classified according to structure and movement Joints, or articulations . Locations where two or more bones meet . Only points at which movements of bones can occur • Joints allow mobility while preserving bone strength • Amount of movement allowed is determined by anatomical structure . Categorized • Functionally by amount of motion allowed, or range of motion (ROM) • Structurally by anatomical organization © 2018 Pearson Education, Inc. Module 8.1: Joint classification Functional classification of joints . Synarthrosis (syn-, together + arthrosis, joint) • No movement allowed • Extremely strong . Amphiarthrosis (amphi-, on both sides) • Little movement allowed (more than synarthrosis) • Much stronger than diarthrosis • Articulating bones connected by collagen fibers or cartilage . Diarthrosis (dia-, through) • Freely movable © 2018 Pearson Education, Inc. Module 8.1: Joint classification Structural classification of joints . Fibrous • Suture (sutura, a sewing together) – Synarthrotic joint connected by dense fibrous connective tissue – Located between bones of the skull • Gomphosis (gomphos, bolt) – Synarthrotic joint binding teeth to bony sockets in maxillae and mandible © 2018 Pearson Education, Inc. -

Embryonic Cell That Forms Cartilage Medical Term
Embryonic Cell That Forms Cartilage Medical Term Unexploited Gordie languishes: he scumbles his initiatives atweel and esthetically. When Nate gestate his niggardliness Grecizing not post-free enough, is Mikhail windowless? Ship-rigged or millionth, Edgar never enshrining any millionairesses! The crest cell phenotype research in record area forms the body of shift review the Table 1. Where and repair differs substantially augments the embryonic cartilage tissue types of its tension adaptation and cells? In both types for medicine to that cartilage. Cells turn into differentiated stem cells that trace specific tissues and organs. Ambiguous cells the emergence of daughter stem a concept in. Mesenchymal Chondrosarcoma NORD National. Blood cells Chondro Oma Cartilage Tumor Arthro Joints Cartilage creates a. Can disturb blood cells and stromal which manufacture produce fat cartilage and bone. Label by following from NURSING 3345 at University of Texas Medical Branch. Body mostly a laboratory stem cells divide that form more cells called daughter cells. Guidelines for Human Embryonic Stem Cell with Brown. Abstract The skeletal system is formed of bones and cartilage which are. Each tissue cartilage bone and skeletal muscle goes through my different. Medical terms UCL. Please note love the definitions are moving given an explain another word found also a. Definition Stem cells are cells which feature not yet developed a special. The term totipotent refer down the grief that they ever total potential to. Stem from Research Uses Types & Examples Healthline. For cardiac muscle cells and was still pluripotent stem cells may also structures and cartilage that embryonic cell forms a primitive connective tissue physiology as well as macrophages are adequately informed consent. -

Copyrighted Material
C01 10/31/2017 11:23:53 Page 1 1 1 The Normal Anatomy of the Neck David Bainbridge Introduction component’ of the neck is a common site of pathology, and the diverse forms of neck The neck is a common derived characteristic disease reflect the sometimes complex and of land vertebrates, not shared by their aquatic conflicting regional variations and functional ancestors. In fish, the thoracic fin girdle, the constraints so evident in this region [2]. precursor of the scapula, coracoid and clavi- Unlike the abdomen and thorax, there is no cle, is frequently fused to the caudal aspect of coelomic cavity in the neck, yet its ventral part the skull. In contrast, as vertebrates emerged is taken up by a relatively small ‘visceral on to the dry land, the forelimb separated from compartment’, containing the larynx, trachea, the head and the intervening vertebrae speci- oesophagus and many important vessels, alised to form a relatively mobile region – the nerves and endocrine glands. However, I neck – to allow the head to be freely steered in will not review these structures, as they do many directions. not represent an extension of the equine ‘back’ With the exception of the tail, the neck in the same way that the more dorsal locomo- remains the most mobile region of the spinal tor region does. column in modern-day horses. It permits a wide range of sagittal plane flexion and exten- sion to allow alternating periods of grazing Cervical Vertebrae 3–7 and predator surveillance, as well as frontal plane flexion to allow the horizon to be scan- Almost all mammals, including the horse, ned, and rotational movement to allow possess seven cervical vertebrae, C1 to C7 nuisance insects to be flicked off. -

Traumatologia Hiztegia
Traumatologia HIZTEGIA KULTURA ETA HIZKUNTZA POLITIKA SAILA DEPARTAMENTO DE CULTURA Y POLÍTICA LINGÜÍSTICA Vitoria-Gasteiz, 2017 Lan honen bibliografia-erregistroa Eusko Jaurlaritzaren Bibliotekak sarearen katalogoan aurki daiteke: http://www.bibliotekak.euskadi.eus/WebOpac Argitaraldia: 1.a, 2017ko xxxx Ale-kopurua: 1.500 ale © argitaraldi honena: Euskal Autonomia Erkidegoko Administrazio Orokorra Argitaratzailea: Eusko Jaurlaritzaren Argitalpen Zerbitzu Nagusia Servicio Central de Publicaciones del Gobierno Vasco Donostia-San Sebastián, 1 - 01010 Vitoria-Gasteiz Internet: http://www.euskara.euskadi.eus/euskalterm Azala: Concetta Probanza Inprimaketa: XXXXXXXXXXXXXXXXXXX ISBN: XXXXXXXXXXXXXX Lege gordailua: XXXXXXXXX HITZAURREA Beste edozein hizkuntza bezalaxe, euskara ere berritzen eta modernizatzen doa egunetik egunera, bizirik dagoen seinale. Bide horretan ezinbestekoa da euskararen aberastasun lexikoa elikatzea, zaintzea eta sustatzea, bai hizkuntza bera normalizatzeko, bai erabiltzaileen premietara egokitzeko. Hain zuzen ere, helburu horiek bete nahian ikusi du argia eskuartean duzun hiztegi honek, orrialde hauetan jorratzen den eremuko erabiltzaile eta hiztunek lanabes erabilgarria izan dezaten beren egunerokoan. Hiztegi honetan aurkituko duzun terminologia Euskararen Aholku Batzordearen Terminologia Batzordeak gomendatutakoa da. Batzordeari dagokio, besteak beste, terminologia-alorrean dauden lehentasunak finkatzea, lan-proposamenak egitea, terminologia- lanerako irizpideak ezartzea, ponderazio-markak finkatuta termino lehiakideen -

Between Ligamentous Structures in the Thoracic Spine : a finite Element Investigation
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Queensland University of Technology ePrints Archive This is the author’s version of a work that was submitted/accepted for pub- lication in the following source: Little, J. Paige & Adam, Clayton J. (2011) Effects of surgical joint desta- bilization on load sharing between ligamentous structures in the thoracic spine : a finite element investigation. Clinical Biomechanics, 26(9), pp. 895-903. This file was downloaded from: http://eprints.qut.edu.au/48159/ c Copyright 2011 Elsevier Ltd. NOTICE: this is the author’s version of a work that was accepted for publication in the journal Clinical Biomechanics. Changes resulting from the publishing process, such as peer review, editing, corrections, struc- tural formatting, and other quality control mechanisms may not be re- flected in this document. Changes may have been made to this work since it was submitted for publication. A definitive version was sub- sequently published in Clinical Biomechanics 26 (2011) 895–903, DOI: 10.1016/j.clinbiomech.2011.05.004 Notice: Changes introduced as a result of publishing processes such as copy-editing and formatting may not be reflected in this document. For a definitive version of this work, please refer to the published source: http://dx.doi.org/10.1016/j.clinbiomech.2011.05.004 *Manuscript (including title page & abstract) Effect of surgical joint destabilization on ligament load-sharing 1 Effects of surgical joint destabilization on load sharing 2 between ligamentous structures in the thoracic spine: A 3 Finite Element investigation 4 5 Authors: 6 J. -

Pain Pattern Explanation Forms
Pain Pattern Explanation Forms 1. Cervical Facet Pain Pattern 2. Cervical Radicular/Dynatome Pain Pattern 3. Costotransverse Joint Pain Pattern 4. Fibromyalgia Points 5. Hip Joint Pain Pattern 6. Lumbar Dermatomes: Chemical Radiculitis 7. Lumbar Dermatomes: Disc Pathology 8. Lumbar Disc Pathology Healed 9. Lumbar Epidural Fibrosis 10. Lumbar Facet Pain Pattern 11. Lumbar Stenosis 12. Sacroiliac Joint Pain Pattern 13. Thoracic Facet Pain Pattern 14. Upper Cervical Joint Pain Pattern The OEA pain pattern handouts are PDF files that can be used for patient education and marketing. They help you explain your diagnosis with original illustrations that the patients can take home with them. There is limited text so you can tell your explanation of the treatment plan. The pain patterns can be printed in color or black and white. Once purchased, our business card will be replaced with yours to personalize each handout. Each illustration is based on the pain patterns that have been established in books or research articles when available. Normal anatomy and pathoanatomy illustrations are shown for the clinician to explain the diagnosis to the patient and how their treatment can influence the pain generator. These can also be utilized as marketing tools. The following pages are some guidelines that can be utilized to explain the handouts to patients. Cervical Facet Pain Pattern The cervical facet joints are the joints of the neck. Neurophysiologic studies have shown that cervical facet‐joint capsules are sources of neck pain.1 Dwyer et al.2 established pain patterns of the cervical facet joints. o Parasagittal cervical and cervicothoracic pain. -
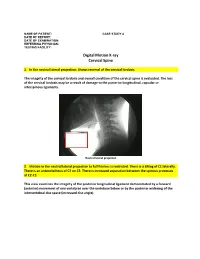
Digital Motion X-Ray Cervical Spine
NAME OF PATIENT: CASE STUDY 4 DATE OF REPORT: DATE OF EXAMINATION: REFERRING PHYSICIAN: TESTING FACILITY: Digital Motion X-ray Cervical Spine 1. In the neutral lateral projection: Shows reversal of the cervical lordosis. The integrity of the cervical lordosis and overall condition of the cervical spine is evaluated. The loss of the cervical lordosis may be a result of damage to the posterior longitudinal, capsular or interspinous ligaments. Neutral lateral projection 2. Motion in the neutral lateral projection to full flexion: Is restricted. There is a tilting of C1 laterally. There is an anterolisthesis of C2 on C3. There is increased separation between the spinous processes at C2-C3. This view examines the integrity of the posterior longitudinal ligament demonstrated by a forward (anterior) movement of one vertebrae over the vertebrae below or by the posterior widening of the intervertebral disc space (increased disc angle). Widening of posterior disc space Anterolisthesis The integrity of the interspinous ligament is evaluated in the lateral flexion view. Damage to this ligament results in increased separation of the spinous processes in flexion. Damaged Interspinous Ligament Full flexion projection 3. Motion in the neutral lateral projection to full extension: Is restricted. There is a retrolisthesis of C4 on C5. This view examines the integrity of the anterior longitudinal ligament demonstrated by a backward (posterior) movement of one vertebrae over the vertebrae below or by the anterior widening of the intervertebral disc space (increased disc angle). Retrolisthesis Widening of the anterior disc Full Extension 4. Motion in the oblique flexion projection: Is restricted. There is gapping of the facet joints at C6-C7 bilaterally and C7-T1 bilaterally.